


Abstract
PURPOSE Burnout, attrition, and low work satisfaction of primary care physicians are growing concerns and can have a negative influence on health care. Interventions for clinicians that improve work-life balance are few and poorly understood. We undertook this study as a first step in investigating whether an abbreviated mindfulness intervention could increase job satisfaction, quality of life, and compassion among primary care clinicians.
METHODS A total of 30 primary care clinicians participated in an abbreviated mindfulness course. We used a single-sample, pre-post design. At 4 points in time (baseline, and 1 day, 8 weeks, and 9 months postintervention), participants completed a set of online measures assessing burnout, anxiety, stress, resilience, and compassion. We used a linear mixed-effects model analysis to assess changes in outcome measures.
RESULTS Participants had improvements compared with baseline at all 3 follow-up time points. At 9 months postintervention, they had significantly better scores (1) on all Maslach Burnout Inventory burnout subscales—Emotional Exhaustion (P =.009), Depersonalization (P = .005), and Personal Accomplishment (P <.001); (2) on the Depression (P =.001), Anxiety (P =.006), and Stress (P = .002) subscales of the Depression Anxiety Stress Scales-21; and (3) for perceived stress (P = .002) assessed with the Perceived Stress Scale. There were no significant changes on the 14-item Resilience Scale and the Santa Clara Brief Compassion Scale.
CONCLUSIONS In this uncontrolled pilot study, participating in an abbreviated mindfulness training course adapted for primary care clinicians was associated with reductions in indicators of job burnout, depression, anxiety, and stress. Modified mindfulness training may be a time-efficient tool to help support clinician health and well-being, which may have implications for patient care.
INTRODUCTION
Physician burnout is a pervasive health care problem characterized by a loss of emotional, mental, and physical energy due to continued job-related stress. Burnout is more common among physicians than among other professionals, with specialties on the front lines such as primary care being at greatest risk.1 Up to 60% of physicians report having experienced burnout at some point in their careers,2 with as many as 30% to 40% experiencing burnout at any given time.3 Considerable evidence suggests that burnout negatively affects patient care,4 which poses new challenges with implementation of the Patient Protection and Affordable Care Act. Providing insurance to 32 million previously uninsured citizens will increase demand for primary care services.5 An expanding older adult population, insufficient supply of primary care physicians, low medical student interest in primary care, lower primary care reimbursement, and increasing workload will add further strain to these professionals.6–9 This situation is compounded by physicians’ tendency to give suboptimal attention to self-wellness3 and the possibility that they may become alienated or depersonalized in an increasingly bureaucratized health care system.9,10
Mindfulness is a form of mental training that enables one to attend to aspects of experience in a nonjudgmental, nonreactive way, which in turn helps cultivate clear thinking, equanimity, compassion, and open-heartedness.11 The goal is to maintain open awareness in one’s experience in a way that generates a greater sense of emotional balance and well-being. Through mindfulness practice, unhelpful habitual thoughts and behaviors can be recognized, allowing for new and creative ways of responding.
A previous study demonstrated that mindfulness education over 12 months is helpful in addressing burnout by improving mood and emotional stability among primary care physicians.12 Other studies demonstrate that an 8-week mindfulness class can also improve mood and emotional exhaustion (a component of burnout) for hospital administrative and direct patient care staff13 and decrease perceived stress in health care professionals.14 The authors of the latter study, which had a high dropout rate in the intervention group, suggested participants’ lack of time was a major concern.14 It is unknown whether an adapted mindfulness training period that lessens the time burden for clinicians would produce similar positive results. Addressing this barrier is particularly important given the high work demands and time constraints of primary care medicine.8
We undertook this study as a first step in investigating whether an abbreviated mindfulness intervention could increase job satisfaction, quality of life, and compassion in primary care clinicians. We were well positioned to address this question given our association with staff from the University of Wisconsin (UW) Health Mindfulness Program, which has a 20-year history of facilitating mindfulness-based stress reduction (MBSR) classes, and our location within a medical school with large primary care residency programs, which aided our recruitment efforts.
