


Abstract
PURPOSE Negative attitudes and beliefs about depression treatment may prevent many young adults from accepting a diagnosis and treatment for depression. We undertook a study to determine the association between depressive symptom severity, beliefs about and attitudes toward treatment, subjective social norms, and past behavior on the intent not to accept a physician’s diagnosis of depression.
METHODS We conducted a cross-sectional study of 10,962 persons aged 16 to 29 years who participated and had positive screening results on the Center for Epidemiologic Studies Depression (CES-D) score in an Internet-based public health depression screening program. Participants reported whether they would accept their physician’s diagnosis of depression. Based on the theory of reasoned action, we developed a multivariate model of the factors that predict intent not to accept a diagnosis of depression.
RESULTS Twenty-six percent of the participants stated their intent not to accept their physician’s diagnosis of depression. Disagreeing that medications are effective in treating depression (strongly disagree, odds ratio ( OR ) = 6.5, 95% confidence interval (CI), 4.6–9.3), that there is a biological cause for depression (strongly disagree, OR = 1.9, 95% CI, 1.3–2.7), and agreeing that you would be embarrassed if your friends knew you had depression were associated with the intent not to accept a diagnosis of depression (strongly agree, OR = 2.3, 95% CI, 1.8–2.9). Beliefs and attitudes, subjective social norms, and past behavior explained most of the variance in this model (84%).
CONCLUSIONS Negative beliefs and attitudes, subjective social norms, and lack of past helpful treatment experiences are associated with the intent to not accept the diagnosis of depression and may contribute to low rates of treatment among young adults.
INTRODUCTION
Twenty-five percent of young adults will experience a depressive episode by age 24 years, the highest incidence rate of any adult age-group.1–,3 Although depression during this critical period may increase the likelihood of substance abuse, impair work and relationship function, and negatively influence an individual’s subsequent development,1,4–,11 fewer than 20% of young adults with depression receive high-quality care.12
Lack of health insurance coverage and affiliation with a primary care physician do not fully explain these low treatment rates.13,14 Obtaining treatment for depression is a multistage process that includes self-evaluation of need for care, seeking services, and finally accepting a diagnosis and treatment for the disorder, which is substantially influenced by patient attitudes.15,16 Patient reluctance to accept diagnosis and treatment for depression has been identified by primary care physicians as a major barrier to implementing evidence-based treatment for depression17 and may be associated with poor quality of care and outcomes.18–,24 Why patients refuse the diagnosis and treatment for depression remains poorly understood, however.
The theory of reasoned action, which has been used to predict a variety of health behaviors, provides a theoretical framework for understanding why many patients will not accept their physician’s diagnosis of depression.25–,27 According to the theory of reasoned action, intention is the critical determinant of behavior. Intention is determined by beliefs and attitudes about treatment behaviors (eg, medication efficacy and adverse effects), subjective social norms (eg, concern with regard to family opinions), past behavior (eg, past treatment), perceived behavioral control (eg, theory of planned behavior), and self-efficacy.28 The balance of favorable and unfavorable attitudes, subjective social norms, beliefs about control and self-efficacy, and past behavior will determine intention, which in turn leads to action.28,29 Intentions measured close to the actual behavior (in both time and place) strongly predict action.29
Internet surveys are a cost-effective way to obtain information from non–clinic-based populations, such as those who may be seeking or considering care but are not yet in treatment.30,31 Seventy-five percent to 80% of adolescents and young adults have Internet access and use the Internet to search for health information, usually in the early stages of care seeking (ie, considering seeking or accepting treatment).32–,35 In this study, using results from an Internet survey of 10,962 young adults, we developed a multivariate model of intent to not accept a diagnosis of depression, based on the theory of reasoned action as revised by Howland and Hagger27,28 (Figure 1⇓). As we measured intention using the Internet in circumstances separate from possible action, we use the term intent to describe our outcome variable.
