


Abstract
PURPOSE Access to health care is a long-standing concern for rural patients; however, administrative measures fail to capture the subjective patient experience of accessing health care. The purpose of this review was to synthesize the qualitative literature on patient and caregiver experiences of accessing health care services for chronic disease management among US residents of rural areas.
METHODS We searched Embase, MEDLINE, PsycInfo, CINAHL, and Scopus to identify qualitative studies published during 2010-2019. A thematic synthesis approach was used to analyze findings from included studies.
RESULTS A total of 62 studies involving 1,354 unique participants were included. The largest share of studies (24.2%) was focused on the experience of patients with cancer, followed by behavioral health (16.1%), HIV and AIDS (14.5%), and diabetes (12.9%). We identified 4 primary analytic themes of barriers and facilitators associated with the experience of accessing health care services for chronic disease management in rural areas: (1) navigating the rural environment, (2) navigating the health care system, (3) financing chronic disease management, and (4) rural life (ie, common elements of a distinct “rural” way of thinking and behaving).
CONCLUSIONS In this comprehensive review, we found that important cultural, structural, and individual factors influenced the rural patient’s experience of health care access and use, including barriers and facilitators posed by geographic and built environments, and distinct rural mores. Our findings can inform policies and programs that both facilitate structural aspects of access and include culturally appropriate interventions.
- rural health
- health care access
- barriers
- facilitators
- chronic disease management
- systematic review
- qualitative research
- vulnerable populations
- public health
INTRODUCTION
Nearly 1 in 5 people in the United States live in rural areas.1 Chronic health conditions are both more prevalent and associated with higher rates of disease-attributable mortality among rural residents compared with their urban and suburban counterparts.2-5 At the same time, people dwelling in rural areas face immense challenges to accessing the health care services needed to prevent, diagnose, and manage chronic health conditions.
The concept of access to health care, broadly defined as the opportunity and ability to use health care resources and services, is often focused on supply-demand relationships and other quantifiable measures of availability and use.6 Administrative measures, however, fail to capture the subjective patient experience of accessing health care, which may include important cultural, structural, and individual or interpersonal factors that influence decisions to seek (or not seek) care, the perceived quality of the care received, and treatment adherence. In addition, the experiences of rural residents as they access health care services are not readily represented in the research literature for multiple reasons, including the heterogeneity of rural settings and lifestyles, as well as logistic difficulties in recruiting and retaining study participants from outlying areas.7,8
Consequently, there is a critical gap in current understanding of factors that influence health care access among rural patients. The objective of this study was therefore to conduct a comprehensive systematic review and thematic synthesis of the qualitative literature on rural patient experiences of accessing health care for chronic health conditions. Beyond contributing to the research base, the insight gleaned can be used to inform the development of future interventions to improve the experiences of rural patients with chronic health conditions as they access health care services.
METHODS
We used a thematic synthesis methodology to inform our search approach, quality appraisal, and analysis.9 Reporting of this review follows the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement guidelines.10,11
Search Strategy
We ran a comprehensive search strategy on October 4, 2019 to identify all available empirical studies published in peer-reviewed journals from January 2010 through and including October 2019 indexed in the following databases: Embase, MEDLINE, PsycInfo, CINAHL, and Scopus (Supplemental Appendix 1).
Study Inclusion Criteria
Eligible studies were those describing original research published in English. We used the following additional key inclusion criteria: participants were adult patients, their unpaid caregivers, or both; the study used qualitative methodology; participants lived in US rural settings; and participants had at least 1 diagnosed chronic health condition.
Screening and Data Extraction
All records were reviewed in duplicate in phases by title and abstract, full text, and data extraction (see Supplemental Appendix 2 and Supplemental Appendix 3 for protocol and review forms). All study screening and data extraction activities were conducted using DistillerSR (Evidence Partners).
Assessment of Study Quality
The first author (E.H.G.) assessed each included study using the Critical Appraisal Skills Program (CASP) qualitative research checklist (Supplemental Table 1).12 Studies were not weighted or excluded based on quality rating.
Analysis
We followed a 3-step process of thematic synthesis consistent with methods detailed by Thomas and Harden.9 First, we performed line-by-line coding of text in the Results sections of articles reporting primary studies. Codable text included quotes from participants, summaries of participant responses, and interpretive statements by the study authors. A coding team of 4 authors (E.H.G., D.L.G., A.G.B., S.V.) developed an initial codebook inductively (ie, through initial reading of included studies) and deductively, based on known dimensions of health care access in rural areas (eg, transportation, clinician availability).