METHODS
Study Participants
We recruited 30 primary care clinicians from the UW-Madison departments of family medicine, internal medicine, and pediatrics. Recruitment methods included e-mail invitations, flyers, visits to departmental meetings and clinics, and word of mouth. Inclusion criteria were (1) employment as a primary care medical doctor or doctor of osteopathy, nurse practitioner, or physician assistant; (2) working at least 50% time in direct patient care; (3) availability to attend all or most intervention sessions; (4) willingness to do 10 to 20 minutes of mindfulness-related activity daily, and (5) agreement to complete a 15- to 30-minute online survey 4 times. The study coordinator conducted telephone screening interviews with clinicians expressing interest in the project. Those eligible were enrolled on the return of a signed consent form.
The UW-Madison Health Sciences Institutional Review Board approved this study.
Intervention
All study participants received the intervention—an abbreviated version of the 8-week MBSR program developed by Jon Kabat-Zinn at the University of Massachusetts Medical Center that is taught regularly by the UW Health Mindfulness Program. MBSR is a well-researched and clinically useful program widely recognized as a healthy way to manage symptoms of stress.11 Of the various meditation styles, mindfulness is particularly suitable for physician burnout because it is nonreligious yet addresses meaning and purpose, has secular and academic appeal, and has a solid scientific foundation. We focused on creating a mindfulness course that was efficient but sufficient in teaching the basic practices of mindfulness meditation. We encouraged participants to view clinical work as an opportunity to practice mindfulness.15
Table 1 presents a comparison between the study’s modified MBSR training and the longer, typical MBSR course. The study’s intervention was conducted in 2 groups of 15 participants each, led by UW mindfulness instructors who have completed professional training through the University of Massachusetts Center for Mindfulness and other advanced teacher training. UW Integrative Medicine faculty facilitated the final follow-up sessions. The first evening session was held 10 days after the end of the mindfulness training, and the second session was held 2 to 3 weeks after the first evening session. Activities included guided sitting and walking mindfulness practices. Participants were encouraged to report their experiences in a shared group setting, including examples of “practice in your practice,”15 an adaptive mindfulness approach, that reflected working with patients using mindful attitudes.
Comparison of Modified MBSR Training With Typical MBSR Course
We created a Web site for this study15 that assisted clinicians in bringing their mindfulness practice into the examination room, where the patient becomes the centering focus. The goal was to help the clinician be more present with patients using the practice in your practice approach. The Web site provides instruction to pause, be fully present with the patient, and then proceed with recommendations, questions, and advice that mindfully address the patient’s needs.
Survey Procedures
We conducted 4 surveys using Qualtrics, a secure Web-based survey system, via links within e-mail messages. Completed survey questionnaires were saved to the Qualtrics Web site anonymously. Asking 3 innocuous questions on each resulted in responses unique to each participant. This approach allowed us to identify the 4 questionnaires answered by the same respondent without revealing identity. We sent the link for survey 1 (baseline) after each participant signed the consent form, but no more than 2 weeks before the training started. We e-mailed links for survey 2 the day after the last mindfulness training session, for survey 3 at 8 weeks after the last session, and for survey 4 at 9 months postintervention. We sent up to 2 reminder e-mails for each survey.
Outcome Measures
Each survey questionnaire had 5 validated measures: the Maslach Burnout Inventory (MBI); the Depression Anxiety Stress Scales-21 (DASS-21); the Perceived Stress Scale (PSS); the 14-item Resilience Scale (RS-14); and the Santa Clara Brief Compassion Scale (SCBC).
Job Satisfaction
The MBI, used to investigate job satisfaction, consists of 22 questions that assess 3 aspects of professional burnout syndrome: emotional exhaustion, depersonalization, and lack of personal accomplishment.16 The MBI is used worldwide and has been validated in samples of health care workers, including primary care clinicians.17,18 Respondents record how often they experience job-related feelings using a 7-point Likert scale ranging from “never” to “every day.” Burnout is conceptualized as a continuous variable along a spectrum ranging from low to high experienced feelings, and not as a dichotomous condition that is either present or absent.16 Three scores are computed for each respondent, 1 for each aspect of burnout, and are not combined into a composite score. A high degree of burnout is one in which a respondent has high scores on the Emotional Exhaustion and Depersonalization subscales, and a low score on the Personal Accomplishment subscale.16
Quality of Life
We assessed quality of life measures using the DASS-21, PSS, and RS-14, which are brief but validated research tools used worldwide. The DASS is a set of 3 scales designed to measure emotional states of depression, anxiety, and stress.19 It measures current state or change in state over time. The major development of the DASS was done with nonclinical samples, and it is well suited for use with nonclinical populations in research. We used a version consisting of 21 questions, 7 in each of the 3 scales. Respondents record how much a statement applies to them over the past week using a 4-point Likert scale ranging from “not at all” to “very much or most of the time.” Higher scores indicate greater levels of that emotional state.