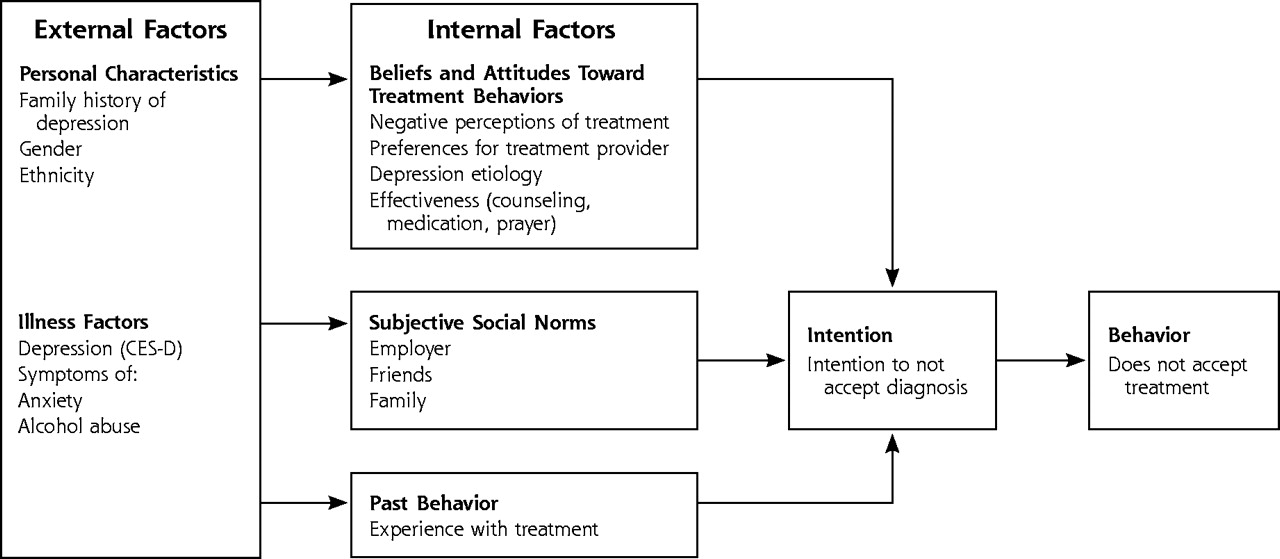
Theory of reasoned action and intention not to accept the diagnosis of depression.
Theory of reasoned action adapted from: Hagger MS, Chatzisarantis NL, Biddle, SJ. A meta-analytic review of the theories of reasoned action and planned behavior in physical activity; predictive validity and the contribution of additional variables. OpenUrlPubMed28; and Howland MJ. Examining the decision to seek professional psychological help; a comparison of attribution and attitude theory in predicting help-seeking intention using the theory of reasoned action. U Illinois at Urbana-Champaign, Ill; 1997.27
METHODS
Study Design
This study is a cross-sectional analysis of 10,962 young adults who completed an Internet-based screening test for depression between March 1999 and March 2000 on a major online health portal (Intelihealth [www.inte-lihealth.com], owned by US Aetna/Healthcare). Based on Zip codes, this database was subsequently cross-referenced with census information. To better understand the comparability of this sample to patients seen in primary care, we compared those of the Internet sample with those of a primary care sample of young adults (the Quality Improvement in Depression Study[ QID]).36,37
Internet users could access the Web site directly at http://www.Intelihealth.com/ depression test, or by entering “depression test” into any search engine or through multiple direct links from other organizations.38 The Web site invited participants to “take a depression assessment” and provided participants with an assessment of their likelihood of having major depression based on their Center for Epidemiologic Studies Depression (CES-D) score: <16, low; 17 to 22, moderate; and >22, high probability.39,40 In population screening, the CES-D cutoff score of 16 has sensitivity ranges of 86% to 100% and specificity ranges of 53% to 84%.38,39,41–,45 Previous work describes the development of this Internet screening test and the selection of cutoff values for the CES-D scores.38
The Web site asked participants to complete a questionnaire concerning their beliefs and attitudes. Also, the Web site provided feedback similar to advice that is often provided after completing a depression screening questionnaire. Participants with a moderate or high probability of having depression were advised to “see a health professional to confirm the diagnosis and discuss what treatment might be best” and that “a delay in treatment could be dangerous.” Participants were also cautioned that having positive screening results for depression was not equivalent to a diagnosis of depression (“about one quarter of individuals who score high are found not to have depression”).43 The Web site also sought to dispel common concerns about treatment.
