


Article Figures & Data
Figures
- Figure 1
CONSORT diagram.
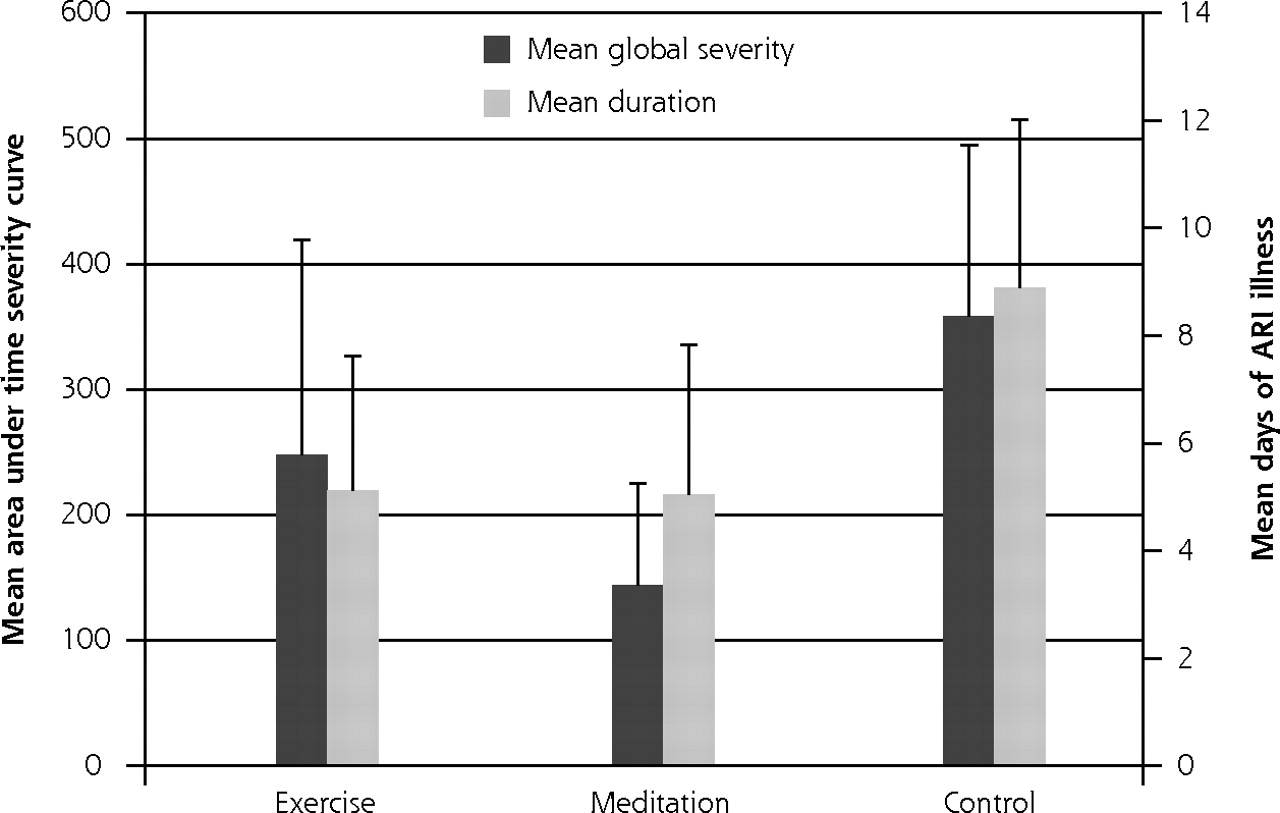
- Figure 2
Primary outcomes: days of acute respiratory infection illness and area-under-curve global severity.
ARI = acute respiratory infection; global severity = area under curve time severity curve, calculated as trapezoidal approximation using daily scores on Wisconsin Upper Respiratory Infection Symptom Severity (WURSS-24) for y-axis and duration of ARI illness as x-axis.
Note: Error bars indicate 95% confi dence intervals.


