


Article Figures & Data
Figures
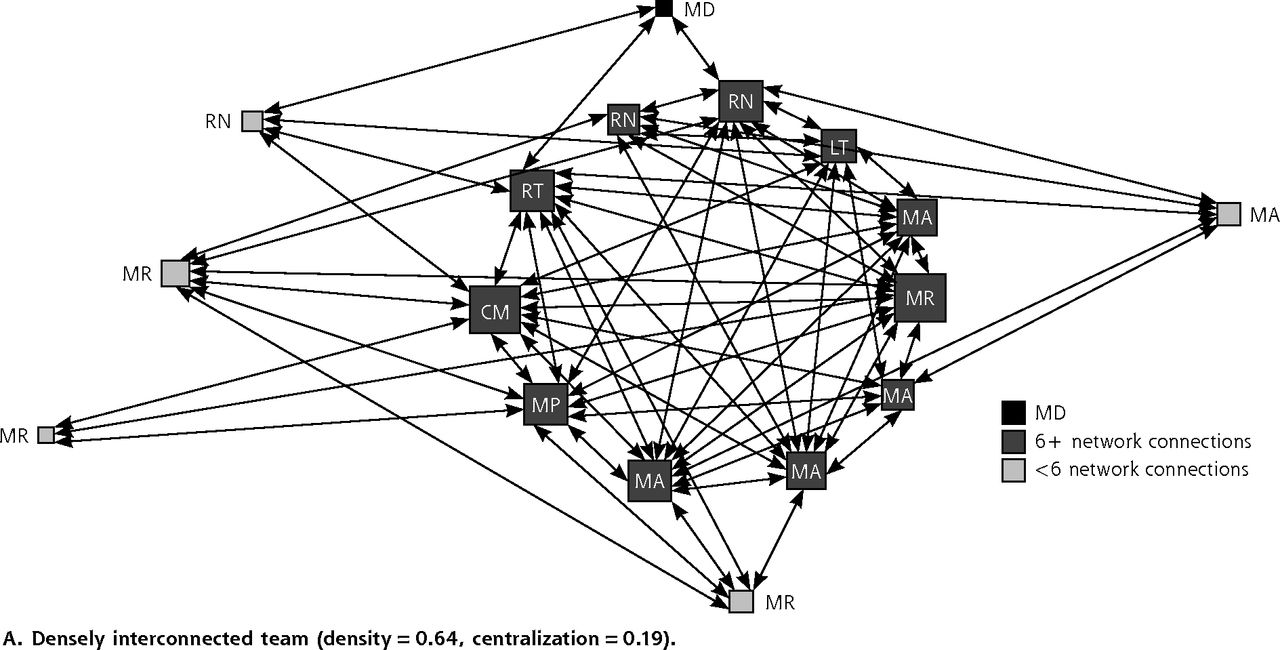
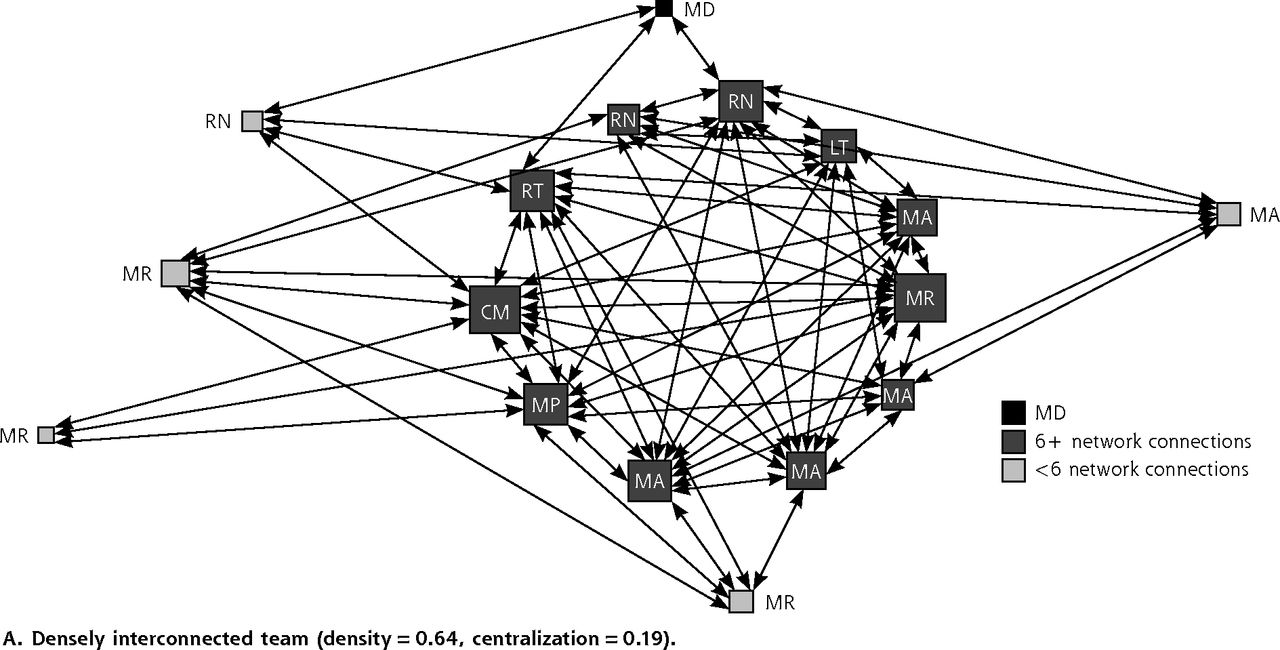