Study Population and Eligibility
We included only those participants with a moderate or greater likelihood of having major depression (CES-D score >16). We excluded those who either reported the diagnosis of bipolar disorder (mania), symptoms consistent with this diagnosis, or treatment with lithium (n = 329). We did not, however, exclude individuals with symptoms in the last 4 weeks suggestive of other common mental disorders that often co-occur with depression (ie, generalized anxiety disorder, panic disorder, and alcohol abuse).1,8 No personal identification information was collected. The Johns Hopkins University School of Medicine Institutional Review Board approved this study.
Dependent Variable
The main outcome variable, “intent not to accept a diagnosis of depression,” was constructed from the response to the question: “If my doctor told me I had depression, I could accept that.” The participants responded with their level of agreement using a Likert-style scale consisting of strongly agree, agree, neither agree nor disagree, disagree, and strongly disagree. We created a dichotomous variable. All participants who disagreed, strongly disagreed, or neither agreed nor disagreed were considered to have the intent not to accept a diagnosis of depression. We included those who neither agreed nor disagreed as having intent to not accept a depression diagnosis because attitude theory suggests that such individuals would be unlikely to take action and accept treatment.46 All those who agreed or strongly agreed were considered to have the intent to accept a diagnosis of depression. Intent not to accept a diagnosis of depression was strongly associated with having had no mental health services visits and not having received treatment with antidepressant medication in the previous 6 months (odds ratio [OR] = 4.5, 95% confidence interval [CI], 1.4–15.0, vs OR = 1.0 for intent to accept the diagnosis of depression) in the baseline survey of the comparison primary care sample.
Independent Variables (Internal Factors)
Beliefs and Attitudes, Social Norms
The beliefs and attitudes towards treatment behaviors (“beliefs and attitudes”) and subjective social norm (“social norms”) items used in this study were developed using focus group methods and were adapted post hoc to the theory of reasoned action model.36,47,48 Participants rated their agreement with several beliefs and attitudes, and social norm statements, using the same Likert scale used for the dependent variable. We constructed indicator variables for responses on the Likert scale for beliefs and attitudes: “biological changes in the brain cause depression,” “some medications are effective in treating depression,” “counseling is as effective as medication,” “prayer can heal depression,” “medications are addictive,” “counseling brings up bad feelings,” “prefer same gender provider,” and “prefer same race provider,” and social norms with regard to treatment: “my employer should not know,” “I would be embarrassed if my friends knew,” and “my family would be disappointed.” Similarly, we created indicator references for treatment type: counseling, medication, or neither. Treatment options were defined for the preference item as “antidepressant medication for 6 to 9 months” or “counseling weekly for 3 months.”
Past Treatment Behavior (Past Behavior)
We constructed indicator variables to describe each type of possible treatment experience in terms of form of treatment (medication or counseling) and whether each form of treatment was helpful. We used the available responses from 4 separate items of “ever taken medication for depression,” “ever had counseling for depression,” “how helpful was medication,” and “how helpful was counseling.” From these responses, we constructed the following mutually exclusive categories to describe type of treatment (whether the participant had experienced medication or counseling or both) and helpfulness of each treatment: (1) no past treatment, (2) both treatments not helpful, (3) medication helpful, (4) medication not helpful, (5) counseling helpful, (6) counseling not helpful, (7) medications helpful/counseling not helpful, and (8) counseling helpful/medications not helpful, and (9) both treatments helpful. Helpfulness was rated as not at all, not very, somewhat, and very. All responses of somewhat or very were characterized as helpful in the construction of the indicator variables. Participants who reported only 1 form of treatment were classified in either the medication or counseling groups, while those who had experienced both forms of treatment were placed in a combination group. For example, a participant who reported that medication treatment was helpful, but counseling was not, would be classified “medication helpful/counseling not helpful,” but not in the “medication helpful” or “counseling not helpful groups.”
