


Abstract
PURPOSE We compared the effectiveness of 2 physical activity prescriptions delivered in primary care—the standard time-based Green Prescription and a pedometer step-based Green Prescription—on physical activity, body mass index (BMI), blood pressure, and quality of life in low-active older adults.
METHODS We undertook a randomized controlled trial involving 330 low-active older adults (aged =65 years) recruited through their primary care physicians’ patient databases. Participants were randomized to either the pedometer step-based Green Prescription group (n = 165) or the standard Green Prescription group (n = 165). Both groups had a visit with the primary care practitioner and 3 telephone counseling sessions over 12 weeks aimed at increasing physical activity. Outcomes were the changes in physical activity (assessed with the Auckland Heart Study Physical Activity Questionnaire), blood pressure, BMI, quality of life (assessed with the 36-Item Short Form Health Survey), physical function status (assessed with the Short Physical Performance Battery), and falls over a 12-month period.
RESULTS Of the patients invited to participate, 57% responded. At 12 months, leisure walking increased by 49.6 min/wk for the pedometer Green Prescription compared with 28.1 min/wk for the standard Green Prescription (P=.03). For both groups, there were significant increases across all physical activity domains at 3 months (end of intervention) that were largely maintained after 12 months of follow-up. BMI did not change in either group. Significant improvements in blood pressure were observed for both groups without any differences between them.
CONCLUSIONS Pedometer use resulted in a greater increase in leisure walking without any impact on overall activity level. All participants increased physical activity, and on average, their blood pressure decreased over 12 months, although the clinical relevance is unknown.
- physical activity
- primary health care
- randomized controlled trial
- older adults
- sedentary lifestyle
- health promotion
- practice-based research
INTRODUCTION
Older adults are at particular risk of low levels of physical activity,1 and increasing physical activity reduces risks of cardiovascular disease, type 2 diabetes, some cancers, obesity, injury, osteoporosis, and depression.2 Participation in physical activity also improves psychological functioning,3–5 quality of life, and independent living for older people.6 Despite mounting evidence of the benefits of activity, population-level data show adults aged 80 years and older to be 7 times more likely to be inactive than those aged 60 to 64 years.7
In New Zealand, the Green Prescription is a nationally supported and funded intervention delivered through primary care to increase physical activity. It involves an initial prescription of physical activity by a primary care physician, followed by telephone counseling from trained physical activity counselors (in government-funded, regional sport, and physical activity organizations), and is based largely within a framework of motivational interviewing and goal setting. The intervention uses time-based activity goals to increase physical activity to meet the New Zealand national guidelines of 30 minutes of moderate activity on most, if not all, days of the week.8 Research has shown the Green Prescription to be effective in increasing physical activity in the adult9 and older adult10 populations, and also to be cost-effective.11,12 In a cluster-randomized trial, the group who received the Green Prescription increased leisure activity by 34 min/wk more than the control group.9 For the older subpopulation of that trial (aged 65–79 years), leisure time moderate activity increased by 40 min/wk.10 Only about 10% of people who participate in the Green Prescription have an increase in activity10; thus, ways to involve more older people in regular activity are clearly needed. Accumulated incidental physical activity may be important to achieving health benefits in older adults,13 and the use of pedometers (as a motivational tool) is an effective way of maintaining physical activity levels.14 In previously inactive middle-aged women, pedometers have been found to increase walking compared with advice to spend a specific amount of time in this activity15; however, health outcomes related to this increase were not assessed.
Based on an overall goal of improving this national scripting program, the Healthy Steps trial reported here had the aim of comparing the effectiveness of a pedometer-based Green Prescription with that of the proven time-based (standard) Green Prescription.9,10 The trial also sought to investigate the effects of the interventions on blood pressure, body mass index (BMI), functional status, and health-related quality of life.
METHODS
Trial Design
We used a randomized controlled trial to test the effect of a pedometer-based Green Prescription on physical activity and a range of health outcomes in low-active older adults. The intervention group was compared with a group assigned to the standard Green Prescription. Methods for this trial have been described elsewhere,16 as have details of its cost-effectiveness.17 The trial is reported according to the Consolidated Standards of Reporting Trials (CONSORT) statement.18 The trial protocol was approved by the New Zealand Ministry of Health’s Health and Disability Ethics Committee in 2005.