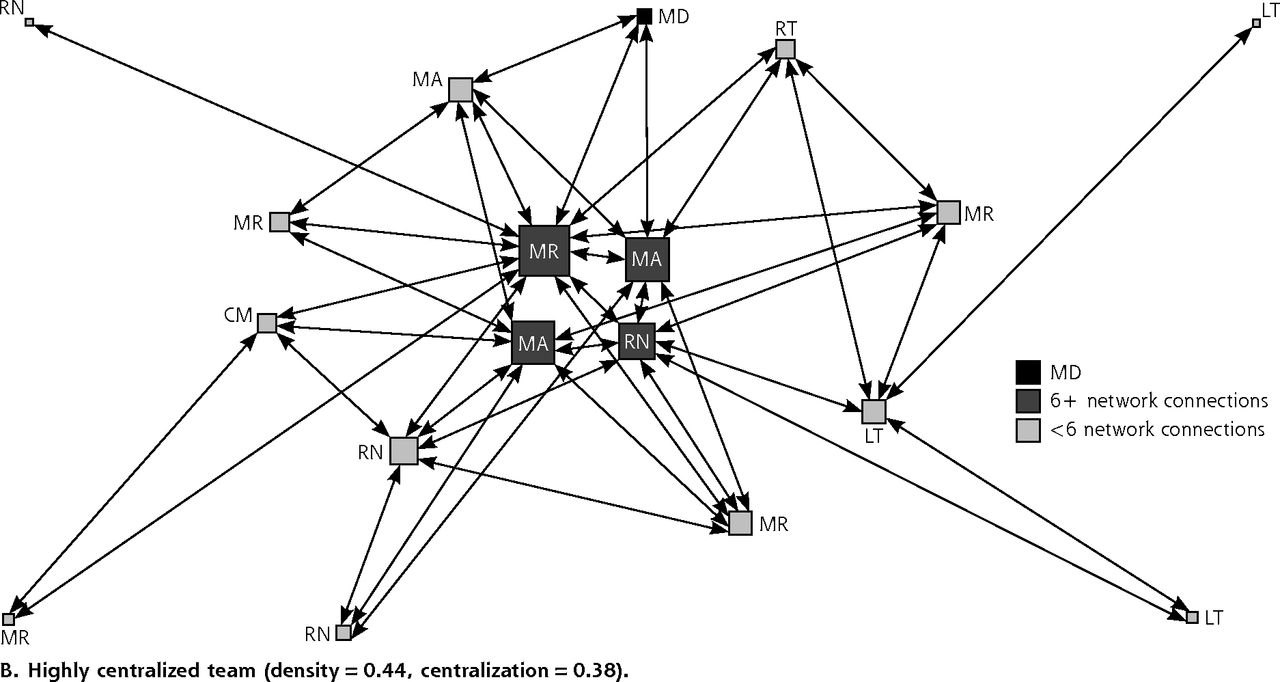
- Figure 1
Primary care team communication networks about patient care.