Covariates (External Factors)
Personal Characteristics
The model included sex, ethnicity, and family history of depression. With regard to family history, participants were asked whether “their mother, father, sisters, or brother previously had depression that lasted more than 4 weeks or had been treated for it.” Our chosen young adult age range (ages 16 to 29 years) was used as a distinct category on this Web site and was not further defined.
Illness Factors
We examined the effects of depressive symptom severity (total CES-D score) on intent not to accept a diagnosis of depression. CES-D score was incorporated as a continuous variable adjusting for its non–log-linear relationship with the outcome variable. We reported results for CES-D scores using indicator variables for score quartiles for ease of interpretation and because the quartiles closely approximated the nonlinear relationship between the outcome variable and CES-D score. Participants were asked about the presence (yes/no) in the past 4 weeks of symptoms of panic disorder (“sudden anxiety, heart pounding, short of breath”), generalized anxiety disorder (“very anxious, nervous, or panicky”), and alcohol abuse (“drinking >5 drinks/day” and “drinking more than usual”).
Statistical Analysis
As appropriate, we used Pearson χ2 or Fisher exact tests to compare our Internet sample with the primary care sample. In our Internet sample, we used a 2-step multivariate logistic regression model to evaluate the relationship between the independent variables and intent not to accept a diagnosis of depression.49 In the first step, we screened all the independent variables in bivariate linear regression analyses for statistical significance. Those with P values <.05 were advanced to the multivariate model. We evaluated possible interactions between past behavior and beliefs and attitudes, social norms, and the outcome variable using tests of interaction and stratified analyses. We calculated the proportion of model variance explained by each group of factors and conducted sensitivity analyses and goodness of fit tests.
RESULTS
Study Population
As displayed in Table 1⇓, we compared our Internet sample with a probabilistic representative primary care sample. Our Internet sample had similar depressive symptom levels, whether measured by 2 different commonly accepted cutoff scores or by a mean score. With regard to treatment history, included as one of our internal factors (Figure 1⇑), our Internet sample had a greater percentage of persons who never had any depression treatment, suggesting the possible importance of our design of using the anonymous Internet medium for depression screening. Our Internet sample differed by having lower percentages of minority groups. Also, as shown in Table 2⇓, our Internet sample included a strong belief in a biological cause and medical treatment approach for depression. With regard to subjective social norms, 67% believed that their employer should not know about their depression. Nearly one half the participants reported a family history of depression.
