


Abstract
PURPOSE Peer health coaches offer a potential model for extending the capacity of primary care practices to provide self-management support for patients with diabetes. We conducted a randomized controlled trial to test whether clinic-based peer health coaching, compared with usual care, improves glycemic control for low-income patients who have poorly controlled diabetes.
METHOD We undertook a randomized controlled trial enrolling patients from 6 public health clinics in San Francisco. Twenty-three patients with a glycated hemoglobin (HbA1C) level of less than 8.5%, who completed a 36-hour health coach training class, acted as peer coaches. Patients from the same clinics with HbA1C levels of 8.0% or more were recruited and randomized to receive health coaching (n = 148) or usual care (n = 151). The primary outcome was the difference in change in HbA1C levels at 6 months. Secondary outcomes were proportion of patients with a decrease in HbA1C level of 1.0% or more and proportion of patients with an HbA1C level of less than 7.5% at 6 months. Data were analyzed using a linear mixed model with and without adjustment for differences in baseline variables.
RESULTS At 6 months, HbA1C levels had decreased by 1.07% in the coached group and 0.3% in the usual care group, a difference of 0.77% in favor of coaching (P = .01, adjusted). HbA1C levels decreased 1.0% or more in 49.6% of coached patients vs 31.5% of usual care patients (P = .001, adjusted), and levels at 6 months were less than 7.5% for 22.0% of coached vs 14.9% of usual care patients (P = .04, adjusted).
CONCLUSIONS Peer health coaching significantly improved diabetes control in this group of low-income primary care patients.
INTRODUCTION
Primary care faces serious challenges in the face of the growing demand for diabetes care. Primary care physicians are in short supply and need more time to care for patients with highly complex conditions whose costs are destabilizing US health care.1 Current numbers of nurse practitioners and physician assistants are not sufficient to provide access to the increasing demand for primary care.1,2 Registered nurses and pharmacists, who are capable of managing a large proportion of patients with diabetes, are too costly for many primary care practices. The time of medical assistants is often consumed by managing patient flow and assisting clinicians to get through the day.3 In sum, many primary care practices have no one available to provide the time-consuming counseling and teaching of self-management skills that have been shown to improve diabetes outcomes.4
To address this need, several models have been developed to provide support for patient self-management from lay workers with minimal training, including community health workers, lay peer educators, and peer coaches. Community health workers are from the community of the patients they assist but do not necessarily have the same disease as the patient. Though some are volunteers, most are employed by a health facility or community agency.5 Of 4 randomized controlled trials using community health workers for patients with diabetes,6–9 only 1 found a significant reduction in glycated hemoglobin (HbA1c) levels.9 In that study, community health workers visited patients at home twice a month and telephoned every 2 weeks.
Peer educators and coaches (collectively known as peer supporters), in contrast, always have the same disease as the people they assist, are usually volunteers (perhaps receiving a small monetary allowance), and generally focus on providing ongoing support for self-management to a small group of clients.10 Because they experience similar challenges of living with the same chronic condition as the patients they assist, peer supporters are uniquely poised to engage and motivate other patients in self-management.11,12
Peer educators typically lead classes or support groups for individuals with diabetes, either recruited directly from the community or through 1 or more primary care clinics. Two studies of community-based peer support found a significant reduction in HbA1c levels for patients enrolled in a peer-led support group compared with patients in the delayed support arm.13,14 A third, using an Internet-based support intervention, did not find a significant difference (possibly because the mean baseline HbA1c level was only 6.4%).15 A fourth study, with participants recruited from 24 churches, found a small but significant relative reduction in HbA1c levels (0.4%) at 8 months but not at 12 months.16
Although community-based peer support can be effective at improving diabetes control for the relatively small proportion of people with diabetes enrolled from the community, it is not clear whether the results would apply to the majority of patients in a clinic population. In contrast to the largely positive results from community-based peer education, studies that have evaluated clinic-based peer educator groups have had mixed results. Of 2 clinic-based peer educator interventions, 1 found no intervention effect,17 whereas the other found a significant drop in HbA1c levels for the intervention.18 Both studies were limited by low enrollment.