CM = clinic manager; LT = laboratory technician; MA = medical assistant; MD = physician; MR = medical receptionist; RN = registered nurse; RT = radiology technician.
Note: Symbol size proportional to number of connections.
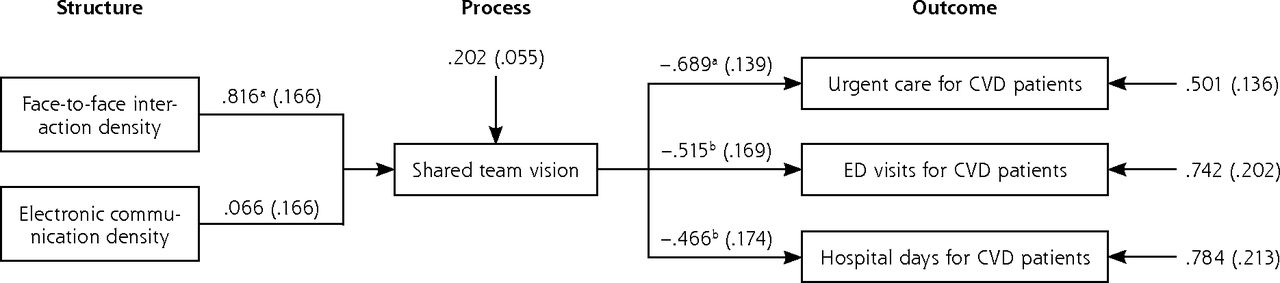
- Figure 2
Structural equation model of team social networks and quality of care for patients with cardiovascular disease (n = 31 primary care teams, n = 7,457 patients).
CVD = cardiovascular disease; ED = emergency department.
Notes: Pathway coefficients between boxes denote the standardized change in end point outcome variable associated with a 1 SD increase in lead predictor variable. By multiplying pathway coefficients between structure, process, and outcome measures, the analysis estimates team social network impact on health care utilization. As an example, for every 1 SD increase in face-to-face interaction density, urgent care visits, emergency department visits, and hospital days decrease by 0.562 (0.816*0.689), 0.420 (0.816*0.515), and 0.380 (0.816*0.466) SDs, respectively.
aP = <.001.
bP = <.01.


Tables
Characteristic No. (%) Mean (SD) Rangea Sex Male 8 (5.2) 7.2 (2.7) 3–11 Female 147 (94.8) 10.8 (4.0) 2–25 Position Physician 20 (12.9) 7.2 (2.3) 3–12 NP/PA 7 (4.5) 7.3 (2.0) 5–11 Clinic manager 6 (3.9) 10.8 (2.8) 8–15 RN 30 (19.4) 12.4 (4.3) 4–25 LPN/MA 29 (18.7) 13.0 (2.7) 9–19 Medical receptionist 38 (24.5) 11.8 (3.0) 5–17 Laboratory/radiology technician 23 (14.8) 8.2 (4.4) 2–18 Other (scribe/phlebotomist) 2 (1.2) 4.5 (0.7) 4–5 Years at clinic ≤1 30 (19.4) 10.1 (4.2) 2–15 1 to 3 43 (27.7) 12.4 (4.4) 4–25 3 to 6 29 (18.7) 9.4 (3.5) 2–18 6 to 10 16 (10.3) 11.1 (3.6) 4–1 >10 37 (23.9) 9.5 (3.1) 4–15 Full-time employment ≤50% 23 (14.8) 7.3 (3.4) 2–14 >50% to 75% 28 (18.1) 9.2 (3.5) 4–17 >75% 104 (67.1) 11.8 (3.7) 4–25 -
LPN = licensed practical nurse; MA = medical assistant; NP = nurse practitioner; PA = physician assistant; RN = registered nurse.
-
Note: Count of incoming communication ties (ie, the number of other team members who report communicating with the individual about patient care on a daily basis).
-
↵a Minimum-maximum.