Participants and Recruitment
We recruited participants through 17 primary care physicians from 10 general practices in Auckland, New Zealand. Inclusion criteria included an age of 65 years or older, ability to communicate in English, ability to give informed consent, residing in the community, ability to walk, and freedom from health conditions that contraindicate participation in physical activity. Exclusion criteria included visual impairment that would make it impossible to read a pedometer screen. Physicians screened a list of all their patients for eligibility, first using the 65 years and older criterion, and then excluding only those within this age range who did not meet the above criteria. Physicians sent an invitation to all eligible patients in each practice. Those who replied were contacted by telephone and screened for physical activity level with the question “As a rule, do you do at least half an hour of moderate or vigorous exercise (such as walking or a sport) on 5 or more days of a week?” (The positive predictive value of this question is 81% for identifying “less active” adults.19) We used the Physical Activity Readiness Questionnaire (PAR-Q)20 to screen for health conditions contraindicating physical activity. Clearance from their usual physician was obtained for those who had a positive result on the PAR-Q, with no one eventually excluded. A home visit was arranged to obtain written informed consent, assess baseline measures, and arrange an appointment with their physician for commencement of the intervention. In addition, participants were given a calendar for recording any falls and injuries. Recruitment took place between July 2006 and December 2007.
Sample size calculation used means, standard deviations, and changes from baseline in previous trials.9 A sample size of 137 per group would have at least 80% power at the .05 level of significance to detect a true difference in the change between the 2 groups of 60 minutes of moderate physical activity per week, 5 points on the 36-Item Short Form Health Survey (SF-36) general health domain, and a detectable 15% of participants meeting physical activity guidelines. Given an estimated attrition of 20% over 12 months, 165 participants were needed in each group.
Randomization and Blinding
Participants were randomized individually after baseline assessment. Randomization was blocked, and the lists were generated by an independent member of the research team. Physicians were notified of a participant’s group allocation before the participant received the physical activity prescription. For the 31 couples recruited, individuals in the couple were allocated to the same intervention. All outcome measures were assessed by a researcher blinded to group allocation.
Measures
Outcomes were ascertained during home visits. All outcome measures were obtained at 3 to 4 months (end of the intervention) and at 12 months (follow-up). All questionnaires were provided in English. Demographics (age, sex, ethnicity, marital status, education, occupation, and socioeconomic indicators) were collected at baseline.
Outcome variables included physical activity, health-related quality of life, blood pressure, weight, height, functional status, and adverse events (falls and injuries). Physical activity was assessed with the Auckland Heart Study Physical Activity Questionnaire (AHSPAQ),19,21 an instrument validated for use with less active adults in primary care using activity diaries and pedometer readings as comparators.19 The AHSPAQ prompts individuals to recall their physical activity including walking, moderate and vigorous activity, leisure activity, and occupational and domestic activity. Health-related quality of life was assessed with the SF-36 questionnaire.22 Blood pressure was measured 3 times with an electronic sphygmomanometer, and information on use of blood pressure medication was obtained through self-report. We measured weight using electronic scales and height using a portable stadiometer. Physical function was assessed using the Short Physical Performance Battery (SPPB), specifically the gait speed, chair stands, and tandem balance tests.23–25 Data on self-reported adverse events were collected monthly. Blood pressure medications were assessed by self-report at each time point. Self-reported measures of any new illness or life events that had a serious effect on health or ability to do physical activity were collected at the end of intervention and at 12 months.
Interventions
A detailed account of the 2 interventions has been published previously.16 Participants in the pedometer-based Green Prescription group received initial face-to-face advice on engaging in physical activity from their physician that was then followed up by 3 telephone counseling sessions by trained physical activity counselors over 3 to 4 months. Telephone counseling call 1 focused on information provision and goal setting (15–30 minutes), call 2 focused on assessing progress and further goal setting (10–15 minutes), and call 3 provided further encouragement and discussions around relapse prevention (10–15 minutes). All participants took part in all sessions. Goal setting based on steps was used as a main component of this intervention, and participants were encouraged to use their pedometer to monitor steps taken throughout the day. Goals were set by participants as part of their interaction with the physical activity counselor, in which they received guidance on how to set relevant goals based on identified barriers and on factors that enable increasing activity. Individual goals were predominantly based on pursuing activities that increase step counts in an incremental manner over time, and were dependent on identified lifestyle factors, accessibility to facilities, level of mobility, and current level of activity. Some goals were specifically based on engaging in an activity and receiving feedback via the pedometer on step-based gains, whereas other goals were based on increasing the number of steps per day (eg, by 1,000 steps). Examples of goals included walking rather than driving to the shopping center to accumulate 1,500 steps, walking to a friend’s house rather than using the telephone, and participating in an older adult dance activity at the local community center. We did not specifically use the 10,000 steps target used in some other studies.