Comparison of Sample Characteristics between the Internet Sample and Primary Care Sample
Responses to Beliefs and Attitudes Toward Treatment and Subjective Social Norms Items
External Factors
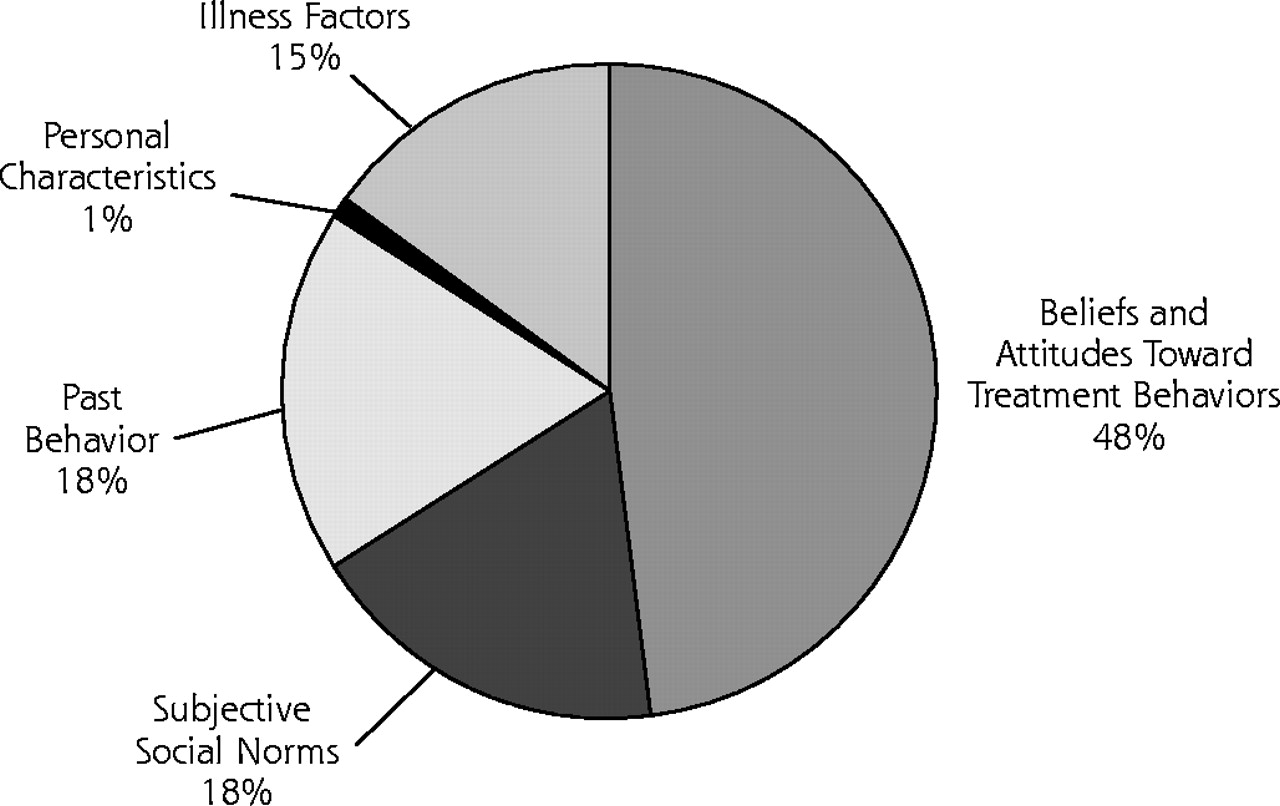
External factors accounted for 16% of model variance (Figure 2⇓). As shown in Table 3⇓, in bivariate analyses, male sex, Asian-American ethnicity, family history of depression, CES-D score, and presence of either generalized anxiety or panic symptoms predicted the intent not to accept the diagnosis of depression. In the multivariate analyses, only male sex and CES-D scores remained predictive, where the lower the depression level, the greater the intent not to accept the diagnosis of depression. The addition of past behavior (treatment) and family history of depression explained most of the loss of association in the multivariate model. The addition of social norms variables to the model explained the loss of association between no family history of depression and the outcome variable, from the bivariate to the multivariate model.
Multiple Logistic Regression Analysis of Personal Characteristics and Illness Factors (External Factors) and Intent Not to Accept a Physician’s Diagnosis of Depression

Percentage of theory of reasoned action model variance explained by model factors.
Note: Percentage of explained model variance calculated from the pseudo-R2 contributed by each group of variable defined by the theory of reasoned action.
Internal Factors
Internal factors accounted for 84% of model variance (Figure 2⇑). As displayed in Table 4⇓, in the bivariate model, all the beliefs and attitudes, social norms, and past treatment behavior variables predicted the intent not to accept the diagnosis of depression. In the multivariate model, adjusting for a variety of variables including CES-D score, all remained predictive with the exception of the belief and attitude variable of “medications are addictive,” the social norm variable of “employer should not know,” the past treatment behavior variables of those who had received both medication and counseling treatment and rated one type as ineffective, and family history of depression. Those who strongly disagreed with the belief and attitude variable of “medications are effective” had odds ratios as high as 11.22. Removal of past treatment behavior variables from the model only minimally effected the relationship between the belief and attitude variables and intent. No interactions existed for belief and attitude, social norm, and past treatment behavior variables and intent.