Peer coaches, in contrast with peer educators, provide support to individuals, which is more flexible for patients who have difficulty attending scheduled group meetings. The few published randomized controlled trials of using peer coaching for patients with diabetes have reported mixed results; 1 found no coaching benefit,19 and 2 reported a significant benefit from coaching.21,20 The latter 2 studies were both conducted with veterans, almost all of whom were men. In addition, 1 study was restricted to African Americans,21 and the second was limited by an enrollment rate of less than 25%.20
Patients with limited resources seen in public (safety-net) clinics often face cultural, language, and literacy barriers to self-management, making peer support particularly appealing. We conducted a randomized controlled trial of peer coaching vs usual care to test the impact of individual peer coaching on glucose control on patients with poorly controlled diabetes attending public clinics.
METHODS
The study was a randomized controlled trial comparing peer health coaching with usual care. A detailed description of the study methods has previously been published22 and is summarized here.
Setting and Participants
All participants were low-income patients seen at 1 of 6 public health clinics that were part of the San Francisco Bay Area Collaborative Research Network. Patients who could potentially be peer coaches were identified by searching the electronic record to locate patients at each clinic who had an HbA1c level of less than 8.5% within the past 6 months and who spoke English or Spanish. A list of patients meeting these criteria was given to their primary care clinicians, who provided a recommendation regarding the patients’ suitability to coach. Additional patients were sometimes recommended by clinic staff or responded to flyers describing the study.
Patients to be randomized to receive peer coaching or usual care were identified from the electronic medical record as being potentially eligible if they spoke English or Spanish and had an HbA1c level of 8.0% or greater within the past 6 months. All patients meeting these criteria were screened by their primary care clinicians, who could exclude any patient considered to be inappropriate, usually because of physical or mental conditions. The remaining patients were ordered randomly and approached by letter, telephone call, or in person during a clinic visit to be further screened and recruited into the study. All participants provided informed consent. The study was approved by the Committee on Human Research (Institutional Review Board) at the University of California, San Francisco (approval number H40013-34104-01-01). The authors had no conflicts of interest.
Intervention: Peer Coaching
Potential peer coaches attended 36 hours of training over 8 weeks in either English or Spanish using a curriculum developed by the study team that included instruction in using active listening and nonjudgmental communication, helping with diabetes self-management skills, providing social and emotional support, assisting with lifestyle change, facilitating medication understanding and adherence, navigating the clinic, and accessing community resources. The curriculum can be found at http://familymedicine.medschool.ucsf.edu/cepc/pdf/HealthCoachTrainingCurriculumMay08.pdf. Training was conducted by 2 of the investigators (A.G. and T.A.B.) and used small-group didactics, role-playing, and observed practice coaching sessions. Trainees who passed both a written and an oral examination became peer coaches in the study. Peer coaches interacted in person with the patients they coached at the discretion of the coach and patient, either outside the clinic by telephone or during a clinic visit; target goals for coaching sessions were telephone contact at least twice a month and 2 or more in-person contacts over 6 months. Coaches helped patients design action plans to achieve goals chosen by the patient. Trainees were paid $150 for completing the training (regardless of whether they passed), and coaches received $25/month for each client they coached.
Usual Care
Usual care included all services normally available to patients, including access to a nutritionist and diabetes educator through referral from their primary care clinician.
Randomization, Enrollment, and Follow-up
Patients who enrolled and completed baseline data collection were paid $10 and assigned to the usual care or peer-coaching study arm using randomly ordered opaque envelopes. Patients assigned to usual care were told they would be contacted in 6 months to repeat the baseline measurements. Most patients in the coaching arm (more than 80%) selected a peer coach from a brief coach profile, whereas the rest were assigned a peer coach based on coach availability.
Of the 37 patients who enrolled to train as coaches, 26 completed and passed the training and were designated as peer coaches. Of these 26 peer coaches, 2 dropped out for personal reasons before starting coaching.