Tables
Characteristic Exercise Meditationa Control P Value Sample, n 47 51 51 Age, mean y (SD) 59.0 (6.6) 60.0 (6.5) 58.8 (6.8) 0.63 Female, n (%) 39 (83.0) 42 (82.4) 41 (80.4) 0.94 Nonsmokers, n (%) 43 (91.5) 48 (94.1) 48 (94.1) 0.84 Race,b n (%) 3 (6.4) 1(1.9) 2 (3.9) 0.52 Black White, n (%) 43 (91.5) 49 (92.5) 48 (94.1) 0.88 Other, n (%) 1 (2.13) 3(5.7) 1 (2.0) 0.50 Ethnicity non-Hispanic, n (%) 47 (100) 51 (100) 49 (96.1) 0.14 BMI, mean (SD) 29.0 (6.9) 29.0 (6.0) 29.8 (6.8) 0.77 SF-12 physical, mean score (SD) 50.9 (9.3) 50.7 (9.4) 50.0 (9.3) 0.89 SF-12 mental, mean score (SD) 52.3 (6.6) 50.9 (8.6) 51.1 (7.8) 0.62 College graduate or higher, n (%) 27 (57.4) 36 (70.6) 35 (68.6) 0.34 Income >$50,000, n (%) 25 (53.2) 31 (60.8) 29 (56.9) 0.75 Mean scores at baseline, n (SD) Physical health (SF-12) 50.9 (9.3) 50.7 (9.4) 50.0 (9.3) 0.89 Mental health (SF-12) 52.3 (6.6) 50.9 (8.6) 51.1 (7.8) 0.62 Negative emotion (PANAS) 15.2 (5.1) 15.8 (4.0) 14.8 (3.7) 0.45 Positive emotion (PANAS) 36.7 (6.2) 36.2 (6.5) 36.3 (6.6) 0.91 Optimism (LOT) 27.1 (3.4) 27.1 (3.9) 28.3 (3.6) 0.17 Social support (Ryff PR) 44.9 (7.2) 45.4 (6.6) 45.9 (6.3) 0.73 Perceived stress (PSS-10) 11.4 (6.0) 13.0 (4.7) 11.2 (5.4) 0.19 Anxiety (current state) (STAI) 30.7 (9.1) 32.2 (8.1) 29.8 (7.3) 0.31 Sleep quality (PSQI) 4.6 (3.1) 5.1 (2.6) 4.7 (2.5) 0.46 Mindfulness (MAAS) 4.6 (0.7) 4.5 (0.7) 4.6 (0.7) 0.37 Exercise, MET min/wk (IPAQ) 1,214 (1,526) 644 (664) 925 (1,225) 0.06 -
BMI = body mass index (weight/height2); IPAQ = International Physical Activity Questionnaire; LOT = Life Orientation Test; MAAS = Mindful Attention Awareness Scale; PANAS = Positive and Negative Affect Schedule; PSS-10 = 10-item Perceived Stress Scale; PSQI = Pittsburgh Sleep Quality Index; Ryff PR = Ryff’s 9-item Positive Relationships with Others scale; SF-12 = Medical Outcomes Study Short Form-12; STAI = State Trait Anxiety Inventory.
-
Note: P values were calculated by analysis of variance using NCSS 2007, LLC (http://www.ncss.com).
-
↵a Missing information on income from meditation group (n = 2).
-
↵b One person in the meditation group reported 3 racial categories.