Participants in the standard Green Prescription group received the same intervention with the exception that counseling focused on accumulating physical activity around time-related goals rather than step-related goals.
Statistical Analysis
We analyzed the differences between the pedometer-based Green Prescription and standard Green Prescription groups in change of outcome variables using a repeated-measures Generalized Estimating Equation (GEE) model with an autoregressive covariance matrix, which computed the observed data as incomplete. Couples were treated as a cluster and, as noted, were randomized together into the same group. The GEE model automatically adjusts for baseline differentials and interpolation of missing data. We adjusted the models for known determinants of physical activity (age, sex, whether partnered, education level, and occurrence of an illness or event that had a serious impact on health or ability to do physical activity), and study design effects (physician and couple cluster). To account for nonnormality of physical activity and BMI data, physical activity minutes were modeled using a negative binomial distribution and BMI was transformed with a logarithmic function. For the analysis of blood pressure data, we included additional covariates of medications for blood pressure, as well as any changes in these medications over the course of the study. All analyses were performed using SAS statistical software, version 9.1.3 (SAS Institute, Inc).
RESULTS
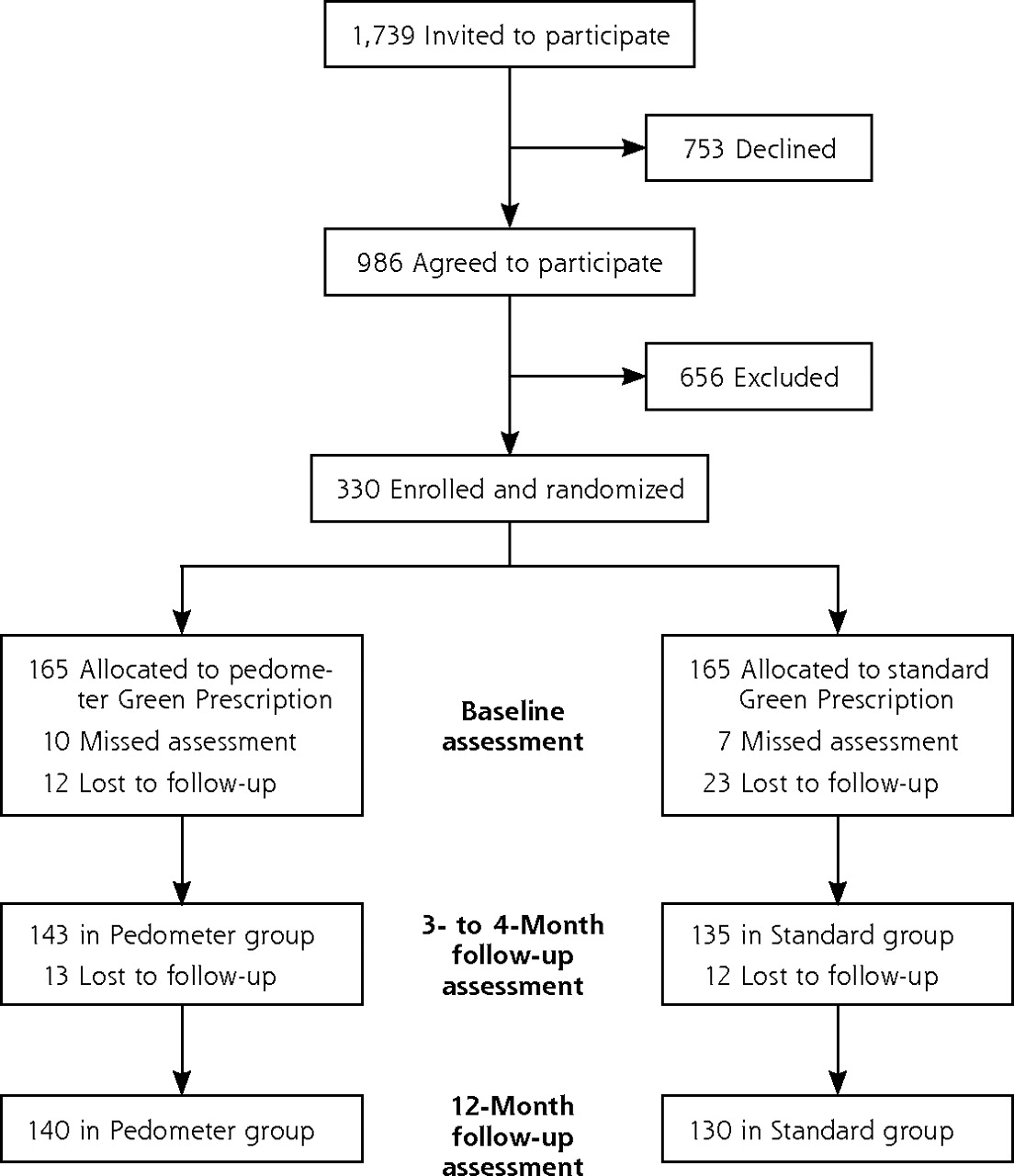
Of 1,739 patients invited by 17 primary care physicians, 986 (57%) agreed to participate. Of these, 656 were excluded because they changed their mind about participation on contact (22%), had participated in a Green Prescription Program in the last 2 years (2%), were too active (40%), or were medically unsuitable for inclusion in the trial (3%). A total of 330 patients were recruited into the trial. At the end of the intervention (3–4 months), 278 remained, and at follow-up (12 months), 270 remained. Reasons for dropping out of the study included death (3 patients), a change in health (14), being too busy or changing one’s mind (31), not receiving any intervention (1), being told by a nurse they were too active for the study (1), traveling (3), moving (4), and being out of contact (3). Figure 1 shows the flow of participants through each stage of the trial.

Flow of participants through each stage of the Healthy Steps trial.