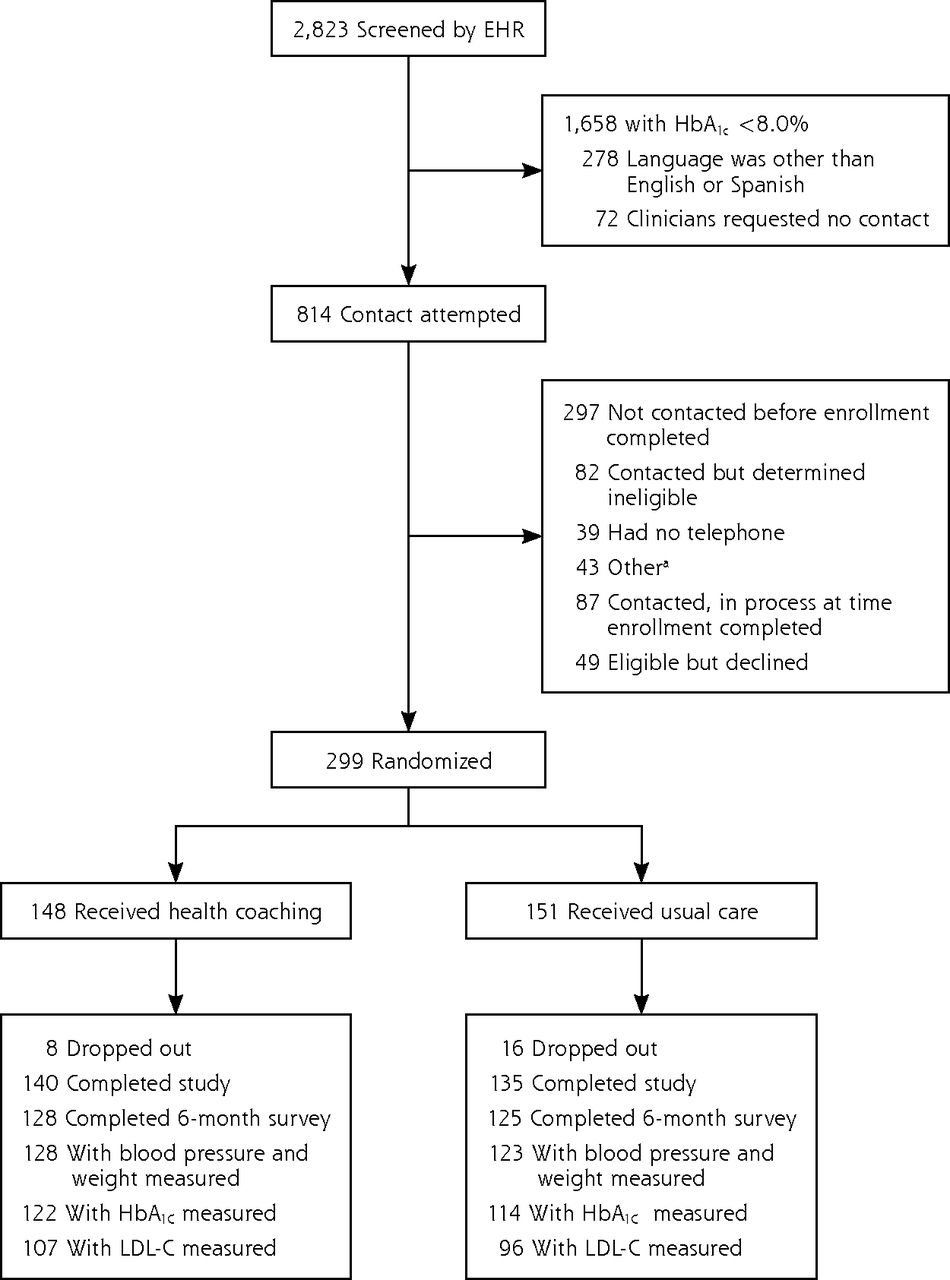
Patients randomized to receive health coaching or usual care were enrolled from March 2010 through October 2010. As displayed in Figure 1, 814 patients met our initial eligibility requirements, of which 297 could not be contacted. Of the 517 patients contacted, 82 were determined to be ineligible, and 87 had been contacted but were still in process at the completion of enrollment, yielding 348 patients, of whom 49 (14%) declined to participate, and 299 were enrolled and randomized.
