


Abstract
PURPOSE Loneliness has important health consequences. Little is known, however, about loneliness in primary care patient populations. This study describes the prevalence of loneliness in patients presenting for primary care and associations with self-reported demographic factors, health care utilization, and health-related quality of life.
METHODS We conducted cross-sectional surveys of adults presenting for routine care to outpatient primary care practices in 2 diverse practice-based research networks. The 3-item University of California, Los Angeles Loneliness Scale was utilized to determine loneliness.
RESULTS The prevalence of loneliness was 20% (246/1,235). Loneliness prevalence was inversely associated with age (P <.01) and less likely in those who were married (P <.01) or employed (P <.01). Loneliness was more common in those with lower health status (P <.01), including when adjusting for employment and relationship status (odds ratio [OR] = 1.05; 95% CI, 1.03-1.07). Primary care visits (OR = 1.07; 95% CI, 1.03-1.10), urgent care/emergency department visits (OR = 1.24; 95% CI, 1.12-1.38), and hospitalizations (OR = 1.15; 95% CI, 1.01-1.31) were associated with loneliness status. There was no significant difference in rates of loneliness between sexes (P = .08), racial categories (P = .57), or rural and urban respondents (P = .42).
CONCLUSIONS Our findings demonstrate that loneliness is common in primary care patients and is associated with adverse health consequences including poorer health status and greater health care utilization. Further work is needed to understand the value of screening for and using interventions to treat loneliness in primary care.
INTRODUCTION
Loneliness, defined as the internal perception of inadequacy of personal relationships,1 has detrimental effects on health and is increasingly acknowledged as a public health crisis. The prevalence of loneliness is recognized to be high, and reports range from 7%2 to 49%3 depending on the country of origin, measurements used, age range, and subpopulations queried. In the United States, it has been reported that over one-third of the general population aged over 45 years may experience loneliness.4
Loneliness is connected to poor physical and mental health outcomes, including increased risk of hypertension,5 cardiovascular disease and stroke,6,7 depression,8 cognitive decline and Alzheimer’s disease,9 and all-causes of mortality.10 In fact, loneliness may be as deleterious as smoking 15 cigarettes per day.6 While much of the literature and popular belief has focused on the relationship between loneliness and the elderly,11 increasing attention is being paid to the patterns of social relationships that begin earlier in life and persist throughout a lifetime.12,13 Given the identified health threats, policy makers have called for research on loneliness in diverse settings, increased consideration from the health care community, and novel interventions.14,15
While studies contribute to our understanding of the reach of loneliness, less is known about the appropriate clinical response, particularly with respect to primary care. In 2014, the National Academy of Medicine called for clinicians to regularly collect information on social connections and social isolation recognizing the negative implications on quality of life and health.16 Few clinicians, however, have begun collecting these data. While valid scales for measuring loneliness exist,17 they are not regularly used in primary care practices. Moreover, the role of primary care in treating loneliness remains unclear.
Therefore, if the goal is to address loneliness within primary care, it is essential to understand the characteristics and behaviors of lonely individuals in this setting. This study describes the prevalence of loneliness in adults presenting to outpatient primary care practices for routine care and examines associations between loneliness and self-reported demographic factors, health status, and health care utilization.
METHODS
This study was a cross-sectional survey of adult patients presenting for outpatient care from April 2017 through January 2018 in 2 practice-based research networks, the State Networks of Colorado Ambulatory Practices and Partners (SNOCAP) and the Virginia Ambulatory Care Outcomes Research Network (ACORN). The study was approved by the Colorado Multiple Institutional Review Board and Virginia Commonwealth University Institutional Review Board.
Setting and Population
SNOCAP is a collaborative of 5 practice-based research networks in Colorado that includes more than 600 primary care clinicians and represents all major demographic populations in Colorado. ACORN, the only practice-based research network in Virginia, consists of over 500 primary care clinicians and includes over 150 rural, suburban, and urban practices. All practices in the participating networks were electronically notified of the study through e-mails and newsletters and were given an opportunity to participate; interested practices e-mailed research coordinators to sign up for the study. Additionally, the research team personally solicited practices likely to be interested collaborators based upon prior experience.