Next, the coding team used this preliminary codebook to perform line-by-line coding on a subset of studies and met to compare notes and refine the codebook in an iterative process over several weeks. Once the codebook was deemed satisfactory, included studies were independently coded. The coding team met weekly to discuss progress, resolve disagreements, and make additional refinements to the codebook. All coding was performed using NVivo, version 11 (QSR International).
After the team completed coding of all included studies, we developed descriptive themes inductively through mapping of codes into similar domains in an iterative process of reexamining and regrouping of codes. Higher-level analytic themes were then formed in a similar process by grouping these secondary descriptive themes into similar conceptual domains in an iterative process of reflection and interpretation.
RESULTS
Studies Characteristics
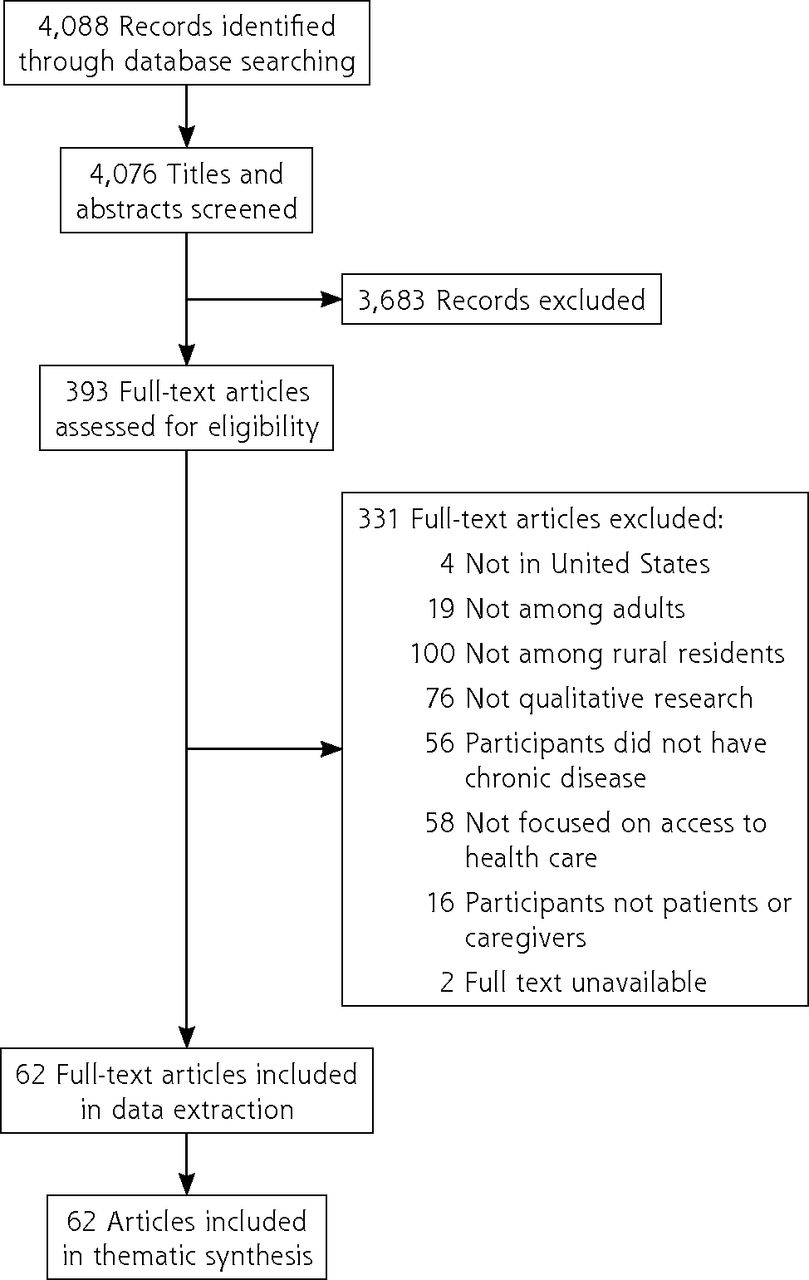
A total of 62 original research studies involving 1,354 unique participants were included in the data extraction and thematic synthesis (Figure 1).