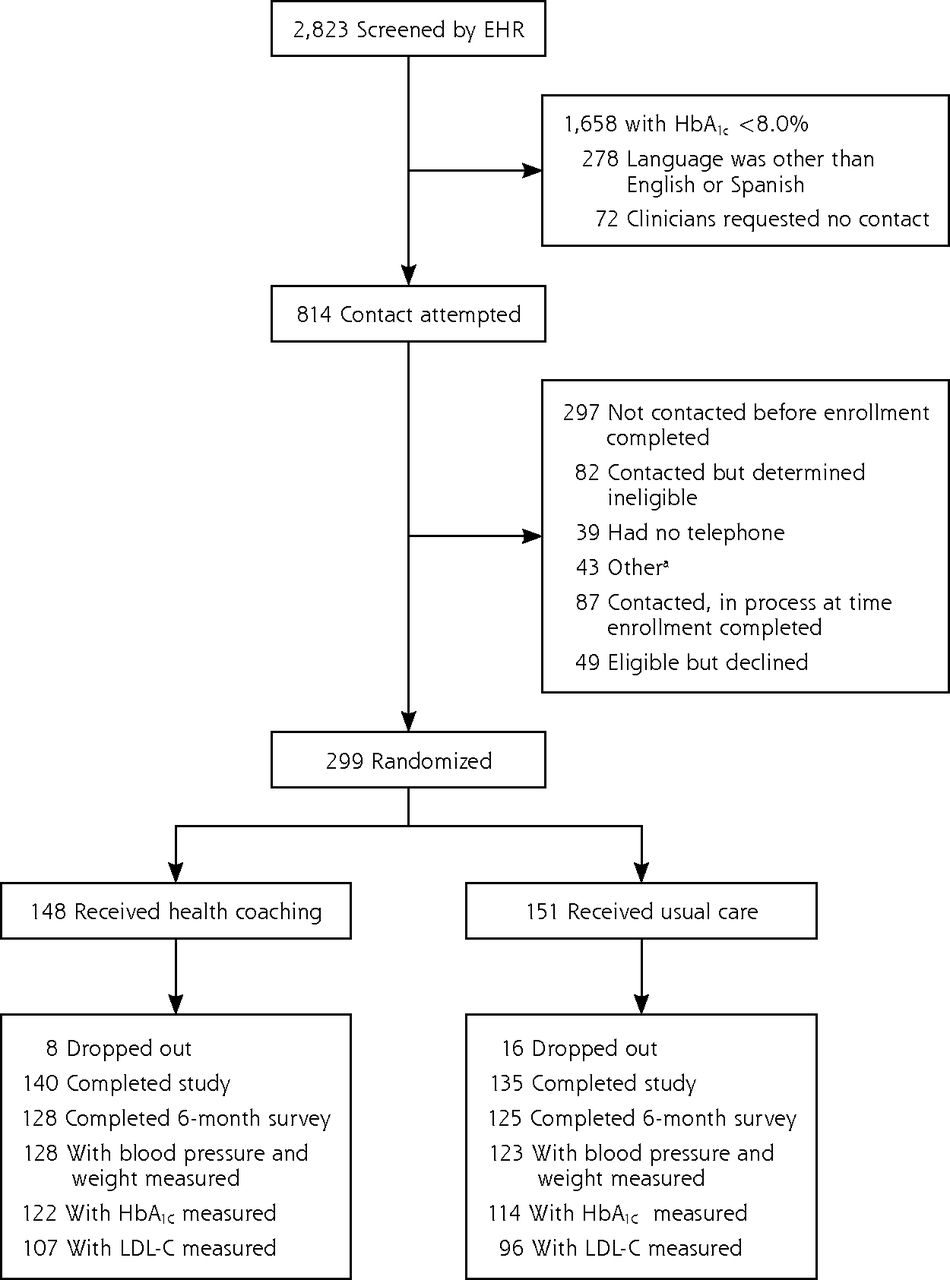
Screening, randomization, and completion.
EHR = electronic health record, HbA1c = glycated hemoglobin; LDL-C = low-density lipoprotein cholesterol.
a Moved out of area (n = 4), not sure will continue to get care at current clinic (n = 15), enrolled in another study (n = 5), other (n = 24).
Measures
At enrollment, a research assistant administered a baseline questionnaire to patients that included questions about demographic characteristics, years with a diagnosis of diabetes, use of insulin, and diagnoses of hypertension or hyperlipidemia. In addition, the research assistant measured participants’ height (using a tape measure and right angle), weight (using a calibrated portable scale), and blood pressure. Blood pressure was measured twice, at least 2 minutes apart, with an Omron Upper Arm Blood Pressure Monitor model HEM-711AC in the left arm after the patient had been sitting for at least 5 minutes. Blood pressure was entered as the average of the 2 readings; if the 2 systolic readings differed by more than 5 points, a third blood pressure reading was taken, and the average of all 3 readings was used.