Sixteen practices participated in the study, 7 ACORN-affiliated and 8 SNOCAP-affiliated practices. The participating ACORN practices were located in Richmond, Fairfax, and Front Royal, serving predominently urban underserved, suburban and affluent, and rural populations, respectively. Participating SNOCAP practices throughout metro Denver, Boulder, and across rural Eastern Colorado, similarly serve diverse populations.
Participants were recruited by convenience sampling. Patients aged 18 years and older (the upper limit being people aged 89 years in Colorado due to institutional review board restrictions) were asked to complete a paper survey before their appointment. Patients who were unable to read English were excluded. At ACORN-affiliated practices, student and research coordinators approached all adult patients with an office visit during the study period to complete the survey. Patients were approached on consecutive days until 100 responses per practice were obtained. Due to availability of resources, at SNOCAP-affiliated practices, front desk staff offered the surveys to all eligible patients until either 100 responses were collected or until the end of a consecutive 4 to 7 day collection period, whichever occurred first. Patients were not reimbursed for survey completion and participation was blinded to the clinician. Given the nature of our deidentified study methods, we did not collect overall clinic response rate estimates or monitor if participants completed the survey more than once.
Measures
Survey questions included validated measures of loneliness as well as sociodemographics, health-related quality of life, and health care utilization (Supplemental Appendix, available at http://www.AnnFamMed.org/content/17/2/108/suppl/DC1/). Demographic information included age, sex, zip code, marital status, employment status, and current relationship status (see Supplemental Appendix for survey instrument). Respondent zip code data was used to interpret urban vs rural status based upon the United States Department of Agriculture Rural-Urban Commuting Area Codes.18
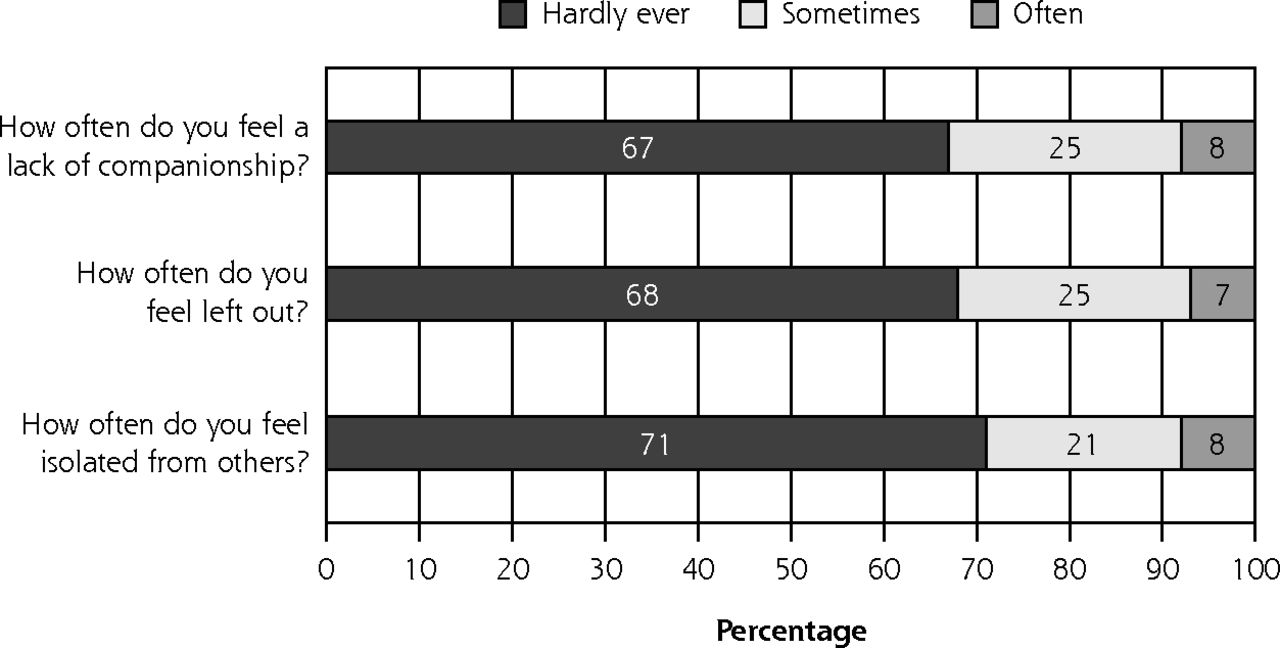
We used the 3-item University of California, Los Angeles (UCLA) Loneliness Scale to measure loneliness.19 This shortened screening tool has illustrated reliability and correlation to the full 20-item Revised UCLA Loneliness Scale, and addresses lack of companionship, feeling left out, and feelings of isolation from others.20 Respondents replied on a 3-point scale from never, sometimes, or often, corresponding to scores of 1-3 for each item, and received a total score of 3-9. A total score of 6 or above was considered lonely.21