As Table 1 shows, there were no significant differences in participant sociodemographic characteristics between groups at baseline. Table 2 shows results of the GEE repeated measure models for the primary and secondary outcomes. At 12 months, minutes of leisure walking differed significantly between groups (P = .03) over time. Specifically, during the intervention period (3–4 months), the pedometer-based Green Prescription group increased leisure walking by 63.0 min/wk on average, more than double the increase in the standard Green Prescription group of 30.9 min/wk. This initial increase was then followed by a decrease of 13.4 minutes (net overall increase of 49.6 min/wk) for the pedometer-based Green Prescription group at the 12-month follow-up, and a decrease of 2.8 minutes (net overall increase of 28.1 min/wk) for the standard Green Prescription group. No other measures showed a significant between-group differential change over time.
Patient Characteristics at Baseline (N = 330)
Measures of Physical Activity and Other Outcomes by Group and Time Point
All participants increased total walking activity over time. Blood pressure (systolic and diastolic, adjusted for medication for heart conditions and hypertension) decreased within each group over time, with no significant difference between them. There was no significant differential change between the groups in physical function SPPB scores (P = .97) and no change over time (P = .25). Neither group had a change in BMI in this study.
We did not analyze several SF-36 quality of life scores because of moderate to strong ceiling effects. Ceiling effects were observed at baseline for bodily pain (29.3% of participants scored 100%), role physical (61.6%), social functioning (69.2%), and role emotional (87.5%). Those SF-36 quality of life measures that we did analyze (physical functioning, general health, vitality, mental health) improved significantly over time, but with no differential changes between groups.
We assessed falls, with and without injuries, across groups both during the intervention period and at follow-up (for 1 month at 11–12 months). During the 3-month intervention, the proportion of patients reporting at least 1 fall that did not result in injury was similar in the 2 groups (7.9% and 7.3% for the pedometer-based and standard Green Prescription groups, respectively, χ21=0.04, P = .84). At follow-up (11–12 months), fall rates were also low, with no difference between groups (5.7% and 3.1%, respectively, χ21=1.10, P = .29). The 2 groups also had a similar proportion of patients reporting at least 1 fall resulting in injury (5.5% and 8.5% for the pedometer-based and standard Green Prescription groups, respectively, χ21=1.17, P=.28). At follow-up (11–12 months), the rate of such falls was also low, with no difference between groups (2.7% and 2.3%, respectively, χ21=1.08, P=.78).