The PSS, designed for use in community samples, is a validated scale used widely to measure the perception of stress. It assesses how unpredictable, uncontrollable, and overloaded respondents experience their lives.20 We used the shorter, validated 10-item version.20 Respondents record how often they felt a certain way during the past month using a 5-point Likert scale ranging from “never” to “very often.” As the PSS is not a diagnostic tool, there are no cutoff ranges for high and low levels. Comparisons can be made within a population sample, over time, and with national normative data. Higher scores indicate greater perceived stress.
The RS directly measures resilience, the ability to recover from adversity.21 It has been used in research with a variety of populations in a wide range of ages and socioeconomic groups. We used a validated 14-item version whereby respondents recorded to what extent they agreed or disagreed with statements using a 7-point Likert scale ranging from “strongly disagree” to “strongly agree.” Total scores for this scale are computed, with higher scores indicating higher resilience.
Compassion
We assessed compassion using the SCBC—a brief, validated version of Sprecher and Fehr’s Compassionate Love Scale,22 a respected and reliable scale developed for use with the general public. Compassionate love is defined as an attitude toward others that is “focused on caring, concern, tenderness; and an orientation toward supporting, helping, and understanding others.”23(p630) The SCBC has 5 questions. Respondents record to what extent ranging from “not at all true of me” to “very true of me.” Higher scores indicate greater compassion.
Statistical Analysis
We conducted descriptive analysis before formal testing in this uncontrolled exploratory study to determine if a short course of mindfulness training would improve specific outcomes. The demographic and individual variables and study outcomes were described by way of frequencies (percents) and mean values. Mean and median tests were also performed. The study outcome data were analyzed with linear mixed effects models,24 which estimate change in values while accounting for the nested structure of the repeated individual measures. Mixed effects models integrated all 4 surveys’ data for all study participants while adjusting estimates for missing data points. The time dependencies were modeled with an AR(1) autoregressive error structure. Values for outcomes on the baseline survey were compared with those on the subsequent 3 surveys. This approach allowed us to estimate changes in the outcome measures during the postintervention period and ascertain whether the changes persisted in the 9-month follow-up period. All analyses were conducted with SAS version 9.1 for Linux (SAS Institute Inc).25
RESULTS
Participants
Of the 30 clinicians enrolled, all completed the baseline measures. One withdrew from the study. During follow-up, 28 (93%) of the participants gave responses for survey 2, and 23 (77%) gave responses for surveys 3 and 4. Participants who failed to complete the follow-up surveys did not differ in their baseline responses from those who complied with the study protocol. Table 2 describes demographic and other characteristics for the study sample.