Participants were asked to report on their health using Healthy Days Measures from the Centers for Disease Control and Prevention measurement of Health-Related Quality of Life.22 Overall health status was measured by responses to “in general, how would you rate your health” on a 5 point scale (1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent). Respondents provided an estimate of the number of days that his or her physical or mental health was not good during the prior month. The patient questionnaire also included 3 questions asking about emergency department visits, primary care visits, and hospitalizations within the prior 12 months. Question structure was based upon the Centers for Disease Control and Prevention National Health Interview Survey.23
Statistical Analysis
Continuous measurements were summarized with means and standard deviations (SD), while categorical measurements were summarized with frequencies and percentages. Differences in patient characteristic distributions between health networks were assessed using χ2 tests. Associations between the categorical loneliness classification and patient characteristics were evaluated with generalized linear mixed models, with the loneliness classification modeled as a binary outcome against a single fixed effect for each patient demographic, and with Froma practice-level random effect to account for inter-practice variability.
Unadjusted and adjusted odds ratios were estimated between patient characteristics and loneliness classification using generalized linear models. Unadjusted estimates were obtained by separately fitting each characteristic (sex, age, race, employment, relationship, location, health) against the binary loneliness classification, with a practice-based random effect to account for between-practice variability. Adjusted estimates were obtained using 2 approaches: by jointly modeling all characteristics against loneliness classification, and by jointly modeling all significant characteristics against the loneliness classification, though omitting the practice-based random effect due to lack of significance. In both cases, some classifications with sparse data (eg, other, prefer not to answer) were removed and some levels with similar meanings and similar loneliness classifications (eg, widowed, separated, divorced; excellent or very good health) were combined to simplify analysis and interpretation. The GLIMMIX procedure in the SAS statistical software package, version 9.4 (SAS Institute, Inc) was used for these analyses.
RESULTS
From 16 practices, 1,246 patients completed the survey, with 1,235 patients responding to the loneliness items on the questionnaire. The mean age of study respondents was 52 years (SD = 16.5). The majority of respondents were female (63%), white (71%), and lived in an urban setting (77%). About one-half were married (54%) and employed full time (45%). Colorado and Virginia populations were significantly different across every demographic category (Table 1).