-
- Table 2
Primary Care Team Characteristics and Outcomes for Patients With Cardiovascular Disease
Characteristic Value Mean (SD) Rangea Primary care teams (n = 31) Social networks variable Team social network density 0.53 (0.12) 0.36–0.77 Team social network centralization 0.29 (0.10) 0.13–0.43 Face-to-face interaction density 0.45 (0.11) 0.31–0.69 Face-to-face interaction centralization 0.28 (0.08) 0.15–0.41 EHR communication density 0.31 (0.08) 0.19–0.46 EHR communication centralization 0.24 (0.07) 0.11–0.43 Team climate (TCI-14) score Shared vision (scale: 0–16)b 12.8 (0.4) 11.6–13.6 Psychological safety (scale: 0–16)b 11.4 (1.1) 8.6–12.3 Task orientation (scale: 0–12)b 8.5 (0.5) 7.5–9.3 Innovation support (scale: 0–12)b 7.9 (0.6) 6.3–8.8 Team characteristics Team size, No. 22.2 (7.5) 12–28 Staff turnover in previous 12 mo, % 19 … Patient panel outcomes in past 12 mo Team patients (n = 7,457) With controlled LDL cholesterol (<100 mg/dL), % 39 … With controlled blood pressure (<130/80 mm Hg), % 71 … Health care use per patient in patient panel Urgent care visits, No. 0.10 (0.44) … Emergency department visits, No. 0.24 (1.20) … Hospital days, No. 0.65 (4.44) … Medical costs, US$ 1,241 (7,538) … - Table 3
Hierarchical Modeling of the Association Between Team Social Networks and Outcomes for Panel of Patients With Cardiovascular Disease
Variable BP Control OR (95% CI) LDL Cholesterol Control OR (95% CI) UC Visits RR (95% CI) ED Visits RR (95% CI) Hospital Days RR (95% CI) Cost ($)β (SE) Reduced form model Team social network densitya 1.14 (0.98–1.33) 1.13 (0.97–1.31) 0.28b (0.19–0.40) 0.58c (0.42–0.80) 0.64b (0.51–0.80) −516b (129) Team social network centralizationa 1.00 (0.84–1.19) 0.94 (0.80–1.11) 3.07b (2.09–4.51) 1.70c (1.23–2.35) 1.47c (1.14–1.89) 519c (143) Full modeld Team social network densitya 1.15 (0.99–1.34) 1.14 (1.00–1.31) 0.95 (0.55–1.66) 0.98 (0.50–1.89) 0.62b (0.50–0.77) −556b (115) Team social network centralizationa 1.03 (0.85–1.25) 0.93 (0.79–1.08) 1.20 (0.79–1.81) 1.33 (0.83–2.13) 1.45c (1.09–1.94) 506c (155) -
BP = blood pressure; ED = emergency department; LDL = low-density lipoprotein; OR = odds ratio; RR = rate ratio; SE = standard error; UC = urgent care.
-
Note: There were 31 primary care teams and 7,457 patients who had cardiovascular disease.
-
↵a Team social network interaction related to daily face-to-face and/or EHR communication connections about patient care in a team.
-
↵b P <.001.
-
↵c P <.01.
-
↵d Patient-level covariates entered in the full model were sex, age, age squared, race/ethnicity, insurance, and comorbidity.