Participants’ Characteristics at Baseline (N = 30)
Outcomes
Job Satisfaction
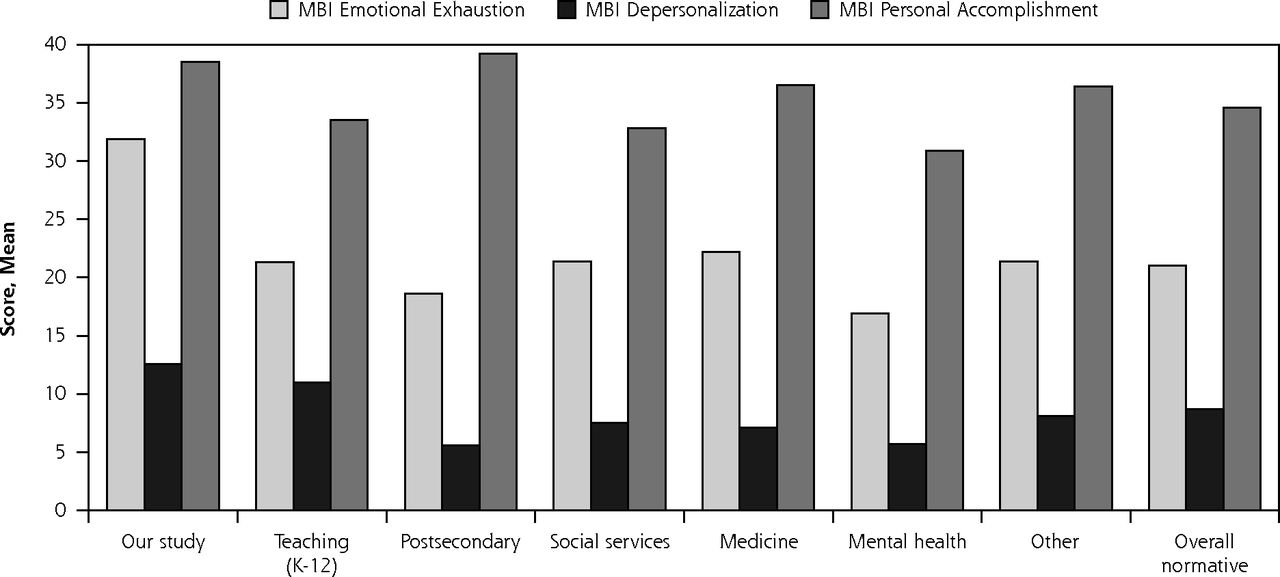
Figure 1 compares the mean MBI scores of our study participants at baseline (N = 30) with the means from the MBI normative sample (N = 11,067) on the 3 subscales. Our study participants scored high on 2 aspects of the burnout syndrome: emotional exhaustion (mean = 31.9, SD 9.6) and depersonalization (mean = 12.6, SD 6.7), indicating a high level of burnout; however, they also scored high on personal accomplishment (mean = 38.5, SD 5.2), indicating a high sense of personal accomplishment. A comparison of MBI means reveals that our participants appeared to score 1.1 SDs higher than the overall MBI normative sample on emotional exhaustion. Depersonalization scores were similar only to those of the teaching (K-12) subgroup and were significantly higher (by 0.6 SDs) than those of the overall normative sample. Our respondents scored 0.8 SDs higher on the Personal Accomplishment subscale than the overall normative sample, however, with scores comparable to those of the postsecondary education subgroup and others.

Baseline Maslach Burnout Inventory (MBI) subscale mean scores for study sample (N = 30) compared with the MBI normative sample (N = 11,067).
Notes: The MBI normative sample consists of the following occupational subgroups: teaching (K-12) subgroup is composed of 4,163 teachers of kindergarten through grade 12; postsecondary education subgroup is composed of 635 college and professional school educators; social services subgroup is composed of 1,538 social workers and child protective services workers; medicine subgroup is composed of 1,104 physicians and nurses; mental health subgroup is composed of 730 psychologists, psychotherapists, counselors, mental hospital staff, and psychiatrists; “other” subgroup is composed of 2,897 legal aid employees, attorneys, police officers, probation officers, ministers, librarians, and agency administrators.14