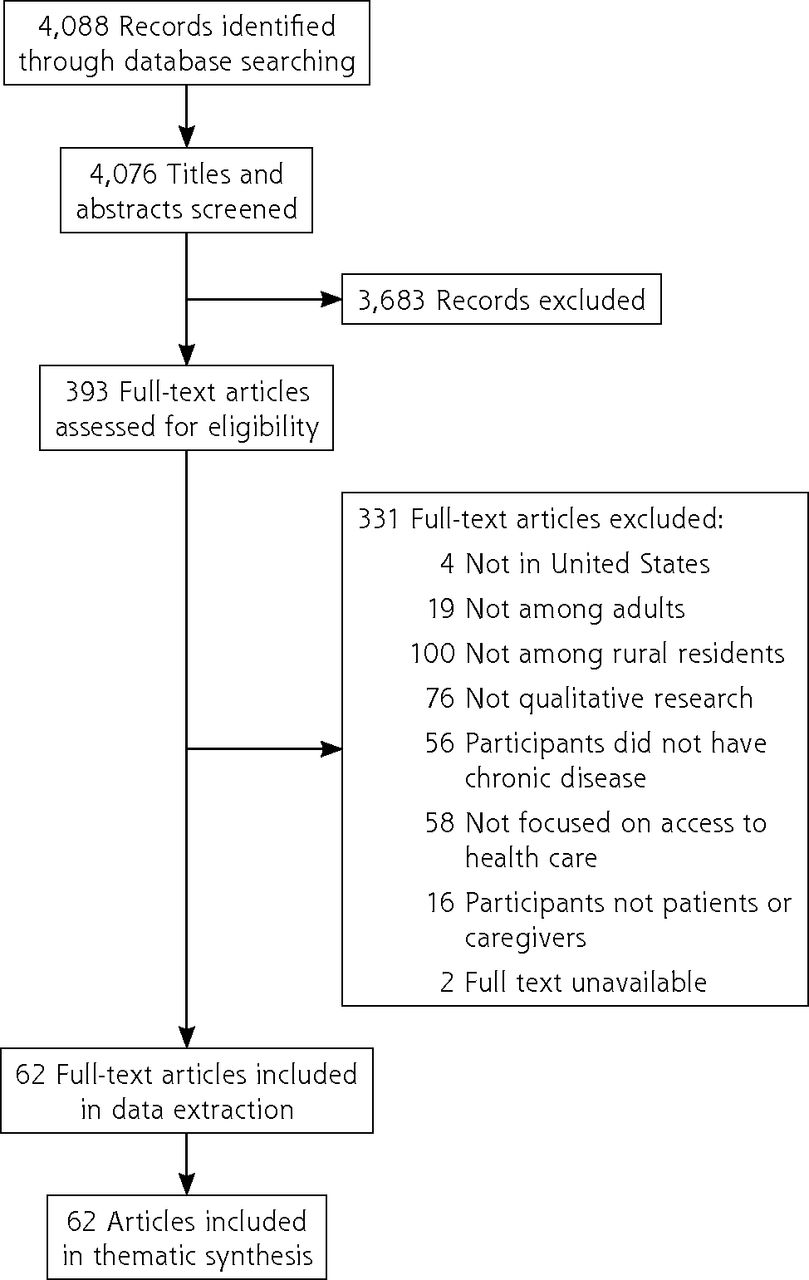
PRISMA flow diagram for study selection.
PRISMA = Preferred Reporting Items for Systematic Review and Meta-Analyses.
Table 1, Supplemental Table 2, and Supplemental Figure 1 present study characteristics. Nearly all studies (98.6%) included patients, while a sizable minority (16.1%) also or solely included caregivers. The largest share of studies (24.2%) was focused on the experience of patients with cancer, followed by behavioral health (16.1%), HIV and AIDS (14.5%), and diabetes (12.9%). The studies most commonly collected data in person (83.9%).
Overview of Study Characteristics (N = 62)
Analytic Themes
Our thematic synthesis identified 4 primary analytic themes associated with rural patient experiences of accessing health care for chronic conditions (Supplemental Table 3). We describe these themes and subthemes in detail below and give examples of relevant comments made by patients and caregivers who participated in the studies.