Patient Demographics By State Health System (N = 1,246)
Loneliness Prevalence
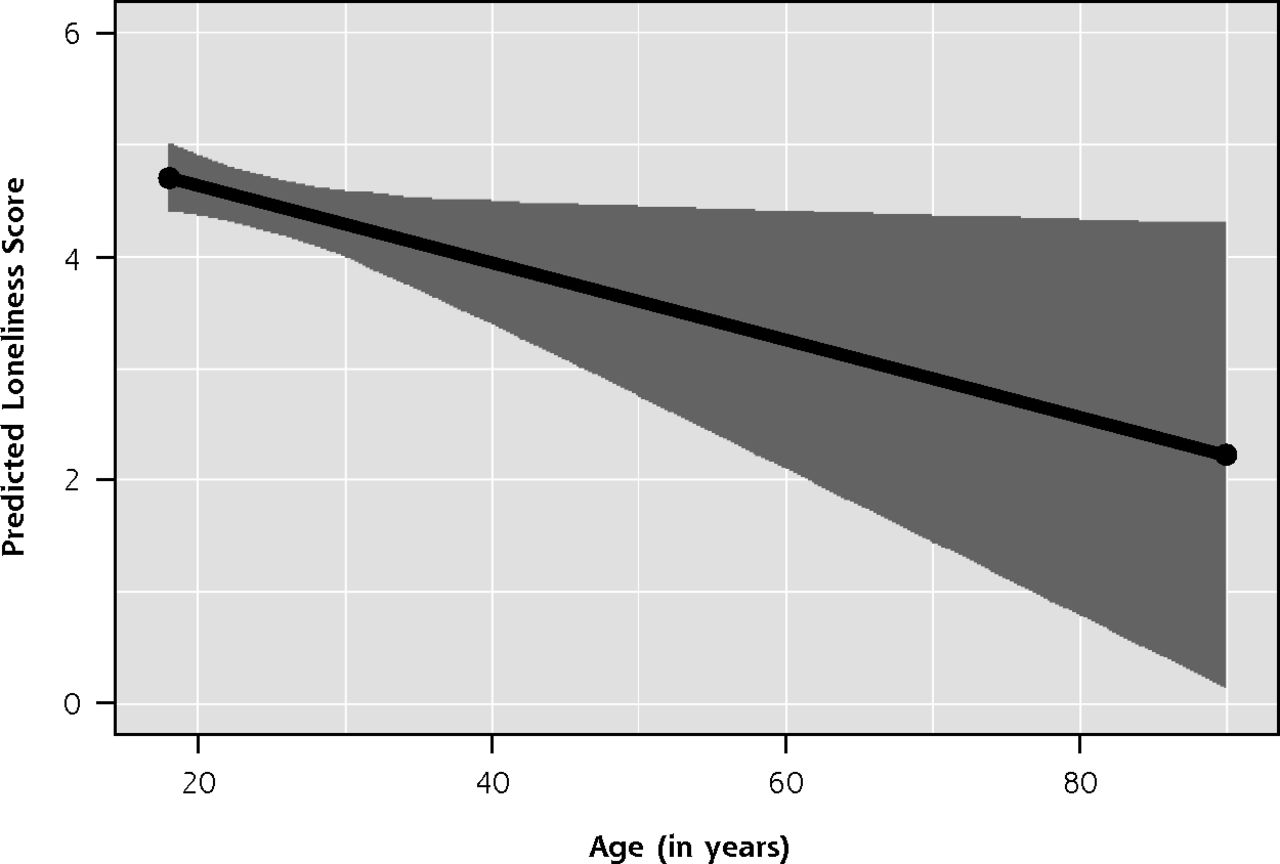
The overall prevalence of loneliness was 20% (246/1,235). The prevalence varied between states, with 22% of patients from Virginia reporting loneliness compared with 17% of patients from Colorado (P = .04). The mean score on the 3-item UCLA Loneliness Scale was 4.2 (SD = 1.6), with about one-third of respondents “sometimes” or “often” feeling lack of companionship, left out, or isolated from others (Figure 1). The prevalence of loneliness generally decreased with age, as 33% (18/58) of respondents aged <25 years reported loneliness compared with 11% (34/307) of those aged >65 years (P <.01). Similarly, the mean loneliness score linearly declined from 4.7 (standard error [SE] = 0.16) at age 18 years to 2.9 (SE = 0.75) at age 80 years (P = .03) (Figure 2).