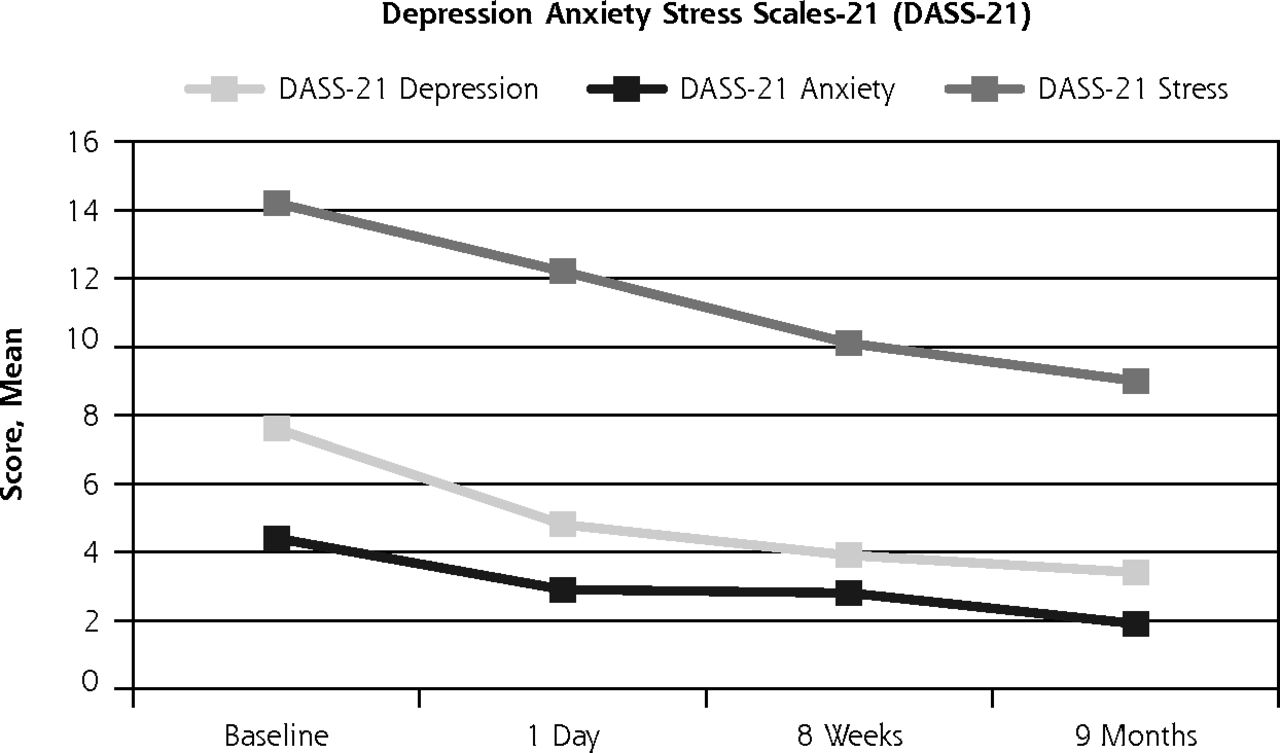
Table 3 and Figure 2 show scores for all of our outcome measures at baseline and specific times postintervention. On the MBI, respondents had significant decreases from baseline in emotional exhaustion scores on surveys 2, 3, and 4 (P = .046, P = .006, and P = .009, respectively). Depersonalization scores were also significantly reduced on surveys 3 and 4 (P = .03 and P = .005, respectively). There was an increase in personal accomplishment scores on all follow-up surveys (all P <.001).
Outcomes Scores at Each Survey With Comparison to Baseline (N = 30)


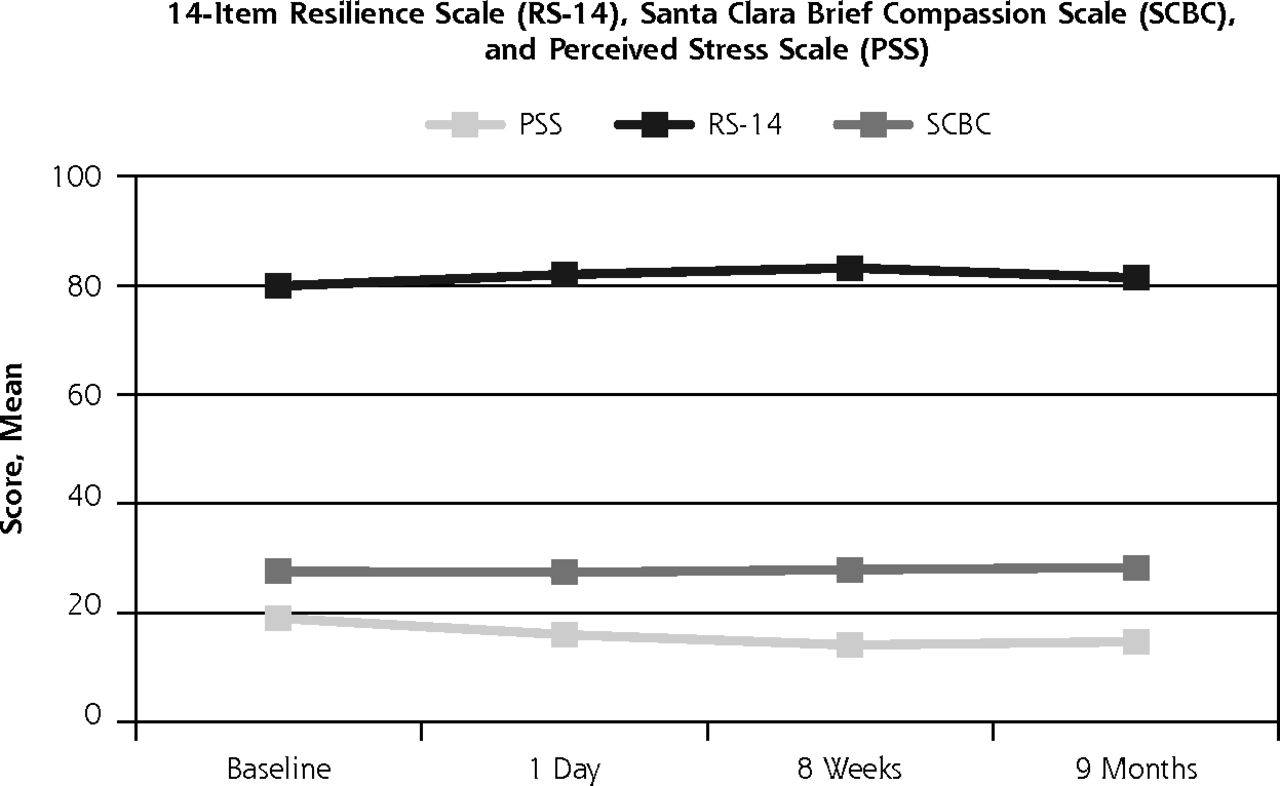
Means for the outcome measures assessed at baseline and postintervention (N = 30 at baseline).
Quality of Life and Compassion
On the DASS-21, study participants displayed significant improvements in depression scores at all follow-up surveys (P ≤.001), anxiety scores on surveys 2 and 4 (P = .022 and P = .006, respectively), and stress scores on surveys 3 and 4 (P = .007 and P = .002, respectively). On the PSS, study participants also had a significant reduction in perceived stress from baseline after the intervention on all 3 follow-up surveys (P = .001, P <.001 and P = .002, respectively). There was no significant change resilience or compassion, as assessed with the RS-14 and SCBC scores, over time.
DISCUSSION
Our findings suggest that an abbreviated mindfulness intervention may help ease professional burnout and support well-being for primary care clinicians.
After a modified mindfulness intervention (Table 1) that consisted of a nonresidential weekend immersion along with 2 short follow-up evening sessions, we found significant reductions in measures of burnout, depression, anxiety, and stress on all 3 follow-up surveys that are consistent with previous research findings.12 It is noteworthy that these long-term benefits were obtained after a relatively short exposure to mindfulness training. That this effect was