Participants who did not have a low-density lipoprotein cholesterol (LDL-C) measurement in the past 11 months received a requisition to perform laboratory testing. All LDL-C and HbA1c levels were measured at a central laboratory at San Francisco General Hospital using a Bio-Rad Variant II Turbo (NSGP-certified) system (Bio-Rad Laboratories, Inc). The baseline questionnaire (without the questions on demographics and health literacy) was readministered at 6 months. Weight and blood pressure were measured at 6 months, and patients received a laboratory requisition for LDL-C and HbA1c testing. We used values for HbA1c and LDL-C that were closest in time to the target date (enrollment or 6 months after enrollment) and within the prespecified window (11 months before to 4 weeks after enrollment for LDL-C, 6 months before to 4 weeks after enrollment for HbA1c, and 5 to 9 months after enrollment for the 6-month HbA1c and LDL-C measurements).
Outcomes
The a priori primary outcome was change in HbA1c level from enrollment to the end of the study. Secondary outcomes were the percentage of patients whose HbA1c level dropped by 1.0% or more and the percentage of patients with an HbA1c level of less than 7.5% at the end of the study. Additional outcomes examined were changes in LDL-C levels, systolic blood pressure, and body mass index calculated as kg/m2.
Study Power and Data Analysis
The original study protocol was to enroll 400 patients. The actual number of patients enrolled was 299 because of budgetary constraints. Assuming a difference in an HbA1c of 0.6% between the 2 study arms and a standard deviation of 1.7%,23–25 the 299 patients enrolled provided a power of .80 to detect a significant difference (P <.05, 2-sided) in change in HbA1c levels between study arms.
Analyses were by intention to treat and in accordance with the CONSORT guidelines for reporting results from clinical trials.26 Changes in primary and secondary outcomes were compared between study arms using a linear mixed model for continuous outcomes and logistic regression for categorical outcomes. Missing data were treated as missing (not imputed). Because the intraclass correlation coefficient for change in HbA1c level by clinic was extremely low (<.01), clustering by clinic was negligible, and clinic site was not retained in the models.
RESULTS
Less than 1% of baseline data was missing for all variables except for employment (2%), years with diabetes (2%) and LDL-C values (9%). Baseline HbA1c measurements were available a median of 30 days before enrollment in the usual care arm (interquartile range [IQR] = 57 to 4 days before enrollment) and 34 days before enrollment in the coaching arm (IQR = 74 to 6 days before enrollment) (difference not significant). The 6-month HbA1c was generally measured at or close to the target date of 6 months from enrollment, with the median difference between the actual and target date being 2 days (IQR = 10 days before to 24 days after the 6-month date) for patients in usual care, and 0 days (IQR = 6 days before to 24 days after the 6-month date) for patients in the coaching group (difference not significant).
Baseline characteristics of coaches and of patients by study arm are presented Table 1. The mean age of patients was 55 years (range 29 to 82). Slightly more than one-half of the patients were women, and approximately one-half were immigrants with a primary language other than English (usually Spanish). Patients in the coaching group were less likely to be working outside the home and to have hypertension compared with usual care patients. Coaches were approximately the same age and similar in race and ethnicity as the patients receiving coaching, but were more likely to be female and have English as their primary language. As expected, coaches also had better controlled diabetes. Of the 299 patients enrolled, 24 (8%) did not provide any 6-month data and were therefore considered to have dropped out (Figure 1). Patients who dropped out were on average younger, more likely to smoke, and less likely to report having hyperlipidemia, but did not otherwise differ significantly from patients remaining in the study. Of the 275 patients who completed the study, 253 (92%) completed the 6-month questionnaire with a mean time from enrollment of 6.1 ± 0.6 months; more than 93% completed the questionnaire between 5 and 7 months. Coaches worked with a median of 7 patients (mean = 6.1). Coached patients had a median number of 5 interactions with their peer health coach, with a range from 0 to 29; 123 patients (83%) had at least 1 interaction. Most interactions were by telephone (76.6%) and the remainder were in-person.