-
- Table 4
Three-Level Hierarchical Model of the Association Between Face-to-Face and EHR Communication Networks and Outcomes for Patients With Cardiovascular Disease (n = 31 teams, n = 7,457 patients)
Variable BP Control Adj OR (95% CI) LDL Cholesterol Control Adj OR (95% CI) UC Visits Adj RR (95% CI) ED Visits Adj RR (95% CI) Hospital Days Adj RR (95% CI) Cost (US$) Adj β (SE) Primary care team social networks Face-to-face interaction density 1.19 (0.89–1.59) 1.17a (1.00–1.37) 0.34a (0.12–0.98) 0.28b (0.12–0.63) 0.63 (0.40–1.00) −594a (240) EHR communication density 0.96 (0.71–1.29) 0.85a (0.72–1.00) 1.64 (0.71–3.81) 2.34a (1.10–4.97) 1.010. (63–1.60) 60 (247) Patient characteristics Male 1.52c (1.23–1.87) 1.67c (1.51–1.88) 0.79b (0.67–0.93) 0.94 (0.85–1.04) 0.97 (0.91–1.03) 118 (180) Age 0.99b (0.99–1.00) 1.01c (1.01–1.02) 0.96c (0.95–0.97) 0.98c (0.97–0.99) 0.99 (0.98–1.00) −24b (8) Age-squared (÷10) 1.00 (0.99–1.01) 0.97c (0.96–0.98) 1.00 (0.99–1.01) 1.01c (1.00–1.01) 1.00 (0.99–1.01) −1 (3) Non-Hispanic White 0.58 (0.33–1.01) 1.22 (0.88–1.69) 0.64b (0.49–0.84) 0.68c (0.56–0.81) 1.52c (1.27–1.83) 205 (540) White Hispanic 2.01 (0.97–4.18) 1.48 (0.91–2.39) 1.16 (0.78–1.73) 1.17 (0.87–1.57) 0.50c (0.34–0.74) −453 (828) Black 0.72 (0.49–1.07) 0.86 (0.56–1.32) 1.79a (1.05–3.06) 1.89a (1.03–3.47) 0.80 (0.32–2.00) −160 (705) Private insurance 4.71c (2.44–9.12) 1.69c (1.36–2.10) 1.88b (1.27–2.79) 0.71c (0.59–0.85) 0.46c (0.42–0.51) −1,135b (359) Medicaid 2.64a (1.04–6.73) 1.40 (0.98–1.99) 3.18c (2.03–4.97) 1.45b (1.15–1.84) 0.81a (0.69–0.95) −588 (581) Medicare 3.65c (1.90–7.04) 2.24c (1.81–2.79) 1.52a (1.01–2.29) 1.51c (1.28–1.78) 0.84c (0.77–0.91) −817a (364) Charlson comorbidity index 1.14c (1.09–1.20) 1.23c (1.20–1.26) 1.06b (1.02–1.10) 1.32c (1.29–1.34) 1.36c (1.34–1.37) 690c (47) -
Adj OR = adjusted odds ratio; Adj RR = adjusted rate ratio; Adj β = adjusted regression coefficient; BP = blood pressure; ED = emergency department; EHR = electronic health record; LDL = low-density lipoprotein; SE = standard error; UC = urgent care.
-
Notes: Confidence intervals rounded to 2 significant digits. Statistically significant intervals for OR and RR do not contain 1.
-
↵a P <.05.
-
↵b P <.01.
-
↵c P <.001.
-
The Article in Brief
Effects of Primary Care Team Social Networks on Quality of Care and Costs for Patients With Cardiovascular Disease
Marlon P. Mundt , and colleagues
Background Cardiovascular disease (CVD) is the leading cause of death and disease in the US. Primary care teams, which provide support and share responsibilities for patient care, offer a unique opportunity to improve quality and lower medical costs for patients with CVD. This study evaluates the association between primary care team communication, interaction, and coordination (i.e., social networks), quality of care, and costs for patients with CVD.
What This Study Found Primary care teams that are more interconnected, less centralized, and have a shared team vision are better positioned to deliver high-quality cardiovascular disease care at a lower cost. Teams with more members reporting daily interactions with a greater number of team members show better quality of care, with a 38 percent reduction in hospital days and, on average, $516 less spent per patient in the previous 12 months. The study findings suggest that teams with more daily face-to-face interactions have fewer urgent care and emergency department visits and $594 less spent in medical costs per patient in the previous 12 months.
Implications
- In this study, a team's shared vision of goals and expectations mediates the relationship between social network structures and patient quality of care outcomes.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Representation of the hierarchical and functional structure of an ambulatory network of medical consultations through social network analysis, with an emphasis on the role of medical specialties
- Exploring the structure of social media application-based information-sharing clinical networks in a community in Japan using a social network analysis approach
- Professional Communication Networks and Job Satisfaction in Primary Care Clinics
- Differences in Team Mental Models Associated With Medical Home Transformation Success
- Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-Motion Observations
- In This Issue: Developing and Amplifying the Effectiveness of the Primary Care Workforce