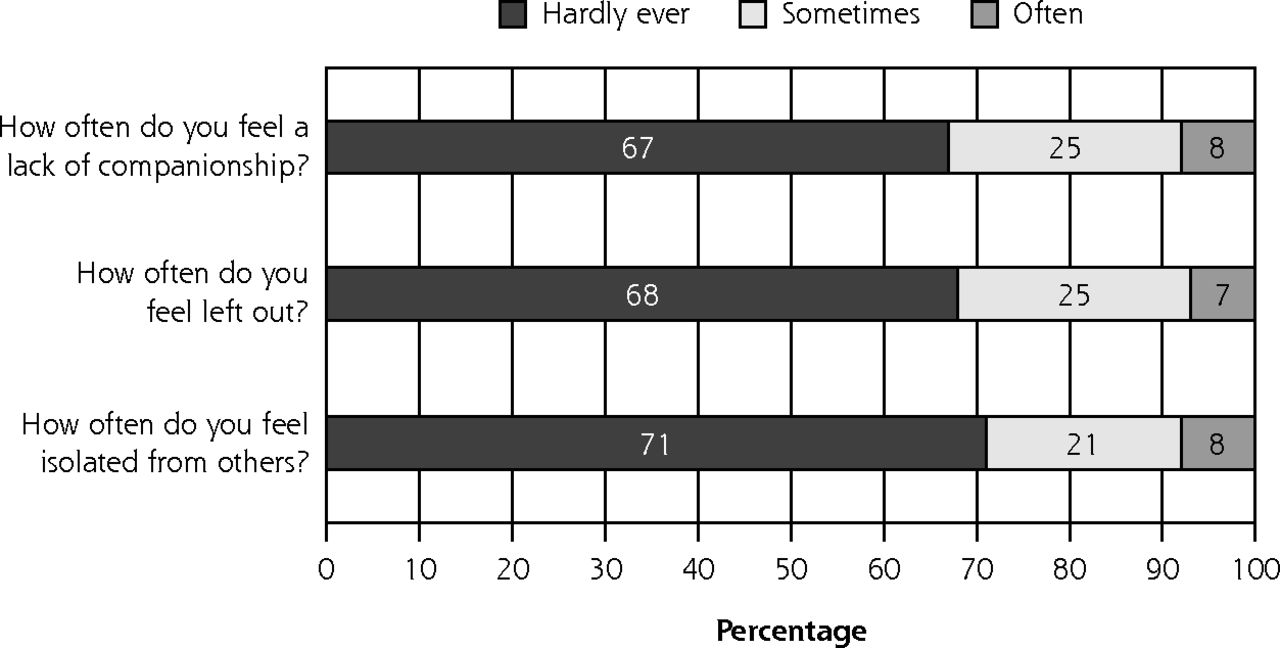
Percentage of responses to the 3-item UCLA Loneliness Scale (N = 1,235).
UCLA = University of California, Los Angeles.
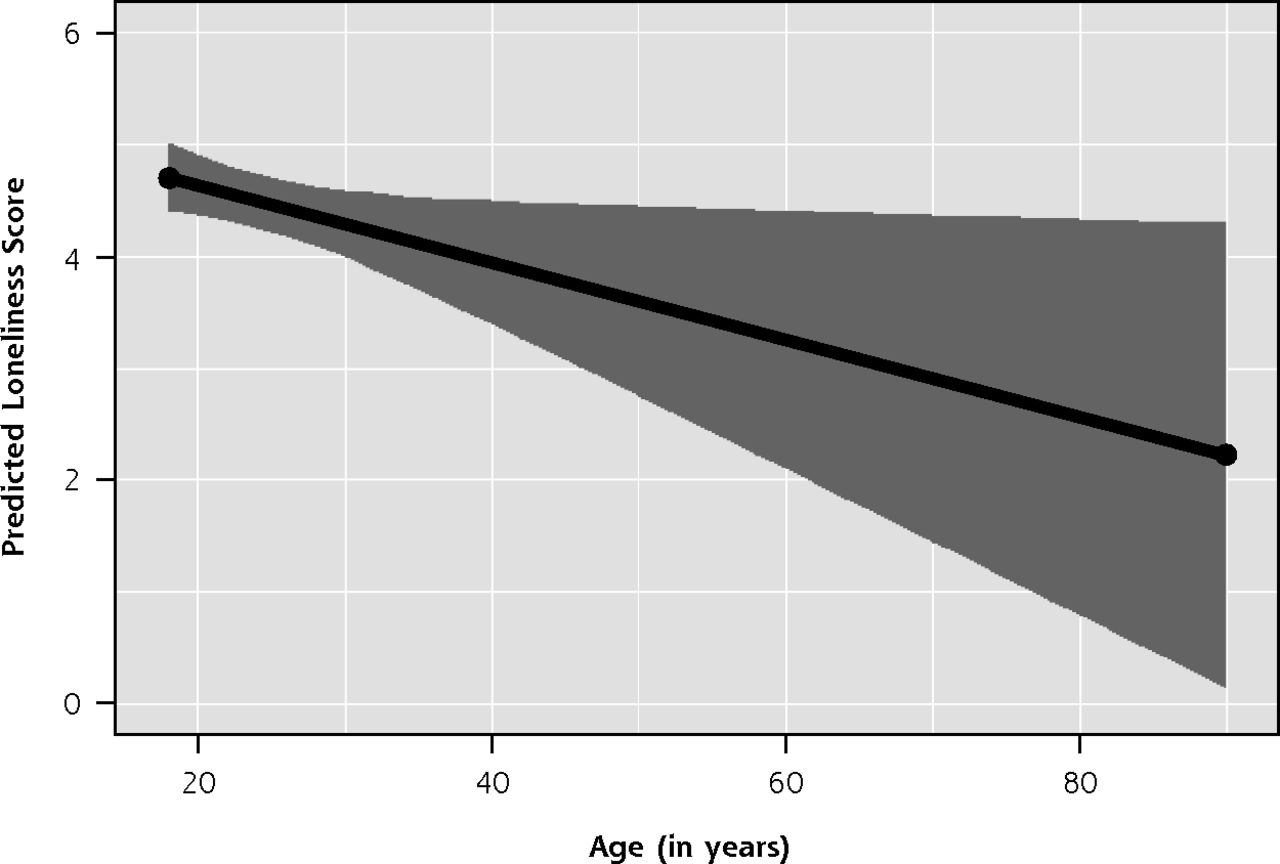
Predicted loneliness score vs age (18-<90 y) (N = 1,235).
Note: The black line illustrates a linear decrease in loneliness scores with increasing age and the gray area represents the 95% CI.
Loneliness and Demographics
As illustrated in Figure 3, loneliness was significantly associated with relationship status and employment status. Divorced, separated, widowed, and never been married respondents illustrated a significantly higher prevalence of loneliness (P <.01). Additionally, individuals who were unemployed or disabled experienced significantly higher levels of loneliness (P <.01). There was not a significant association between race/ethnicity (P = .57) or respondent sex (P = .08) and loneliness score. Finally, there was no significant association between location and loneliness scores (P = .42), with the loneliness prevalence similar in rural (17%) and urban areas (21%).
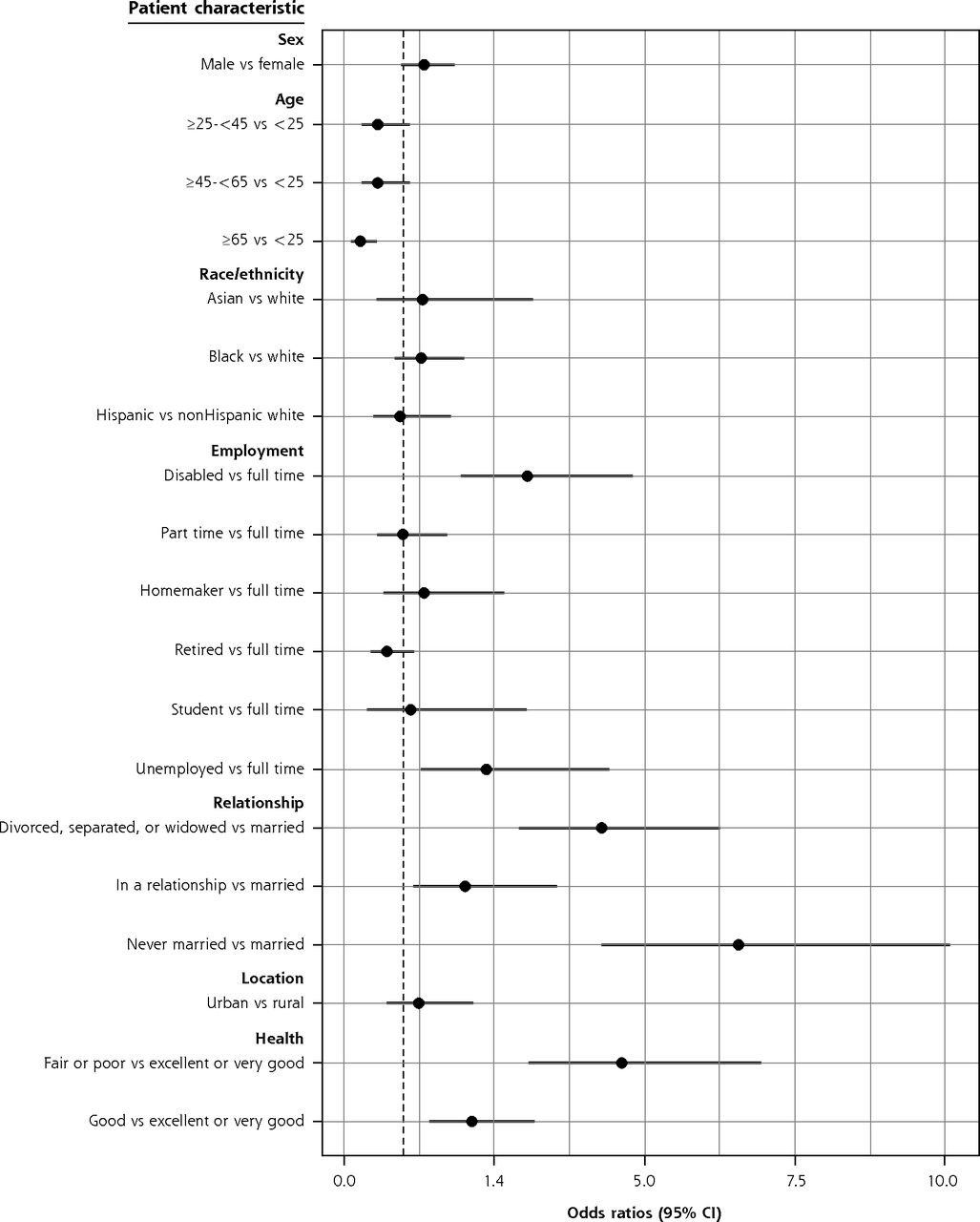
Unadjusted odds ratios for participant characteristics and loneliness (N = 1,246).
Note: Forest plot of the unadjusted odds ratio (black circles) and 95% CI (horizontal lines).
Loneliness, Quality of Life, and Utilization