Baseline Characteristics of Coaches and Patients by Study Arm
Primary and secondary outcomes are displayed in Table 2. Baseline HbA1c levels were similar in the 2 arms at baseline. Both groups experienced a decrease in HbA1c levels, but the decrease in the HbA1c level was significantly greater for the coached patients (1.07% vs 0.30%, adjusted difference = 0.69%; P = .01) A drop in HbA1c level of 1.0% or more was seen in 49.6% patients in the coaching arm compared with 31.5% in the usual care arm (P = .001, adjusted), and 22.0% of patients in the coaching arm achieved an HbA1c of less than 7.5% compared with 14.9% in the usual care arm (P = .04, adjusted). There was no significant difference in change for LDL-C, systolic blood pressure, or body mass index after adjustment for differences in baseline variables.
Outcomes for Patients With HbA1C Levels Measured at 6 Months
DISCUSSION
This randomized controlled trial of clinic-based peer coaching for low-income, underserved patients with poorly controlled type 2 diabetes found a clinically important and statistically significant greater reduction in HbA1c levels in patients who received peer coaching compared with those in the usual care arm. Our results are consistent with the results from 2 prior studies of peer coaching20,21 in veterans, who were almost entirely male. In the one negative randomized controlled trial of peer coaching, the coaches’ role was limited to reinforcing goals set by the patients’ physician19,27 in contrast to the 2 positive studies and our study, which used patient-defined goals.
The results of the current study add to the growing body of support for the effectiveness of peer coaching in improving glycemic control for patients with type 2 diabetes. Peer coaching was accepted by a large proportion of patients in this safety-net population, as well as by clinicians and clinic staff. Whether peer coaching would be as acceptable outside a veterans’ or a public clinic population remains to be shown, but there does not appear to be any reason it would not. The generalizability of peer coaching to other chronic diseases is not known. Most studies of peer support have focused on patients with diabetes. Given that issues typically addressed in action plans for patients with diabetes are relevant to most chronic conditions, it seems likely that peer coaching could be effective for patients with such chronic conditions as hypertension, asthma or congestive heart failure. Many important aspects of peer coaching remain to be studied, including patients’ experience with and preferences for peer coaching and how peer coaches can be more integrated into the health care team.
Perhaps the single most important question is how peer coaching can be supported outside research studies. Although peers coaches are generally volunteers, they need training and some level of supervision. Most peers receive reimbursement for costs and some financial incentive. Reducing these costs would likely increase coach turnover and impair the effectiveness of the program. Moreover, successful coaching to improve patient self-management may not decrease costs in the short run, as patients are encouraged to take their medication as prescribed, get appropriate tests and preventive services, and have regular follow-up with their clinician.
Some potential benefits, such as reducing time needed by clinic staff to support patient self-management, are difficult to quantify. Other benefits, such as fewer emergency department visits, a lower no-show rate for appointments, or fewer complications from poorly controlled diabetes, may not outweigh the costs of increased medications.28 Long-term benefits from improved glycemic control can be calculated29,30 but are most relevant to payers and providers who pay for costs for the same patients over a long period. Nonetheless, peer coaching appears to improve glycemic control and can take the pressure off the primary care clinicians and staff to provide support for patient self-management.
The findings from the current study should be considered in the context of study’s limitations. We chose to conduct the study with a diverse group of underserved patients who had poorly controlled diabetes because they represent a population at higher risk for diabetic complications and may have difficulty accessing medical care. We do not know to what extent our results will generalize to other populations, such as middle-class white patients or patients with better diabetes control. Baseline HbA1c was measured, on average 1 month and up to 6 months before enrollment for some patients. Timing did not differ between study arms, however, and would be unlikely to bias the results. Because patients receiving peer coaching and those receiving usual care were seen at the same clinics, and often by the same clinicians, it is possible that the presence of peer coaching influenced (contaminated) the usual care group. Such an effect would be expected to make the groups more alike and make it more difficult to show a difference between groups. Our follow-up ended at 6 months; thus, we do not know whether the impact of coaching on diabetes control will diminish with time.
Patients are generally not considered as potential resources available to increase primary care capacity. The peer-coaching model creates a structure whereby volunteer peer coaches contribute to the work of primary care teams by providing one-on-one self-management support to patients. Our study shows that clinic-based peer coaches can take on this role in low-income communities and that peer coaching, when compared with usual care conducted in the same clinics, is associated with a significant improvement in patients’ glycemic control.