-
Between-Group Differences Outcome Exercise (n = 47) Meditation (n = 51) Control (n = 51) Exercise vs Control Meditation vs Control Participants with ARI illness, n (%) or (95% CI) 17 (36) 21 (41) 28 (55) 0.19 (−0.01 to 0.37)
P=.0320.14 (−0.06 to 0.32)
P=.083Number of ARI episodes 26 27 40 Mean global severity score, n (95% CI)a 248 (77 to 419) 144 (62 to 225) 358 (221 to 495) 110 (−105 to 324)
P=.16214 (56 to 372)
P=.0042Total days of ARI illness 241 257 453 Mean ARI illness days, n (95% CI) 5.13 (2.64 to 7.62) 5.04 (2.25 to 7.83) 8.89 (5.76 to 12.02) 3.76 (−0.24 to 7.75)
P=.0323.85 (−0.29 to 7.99)
P=.034Health care visits and work days lost to illness Episodes of missed work, n 21 25 33 Total days missed, n 91.5 99 144.5 Mean missed days, n (95% CI) 1.9 (0.8 to 3.1) 1.9 (0.7 to 3.2) 2.8 (1.5 to 4.2) 0.9 (−0.9 to 2.7)
P=.160.9 (−0.9 to 2.7)
P=.17ARI-related missed days, n (95% CI) 32 16 67 0.11 (−0.01 to 0.24)
P=.0410.30 (0.19 to 0.40)
P <.001Mean ARI-related missed days, n (95% CI) 0.68 (0.1 to 1.2) 0.31 (0.1 to 0.5) 1.31 (0.5 to 2.1) 0.63 (−0.4 to 1.6)
P=.101.0 (0.2 to 1.8)
P=.011Total number of health care visits 116 116 121 Mean health care visits, n (95% CI) 2.5 (1.7 to 3.2) 2.3 (1.6 to 2.9) 2.4 (1.8 to 2.9) −0.1 (−1.0 to 0.8)
P=.420.1 (−0.7 to 0.9)
P=.41ARI-related health care visits, n (95% CI) 15 10 16 0.003 (−0.09 to 0.09)
P=.470.05 (−0.04 to 0.13)
P=.13Mean ARI-related health care visits, n (95% CI) 0.32 (0.14 to 0.49) 0.20 (0.07 to 0.32) 0.31 (0.12 to 0.50) −0.01 (−0.26 to 0.25)
P=.480.11 (−0.11 to 0.34)
P=.15Mean non-ARI-related health care visits, n (95% CI) 2.15 (1.5 to 2.8) 2.08 (1.5 to 2.7) 2.06 (1.5 to 2.6) −0.09 (−0.89 to 0.71)
P=.41−0.02 (−0.80 to 0.76)
P=.48Biomarker and viral identification data from nasal secretions IL-8, mean pg/mL (95% CI)b 694 (484 to 904) 910 (696 to 1,124) 658 (511 to 806) −36 (−282 to 211) −252 (−497 to −6) Neutrophils, mean n/HPF (95% CI) 103.7 (−46.1 to 253.5) 107.9 (23.0 to 192.8) 110.4 (22.9 to 197.9) 6.7 (−150.8 to 164.2) 2.5 (−119.6 to 124.6) Positive for virus, n (95% CI) 8 14 19 0.12 (−0.15 to 0.38) 0.004 (−0.24 to 0.25) Specific viruses (n)c HRV (7) CoV (2) Adv C (1) MPV (1) HRV (10) CoV (3) MPV (1) Flu A (2) PIV (2) HRV (11) RSV (1) MPV (1) PIV (1) RSV (1) Negative for virus, n 11 12 16 -
AdV=adenoviruses; ARI=acute respiratory infection; CoV=coronaviruses; flu A=influenza A/H1N1/California 2009; HPF = high-power field; HRV=human rhinoviruses; IL-8=interleukin 8; MPV=metapneumovirus; PIV=parainfluenza viruses; RSV = respiratory syncytial virus. WURSS-24 = 24-item Wisconsin Upper Respiratory Symptom Survey.
-
Notes: P values come from unadjusted intervention-to-control contrasts, using 2 sample t test for continuous means (SAS software) and proportional difference for binomials (StatXact-5, Cytel Statistical Software & Services). P values represent unadjusted contrasts of interventions to control. Significance was set at P ≤.025.
-
↵a Global severity calculated as the area under the curve using WURSS-24 scores for y-axis and duration of ARI illness as x-axis.
-
↵b IL-8: interleukin-8 (pg/mL) assessed by ELISA (Human IL-8 BD OptEIA Set, BD Biosciences Pharmingen).
-
↵c Two nasal wash samples from the meditation group yielded both CoV and HRV. One ARI in the control group yielded both AdV and HRV.