DISCUSSION
This trial shows a beneficial impact in leisure walking of the pedometer when used as part of the Green Prescription for older adults. Pedometer-based activity counseling appears better than the standard Green Prescription, at least for promoting and maintaining (up to 12 months) leisure walking. Walking behavior increased by 30 min/wk more in the pedometer-based group than in the time-based activity group. Similar increases have been observed in middle-aged women, where those instructed to walk 10,000 steps daily walked more than those instructed to take a brisk 30-minute walk on most days of the week.15 The results of the present trial also suggest that regardless of the type of physical activity goal that is recommended to patients and on which they are counseled, levels increased and were maintained over 12 months. This result supports the findings of other studies of the standard Green Prescription, which demonstrated improvements in physical activity among both adult9 and older adult10 groups.
Pedometers, in this study, likely improved the efficacy of the activity prescription by providing regular objective monitoring and feedback to assist motivation. This function is achieved through participants’ ability to see the number of steps attained through particular activities and throughout the day. It could be that the pedometers encouraged more achievable and sustainable increases in habitual physical activity that are not necessarily supported by a time-based prescription. This finding adds to the positive trials set in primary care9,10 and increases options for physical activity counselors. The cost of a pedometer (NZ$25, US$18.50) makes it an affordable option.
In contrast to other trials of the Green Prescription,9,10 this trial showed reductions of systolic and diastolic blood pressure of 10 and 4.5 mm Hg, respectively, for the whole trial population. Such reductions are unusual in physical activity trials and of major health importance for older people as a subsequent reduction in stroke and myocardial infarction would be expected.26
Our results suggest that pedometer-based Green Prescription may be as effective as the standard Green Prescription in improving blood pressure and total energy expenditure, but because there was no true control group, we cannot be certain. We cannot truly determine whether the improvements in both groups were due to participation in the trial, natural progression of symptoms, or other initiatives in health care or changes in the wider community. This study does support earlier findings that quality of life9,10 and activity levels9,10 improve with the Green Prescription intervention and adds a reduction in blood pressure to the positive impact of activity interventions in low-active older people.
Four further considerations are worthy of discussion when interpreting this trial’s findings. First, we have no data on adherence beyond the 12-month follow-up. This limitation is important as the effects of physical activity on health may be cumulative. Second, the response rate (57%) should be considered in relation to the findings, although such a rate is consistent with our experience in primary care physical activity trials.3,27 Third, despite the sample size calculations, the sample may have been insufficient to detect smaller, but still clinically important, improvements in outcomes. Finally, use of self-reported physical activity could be seen as a limitation in this study; however, the AHSPAQ is valid using pedometer data as the comparator.18
In conclusion, this randomized controlled trial tested 2 types of intervention that appear quite similar, yet approach the goal of increasing physical activity from different angles. One (the pedometer-based Green Prescription) encourages accumulation of habitual activity through the use of a device that provides feedback on steps taken. The other (the standard Green Prescription) encourages achieving national physical activity guidelines through a time-based prescription. Both approaches are popular, so understanding differences in outcomes is important. The use of pedometers led to a greater increase in leisure walking activity than did reliance on only time-based goals (ie, no use of a pedometer). Overall physical activity improved in both groups, as did blood pressure. Incorporating pedometers into the Green Prescription is a useful strategy for consideration in physical activity promotion for older people, and our results suggest that these devices may have a large untapped potential for public health benefit. The findings of this study, combined with the demonstrated cost-effectiveness of the interventions,17 allow health funding agencies to consider the use of such approaches to improve activity levels.
Acknowledgments
We acknowledge and thank the staff and patients at the primary care practices from which participants were recruited.
Footnotes
-
Conflicts of interest: authors report none.
-
Disclaimer: The funders had no involvement in the research design, conduct, or interpretation of results.
-
Previous presentation: Aspects of this work were presented at the American College of Sports Medicine 57th Annual Meeting, Baltimore, MD, June 2010.
-
Trial registration number: Australia and New Zealand Clinical Trials Register ACTRN012606000023550
-
Funding support: The Health Research Council of New Zealand (05/279R) and Sport and Recreation New Zealand funded this trial.
- Received for publication March 4, 2011.
- Revision received August 24, 2011.
- Accepted for publication September 12, 2011.
- © 2012 Annals of Family Medicine, Inc.
References





{kind=link}
Jump to section
Related Articles
Cited By...
- Using Web 2.0 applications to promote health-related physical activity: findings from the WALK 2.0 randomised controlled trial
- Feasibility of a Memory Clinic-Based Physical Activity Prescription Program
- Measurement of physical activity in older adult interventions: a systematic review
- Impact of a 12-week, pharmacist-directed walking program in an established employee preventive care clinic
- In This Issue: From Communities of Solution to Joy