maintained over 9 months without formal intervention booster sessions suggests that even limited initial training may be sufficient in teaching fundamental mindfulness practices. We believe that these findings are the first to demonstrate significant long-term effects from an abbreviated mindfulness intervention. A randomized controlled trial is needed to confirm these promising results.
Particularly striking was the high level of emotional exhaustion and depersonalization at baseline among participants in this study. This finding is concerning given that burnout, mood disorder, and suicide are considerable occupational hazards for physicians26,27 that affect many aspects of patient care including associations with lower patient satisfaction, decreased treatment adherence,3,6 and disrupted continuity of care due to physician attrition and early retirement.28 Additionally, burnout negatively affects quality of health care delivery in that physicians self-report increased medical errors, lower empathy, and decreased job dissatisfaction.3,6 Conversely, increased emotional awareness is associated with less burnout, higher work satisfaction, and higher patient satisfaction.29
Although the DASS-21 measures improved significantly after the mindfulness training, these scores were within the normal range at baseline and did not suggest a need for clinical intervention. Nonetheless, the absence of disease—in this case anxiety, depression, and stress—does not suggest the presence of health and well-being.30 Although preliminary research has been encouraging, the full importance and impact of how happy, healthy clinicians influence patient care outcomes has yet to be fully understood.31,32
Changes in the measures of compassion and resilience were not statistically significant, but resilience scores trended toward improvement. Lack of change in the SCBC scores may also be attributed to ceiling effects in that respondents already had high compassion scores at baseline.