-
Exercise, Mean (95% CI) Meditation, Mean (95% CI) Control, Mean (95% CI) Outcome 9 wk 3 mo 9 wk 3 mo 9 wk 3 mo Exercise MET min/wk (IPAQ) 2,222 (1,815 to 2,628)a 1,805 (1,356 to 2,253)a 1,037 (694 to 1,381) 1,122 (804 to 1,440) 1,224 (810 to 1,638) 1,050 (688 to 1,412) Mindfulness score (MAAS) 4.59 (4.36 to 4.82) 4.82 (4.59 to 5.05) 4.55 (4.37 to 4.73) 4.73 (4.54 to 4.91) 4.60 (4.40 to 4.81) 4.59 (4.37 to 4.82) Indicators of good health (positive change indicates improvement) Physical health score (SF-12) 51.8 (49.3 to 54.2) 52.0 (49.4 to 54.6) 49.8 (47.2 to 52.3) 50.5 (48.0 to 53.1) 51.1 (48.5 to 53.6) 50.6 (47.8 to 53.6) Mental health score (SF-12) 53.0 (50.9 to 55.1)b 49.7 (46.7 to 52.7) 52.6 (50.5 to 54.7)b 50.5 (48.1 to 53.0)b 49.0 (46.4 to 51.5) 46.3 (43.5 to 49.0) Positive emotion score (PANAS) 36.8 (34.6 to 39.0) 36.2 (33.9 to 38.5) 36.6 (34.8 to 38.4) 36.3 (34.3 to 38.3) 35.3 (33.0 to 37.5) 34.9 (32.7 to 37.0) Optimism (LOT) score 29.0 (27.9 to 30.1) 28.5 (27.3 to 29.6) 27.9 (26.7 to 29.0) 28.0 (26.6 to 29.3) 28.6 (27.4 to 29.7) 29.0 (27.9 to 30.1) Social support score (Ryff PR) 43.4 (41.1 to 45.7) 43.6 (41.3 to 45.9) 42.4 (39.8 to 44.9) 44.5 (42.4 to 46.5) 44.0 (42.1 to 45.9) 44.0 (42.1 to 46.0) Sleep quality score (PSQI) 4.61 (3.49 to 5.73) 4.54 (3.47 to 5.61) 5.02 (4.06 to 5.98) 5.02 (4.20 to 5.84) 5.22 (4.33 to 6.12) 5.10 (4.22 to 5.99) Indicators of poor health (negative change indicates improvement) Perceived stress score (PSS-10) 9.5 (7.8 to 11.2) 10.0 (8.2 to 11.7) 11.2 (9.7 to 12.8) 11.4 (9.5 to 13.4) 10.5 (8.6 to 12.3) 11.4 (9.5 to 13.2) Negative emotion score (PANAS) 14.0 (12.8 to 15.2) 14.4 (13.1 to 15.7) 15.0 (13.7 to 16.2) 15.0 (13.3 to 16.7) 14.6 (13.3 to 15.9) 14.9 (13.8 to 16.0) Anxiety (STAI) score 30.2 (27.6 to 32.8) 29.1 (26.6 to 31.7) 30.7 (28.0 to 33.4) 29.7 (26.9 to 32.5) 31.2 (28.4 to 33.9) 30.4 (27.9 to 32.9) -
IPAQ = International Physical Activity Questionnaire; LOT = Life Orientation Test; MAAS = Mindful Attention Awareness Scale; MET = metabolic equivalent task; Ryff PR = Ryff’s Positive Relationships with Other scale; PANAS = Positive and Negative Affect Schedule; PSQI = Pittsburgh Sleep Quality Index; PSS-10 = 10-item Perceived Stress Scale; SF-12 = 12-item Medical Outcomes Study Short Form; STAI = State Trait Anxiety Inventory.
-
Notes: Data shown represent mean at 9 weeks (1 week after 8-week intervention), then approximately 3 months later. Two-sided P values calculated by simple 2-sample contrast using t test, SAS software. Statistical significance for secondary outcomes should be interpreted as exploratory and hypothesis-generating rather than confirmatory and hypothesis-testing.