Multiple Logistic Regression Analysis of Attitudes Toward Treatment Behaviors and Subjective Social Norms (Internal Factors) and Intent Not to Accept a Physician’s Diagnosis of Depression
DISCUSSION
Negative beliefs and attitudes and social norms, a variety of past treatment experiences, and low depressive symptom severity are the most important predictors of the intent not to accept a diagnosis of depression in young adults. Those with beliefs and attitudes of disagreeing with a biological approach to depression development and treatment are most likely to express intent not to accept a physician’s diagnosis of depression.
This study uses an established behavioral theory to improve our understanding of the contribution of key beliefs and attitudes, subjective social norms, and past treatment behavior to help explain why certain young adults do not accept a depression diagnosis and are reluctant to obtain depression treatment.24,50–,54 Our results of a preference for counseling resulting in a greater likelihood of not accepting a depression diagnosis may help explain why many primary care patients remain reluctant to accept counseling treatments.16 Behaviorally based treatment used in counseling may be less acceptable than biological treatment approaches.27,55 Also, the protective effect of a family history of depression for accepting a depression diagnosis may be related to the reduction of depression stigma by contact with affected family members.56,57
The principal limitations of this study in terms of internal validity are the lack of a close temporal relationship between expressing intent and performance, information on perceived behavioral control, current treatment status, and a confirmed diagnosis of depression. Although we do not know how participants would respond to a physician’s diagnosis of depression, intent not to accept the diagnosis of depression was associated with not having obtained treatment for depression in the primary care sample.36,37 In developed countries, beliefs and attitudes toward treatment, rather than access to care, may be the critical determinants of mental health help-seeking behavior.14,58–,60 In a previous study we found that adjustment for perceived behavioral control did not change the relationship between beliefs and attitudes and mental health help seeking in a primary care sample.16 Although we do not know which participants were currently seeking treatment, elimination of all those participants who reported previous treatment did not change the relationships between the internal factors and the intent variable. Although we do not know which participants met the criteria for a depressive disorder, we did adjust for that likelihood in our model by including the total CES-D score and symptoms of other mental disorders. We acknowledge that there could be certain additional beliefs and attitudes that may be relevant, too (eg, trust in providers, self-efficacy, self-esteem, and psychological mindedness).
With regard to external validity, our Internet participants had similar depressive symptom severity but contained higher proportions of whites and men than the comparison primary care sample. The Internet participants had less exposure to treatment than those in the primary care sample and most closely resembled those who did not seek treatment in the primary care sample. Such individuals are not often present in convenience clinic samples. Recruiting a sufficiently large number of symptomatic, untreated young adults to perform this multivariate analysis using probabilistic sampling methods would be difficult and prohibitively expensive.
These results have implications for general medical practice and health care policy. Our study suggests that behavioral theories can be used to develop models to understand and deconstruct the reasons why so few young adults seek and accept care for depression. Future studies should focus on understanding how physicians facilitate effective mental health care by focusing on specific patient concerns. Policy makers should consider improved reimbursement to primary care physicians for visits during which they negotiate diagnosis and treatment plans with depressed patients. Reimbursement would provide an incentive for these physicians to spend the time needed to diagnose and manage depression appropriately, which would likely increase patients’ confidence in evidence-based treatments and their receipt of guideline-concordant depression care.
Acknowledgments
The assistance of Donica E. Van Voorhees, MTS, in reviewing this manuscript is gratefully acknowledged.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This work was supported by NRSA grant T32PE10025
- Received for publication December 16, 2003.
- Revision received September 22, 2004.
- Accepted for publication October 20, 2004.
- © 2005 Annals of Family Medicine, Inc.
REFERENCES





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Proportion Of Antidepressants Prescribed Without A Psychiatric Diagnosis Is Growing
- Cardiovascular risk factors associated with lower baseline cognitive performance in HIV-positive persons
- In This Issue: Bursting the Bubble on Chronic Disease Management, the Meaning of Healing, PBRN Methods Supplement, and the Annals' 2-Year Anniversary
- Stimulus, Response, Interpretation
- In This Issue
- Depression Research in Primary Care: Pushing the Field Forward