Acknowledgments:
We would like to acknowledge the members of our study staff whose hard work made this study possible: Marissa Pimental, Denise De Vore, Maria Vivas, Victoria Ngo, and Russell Yamamoto. The study clinical sites are part of the San Francisco Bay Area Collaborative Research Network.
Footnotes
-
Conflicts of interest: authors report none.
-
To read or post commentaries in response to this article, see it online at http://www.annfammed.org/content/11/2/137.
-
Funding support: The study was funded by a grant from the American Academy of Family Physicians.
-
Disclaimer: The American Academy of Family Physicians approved the study design but had no role in the conduct of the study, data analysis, or reporting of the results.
-
Clinical Trials Identifier: NCT01040806. http://clinicaltrials.gov/ct2/show/NCT01040806?term=NCT01040806&rank=1
- Received for publication April 1, 2012.
- Revision received June 23, 2012.
- Accepted for publication July 11, 2012.
- © 2013 Annals of Family Medicine, Inc.
References





{kind=link}
Jump to section
Related Articles
Cited By...
- Virtual Group Pulmonary Rehabilitation in COPD Facilitated by a Peer Coach
- The Natural Helper approach to culturally responsive disease management: protocol for a type 1 effectiveness-implementation cluster randomised controlled trial of a cultural mentor programme
- Peer Coaching to Improve Diabetes Self-Management Among Low-Income Black Veteran Men: A Mixed Methods Assessment of Enrollment and Engagement
- Peer mentorship to improve self-management of hip and knee osteoarthritis: a randomised feasibility trial
- Examining Variations in Action Plan Quality Among Adults With Type 2 Diabetes in Primary Care
- Lifestyle interventions for type 2 diabetes management among migrants and ethnic minorities living in industrialized countries: a systematic review and meta-analyses
- Diabetes Self-management Education and Support in Adults With Type 2 Diabetes: A Consensus Report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association
- Making Inroads in Addressing Population Health in Underserved Communities With Type 2 Diabetes
- Outcomes at 18 Months From a Community Health Worker and Peer Leader Diabetes Self-Management Program for Latino Adults
- Roles and Functions of Community Health Workers in Primary Care
- Clinical Population Medicine: Integrating Clinical Medicine and Population Health in Practice
- Improving risk factor management for patients with poorly controlled type 2 diabetes: a systematic review of healthcare interventions in primary care and community settings
- Peer Support Interventions for Adults With Diabetes: A Meta-Analysis of Hemoglobin A1c Outcomes
- A Qualitative Study of How Health Coaches Support Patients in Making Health-Related Decisions and Behavioral Changes
- What Happens After Health Coaching? Observational Study 1 Year Following a Randomized Controlled Trial
- Diabetes Self-management Education and Support in Type 2 Diabetes: A Joint Position Statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics
- Key Features Of Peer Support In Chronic Disease Prevention And Management
- Contributions of Peer Support to Health, Health Care, and Prevention: Papers from Peers for Progress
- Peer Coaches to Improve Diabetes Outcomes in Rural Alabama: A Cluster Randomized Trial
- Peer Support for Diabetes Management in Primary Care and Community Settings in Anhui Province, China
- Puentes hacia una mejor vida (Bridges to a Better Life): Outcome of a Diabetes Control Peer Support Intervention
- Are Low-Income Peer Health Coaches Able to Master and Utilize Evidence-Based Health Coaching?
- Challenges in the Ethical Review of Peer Support Interventions
- Diabetes Self-management Education and Support in Type 2 Diabetes: A Joint Position Statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics
- Health Coaching by Medical Assistants to Improve Control of Diabetes, Hypertension, and Hyperlipidemia in Low-Income Patients: A Randomized Controlled Trial
- Improving awareness, accountability, and access through health coaching: Qualitative study of patients' perspectives
- Effect of social networks intervention in type 2 diabetes: a partial randomised study
- The 10 Building Blocks of High-Performing Primary Care
- Primary Care: Proposed Solutions To The Physician Shortage Without Training More Physicians
- Effectiveness of general practice based, practice nurse led telephone coaching on glycaemic control of type 2 diabetes: the Patient Engagement And Coaching for Health (PEACH) pragmatic cluster randomised controlled trial
- In This Issue: Finding the Sweet Spot in Health Care