-
↵a P <.01 for comparison of intervention means vs control means at each period.
-
↵b P <.05 for comparison of intervention means vs control means at each period.
-
Supplemental Tables
Supplemental Table 1. Zero-Inflated Poisson Regression Model for Total Days of Acute Respiratory Infection; Supplemental Table 2. Zero-Inflated Poisson Regression Model for Area-Under-Curve Severity; Supplemental Table 3. Estimations of Covariate Multicollinearity
Files in this Data Supplement:
- Supplemental data: Tables 1-3 - PDF file, 2 pages, 168 KB
The Article in Brief
Meditation or Exercise for Preventing Acute Respiratory Infection: A Randomized Controlled Trial
Bruce Barrett , and colleagues
Background Treatments for acute respiratory infection (ARI), such as influenza, are not highly effective. Some evidence suggests that strengthening general physical and mental health may reduce the burden of ARI. There is also evidence that mindfulness meditation can reduce stress and negative emotion. This study tests whether training in meditation or exercise can reduce susceptibility to ARI illness.
What This Study Found Training in mindfulness meditation and sustained moderate-intensity exercise are associated with reduced illness severity and fewer days of missed work from acute respiratory infections. In this study, 149 patients were randomized to 1 of 3 study groups: 8-week training in mindfulness meditation, 8-week training in moderate intensity sustained exercise, or observational control. There were substantial reductions in ARI illness among those randomized to exercise training and even greater benefits among those receiving mindfulness meditation training. Implications for the workplace, the authors note, may be especially important. Compared with the control group, all-cause absenteeism was 31 percent lower in both intervention groups. Looking at ARI-related absenteeism in particular, there were 48 percent fewer days missed in the exercise group, and 76 percent fewer in the meditation group.
Implications
- The authors suggest that these findings, if confirmed in future studies, will have important implications for public and private health policy and practice, and for scientific research into maintaining health and preventing disease.
Annals Journal Club
Jul/Aug 2012: Meditation and Exercise for the Common Cold? Who Knew?
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/A JC/.
CURRENT SELECTION
Article for Discussion
- Barrett B, Hayney MS, Muller D, et al. Meditation or exercise for preventing acute respiratory infection: a randomized controlled trial. Ann Fam Med. 2012;10(4):337-346.
Discussion Tips
Meditation and exercise have many benefits. This study tests their benefit for preventing the incidence, duration, symptoms, and dysfunction from acute respiratory tract infections.
Discussion Questions
- What questions are asked by this study?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the question?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How the findings were interpreted?
- What are the main study findings?
- How do the diversity and number of outcome and process measures affect your interpretation of the findings?
- How comparable is the study sample to similar patients in your practice?
- What would be required to make the intervention feasible in practice?
- What is your judgment about the transportability of the findings?
- Would you consider this study to be an efficacy or an effectiveness trial?
- What contextual factors are important for interpreting the findings?
- What is the biological and social plausibility of the findings? What mechanisms might be operating between the intervention and the observed outcomes?
- How might this study change your practice? Policy? Education? Research?
- Who are the constituencies for the findings, and how might they be engaged in interpreting or using the findings?
- What are the next steps in interpreting or applying the findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/con tent/4/3/196.full





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Using nasal sprays to prevent respiratory tract infections: a qualitative study of online consumer reviews and primary care patient interviews
- Patient perceptions of vulnerability to recurrent respiratory tract infections and prevention strategies: a qualitative study
- Effect of Lactobacillus paracasei subsp. paracasei, L. casei 431 on immune response to influenza vaccination and upper respiratory tract infections in healthy adult volunteers: a randomized, double-blind, placebo-controlled, parallel-group study
- Evaluating Exercise as a Therapeutic Intervention for Methamphetamine Addiction-Like Behavior
- Alternative medicine on trial: Clinical trials home in on complementary therapies and complex natural products
- In This Issue: An Abundance of Interventions and Observations to Improve Care