Loneliness classifications were significantly associated with respondent health classification and health status. Respondents in poor health were more likely to report loneliness (P <.01). As illustrated in Figure 3, there was an inverse relationship with loneliness and respondent health status, from poor to excellent health (P <.01). There was also a significant association between the number of days with poor physical or mental health in the prior month and loneliness (P <.01) (Table 2). This association remained significant when adjusting for all patient characteristics (OR = 1.04; 95% CI, 1.02-1.06) or employment and relationship status (OR = 1.05; 95% CI, 1.03-1.07). A high level of loneliness was positively associated with all 3 utilization measures, including the number of visits to the primary care office, the number of hospitalizations, and the number of emergency department or urgent care visits (Table 2). When adjusting for employment and relationship status, the association of loneliness with primary care visits or emergency department/urgent care visits remained significant (Table 2).
Nonlonely and Lonely Respondents Health Status and Utilization (N = 1,226)
DISCUSSION
We found that the prevalence of loneliness is 20% in adult English-reading patients participating in routine outpatient primary care, with younger populations carrying a significantly higher burden. In addition to demographic factors such as relationship status and employment status, positive loneliness screens were associated with heath care utilization and poor self-rated health. The relationship with poor health status was significantly maintained even when adjusting for patient characteristics.
Our findings both support and enhance other loneliness research currently in the literature, notably adding the perspective of a broadly representative primary care patient population. In other studies focusing on the general population or subset clinical groups, relationship status,24 poor subjective health,25–27 and a variety of health care utilization measures including primary care visits,28,29 emergency hospitalizations,30 and emergency department visits in elders31 have been associated with loneliness. Although few prior studies have shown a higher prevalence of loneliness in rural settings,26 in our population the prevalence of loneliness did not differ significantly with rurality, suggesting that loneliness is constant among diverse clinical settings. While the prevalence varied between Colorado and Virginia, this is almost certainly explained by the substantially different patient populations included in each state. Importantly, we confirmed that the prevalence of loneliness in those presenting for care is similar to that of the general population.32,33 In other words, we do not see evidence that lonely individuals isolate themselves from primary care. This indicates that the primary care setting has the potential to identify solutions and implement interventions.