Limitations of this study include the lack of a control group and the small sample size. Statistical significance should be viewed cautiously because of the multiple comparisons and exploratory nature of the study. In particular, the lack of a control group makes it challenging to know whether improvements were due to the mindfulness intervention or related to normalizing trends over time. Generalizability is limited as study participants were self-selected, may have enrolled because of increased symptoms of burnout and stress, and may be those who find meditation more appealing than do their peers. Further, although there has been debate regarding the extent to which results of various mindfulness interventions are influenced by group effect vs the actual practice of mindfulness,33 the message of “caring for colleagues” that the investigators conveyed throughout this study and the role of “peer interaction and support” are considered inherent aspects of mindfulness teaching and practice.34
Within medical culture, including education, little emphasis has been placed on clinician well-being, and few institutions recognize the impact of burnout on patient care and institutional expenses. Considerable evidence suggests that burnout negatively affects quality of care with profound personal implications, including suicidal ideation.4 Furthermore, physician attrition due to burnout is both disruptive to continuity of patient care and costly to health care organizations.35 There is a paucity of data and few programs that actively address clinician burnout as it relates to personal wellness and quality of care.7 Our findings suggest this intervention is a relatively low cost, collegial, time-efficient way to improve well-being and manage burnout symptoms among primary care clinicians, which has implications for patient care. Nonetheless, additional research, including a randomized controlled trial, is needed to confirm these and previous findings.12–14 Understanding the complex interactions among physician burnout, patient care outcomes, clinician retention, and institutional costs will help health care organizations develop programs that improve work satisfaction, quality of life, and patient care within this demanding profession.
Acknowledgments
We gratefully acknowledge the Mental Insight Foundation and a gift from the Mai Family Foundation for providing support for this project. We also thank the UW Health Mindfulness Program staff for planning and conducting the intervention.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: Two grants from the Mental Insight Foundation and a gift from the Mai Family Foundation provided support for this project.
-
Disclaimer: The funding organizations had no other role in the study.
- Received for publication July 12, 2012.
- Revision received November 29, 2012.
- Accepted for publication December 27, 2012.
- © 2013 Annals of Family Medicine, Inc.
References





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Educational interventions to combat burnout: Are General Practitioners interested? A Qualitative Study
- Role of motivation and well-being indicators in interventions to improve well-being at work among primary care physicians: a systematic review
- Staff wellbeing interventions and its impact on levels of physical intervention in an inpatient unit for individuals with a learning disability: A feasibility study
- The professional resilience of mid-career GPs in the UK: a qualitative study
- Effect of interventions for the well-being, satisfaction and flourishing of general practitioners--a systematic review
- Interventions to reduce occupational stress and burn out within neonatal intensive care units: a systematic review
- Burnout, resilience, and perception of mindfulness programmes among GP trainees: a mixed-methods study
- Mindfulness-based programme for residents: study protocol of a randomised controlled trial
- Physician Well-being
- Resilience in medical doctors: a systematic review
- Effects of mindfulness training on perceived stress, self-compassion, and self-reflection of primary care physicians: a mixed-methods study
- A systematic review of interventions to foster physician resilience
- Barriers, facilitators, and survival strategies for GPs seeking treatment for distress: a qualitative study
- Examining self-reported and biological stress and near misses among Emergency Medicine residents: a single-centre cross-sectional assessment in the USA
- Disenfranchised Grief and Physician Burnout
- Operationalising resilience in longitudinal studies: a systematic review of methodological approaches
- Resilience of primary healthcare professionals: a systematic review
- Mindfulness-based stress reduction for GPs: results of a controlled mixed methods pilot study in Dutch primary care
- BREATHE OUT: A Randomized Controlled Trial of a Structured Intervention to Improve Clinician Satisfaction With "Difficult" Visits
- AMEN in Challenging Conversations: Bridging the Gaps Between Faith, Hope, and Medicine
- In This Issue: Mindfulness in Practice and Policy