Similar to our study, there have been other reports that illustrate an equal or greater prevalence of loneliness in adolescents.34,35 The underlying cause for this level of prevalence in adolescents is not well defined, but may be related to significant transitions during this age period including detachment and independence from parents,1 low self-confidence,36 and concerns with self-identity and peer status.37 Generational differences in communication may also play a role in the impact and experience of loneliness. Given the broad age ranges included in this analysis, future studies can assess whether these results can be replicated within more narrow age cohorts among those presenting to primary care practices.
Although the role of screening and integration into routine care remains unclear, there is emerging data that the health care system has a role in helping patients address loneliness. In the clinical setting, interventions have included social support provided by individual or group counseling,38,39 social recreation interventions offered at mental or clinical health centers,40 telephone-based social support or social cognitive training delivered by health care providers,41,42 and even hospital-based social skills training.43 While many of these interventions are small and not replicated, they have illustrated significant changes in loneliness scores.44,45 Importantly, patients report the desire to talk to their primary care clinician about loneliness.46 Therefore, more attention needs to be placed on the role of the physician and the clinical setting in screening for and mitigating loneliness, the methodological rigor of subsequent studies, and the evaluation of the impact on quality of life and health outcomes.
Several limitations to our study need to be acknowledged. First, due to resource constraints our survey was limited to English-reading participants, creating a bias toward including those able to comprehend standardized research instruments and excluding patients with lower socioeconomic status who may be at high risk for loneliness. In fact, based upon prior literature indicating that many immigrant and refugee populations have high loneliness, a more inclusive population may have increased the loneliness prevalence in our study.47,48 Second, because we did not collect data on nonparticipants, we cannot compare respondents to the general practice population and thus respondents may differ. Additionally, although we surveyed distinct regions, results could differ if this study is repeated in other states or regions. Finally, as this is a cross-sectional study, we cannot establish causation between loneliness and risk factors, nor can we know whether loneliness preceded low self-reported health status and higher health care utilization (or vice versa). Additional research is warranted.
CONCLUSION
In conclusion, our study suggests loneliness is common in primary care patients. Our findings contribute to the growing body of evidence demonstrating that loneliness is widespread and associated with poor health. It is clear this public health concern is unlikely to find a resolution without concentrated, collaborative effort and undertaking. Recognizing that loneliness is present in diverse clinical settings allows for increased opportunities to identify creative, sustainable solutions. In response, primary care clinicians need to prioritize understanding social connections in risk assessment and the needs of lonely patients in clinical practice. Additional research is needed to understand the role of primary care in supporting lonely patients and further addressing loneliness, including screening and individualized approaches to intervention delivery.
Footnotes
Conflicts of interest: authors report none.
Supplemental Materials: Available at http://www.AnnFamMed.org/content/17/2/108/suppl/DC1/.
- Received for publication August 16, 2018.
- Revision received November 4, 2018.
- Accepted for publication November 28, 2018.
- © 2019 Annals of Family Medicine, Inc.
References





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Retrospective cross-sectional study examining the association between loneliness and unmet healthcare needs among middle-aged and older adults using the Canadian Longitudinal Study of Aging (CLSA)
- Randomised controlled trial of the Caring Connections intervention to reduce loneliness and perceived social isolation in persons with spinal cord injuries and disorders: study protocol
- A New Pandemic of Loneliness
- Primary care-based interventions addressing social isolation and loneliness in older people: a scoping review
- Social isolation and psychological distress among southern US college students in the era of COVID-19
- Loneliness, Burnout, and Other Types of Emotional Distress Among Family Medicine Physicians: Results From a National Survey
- Stroke survivors experience elevated levels of loneliness: a multi-year analysis of the National Survey for Wales
- Children as frequent attenders in primary care: a systematic review
- Geographic Characteristics of Loneliness in Primary Care
- In This Issue: Minding the Gaps