1. Navigating the Rural Environment
Financial and physical costs of distance. The intersection of financial issues with limitations of rural physical and built environments was noted in most studies (48 studies). In addition, the burdens associated with lengthy travel to seek routine health care services were compounded by poor health. As one participant remarked, “It’s actually 67 miles from my house to the parking lot [of my doctor’s office]. If I had to drive that sick, that’s horrible. And, depending on how sick you are, it is dangerous.”13
Social support as a facilitator of health care access. Participants in 45 studies described the critical role of spouses and other caregivers in facilitating health care transportation. At the same time, others disclosed feelings of indebtedness or guilt for continually leaning on support networks for transportation; as one participant described, “I don’t have transportation, and I have to get somebody to take me and then that’s…I mean a lot of people they have other things to do to [sic]. Sometimes you gotta’ pay them to take you, $20, $25, no matter what.”14
Willingness to go the extra mile for acceptable health care. Patients and caregivers in nearly one-half of the sample (27 studies) believed that the quality of clinicians, services, or technology in their rural community was suboptimal. Often, they chose to travel additional distances, even if health care services were available closer to home. As one participant remarked, “I do have the option to go somewhere closer to home, but I don’t want to.”15 Some medically complex patients believed that local primary care clinicians were not well equipped to manage their care. Other participants described seeking care far from their rural community to ensure confidential treatment for sensitive or stigmatized conditions. One participant described driving additional distances to ensure his privacy: “To the doctor, I have to drive an hour, hour and a half…I don’t want the local people to know about my condition [HIV] and they can access my records. If I do get a primary doctor, it will not be around me, you know. I live in a small town.”13
2. Navigating the Health Care System
Delays in obtaining care. Rural patients and caregivers in 22 of the 62 studies cited delays in needed care due to local supply-demand imbalances and limited availability of specific clinicians. In some cases, delays in obtaining treatment, medications, or services led to negative consequences for patient outcomes and health care use: “The last time when they diagnosed me with cancer, he [the local oncologist] was on vacation... and those 15 days’ time was ticking away. You know that that cancer is like this, it does not stop. The cancer spreads, spreads, spreads…. We need another doctor in this area.”16
Breakdowns in care continuity and coordination. Participants in many studies (33 studies) described barriers to maintaining a continuous relationship with a specific clinician or organization. Patients were frustrated by the inability to see a trusted or established clinician and the experience of rotating through multiple clinicians within an organization. As one participant remarked, “Every time I go up to the doctor, it’s always a different doctor, and I have to explain each time why I’m there.”17 In addition, communication between different health care professionals and organizations was frequently described as inadequate in ensuring that patients received timely, appropriate care.
Clinic structures and processes. Patients and caregivers in 29 studies described further frustration with inflexible scheduling and lengthy in-clinic wait times. Living in a rural location added considerable travel time to a clinic appointment, compounding the frustration felt when patients were then made to wait in the office: “It’s difficult because you have to plan almost a half-day off to come down here and to be able to get a parking place and to do all the stuff that you have to do to get down here. I just…I can’t fit it in my schedule.”18 Moreover, despite long waits, many patients still believed that they received inadequate time with their clinician during the encounter.
Health care system facilitators. In a smaller number of studies (13 studies), participants described efforts by their health care organization to improve access to care and coordination between clinicians, such as the use of colocated services, after-hours telephone lines, and patient navigation services.
3. Financing Chronic Disease Management
Additional costs associated with living in a rural area. A common complaint, cited in 31 studies, was the fact that living in a remote area compounded the already-high cost of health care, given the additional costs associated with transportation, overnight lodging, and time spent away from work and childcare. A participant in one study noted the indirect costs associated with health care visits: “It ain’t only the bills; it’s the getting backward and forward and stuff [and] having gas money to put in your vehicle to go. I’ve been over there sometimes on a whisper and a prayer, and when you’ve got to drive an hour and a half, 2 hours, away from your home to receive treatment, it is a strain.”19
Competing expenses. In addition to mentioning health care costs, participants in 26 studies cited competing financial priorities related to household expenses, childcare, and utilities, as well as the associated stress of making household economic trade-offs. Other participants simply accepted forgoing needed health care services because of cost.
Underlying economic circumstances. For participants in several studies (14 studies), the ongoing expense associated with obtaining care was positioned against a backdrop of larger economic hardship in rural communities. One participant described the lack of options for patients in his situation: “I work in agriculture…there’s no way, uh…anybody that works in agriculture could afford [cancer treatment], even if they do have insurance.”16 Participants described widespread poverty, a lack of employment opportunities, and a general sense of being “forgotten” by policy makers.
Health insurance–related barriers. Insurance-related limitations had a pronounced impact on certain subgroups. In particular, some Native American participants described trouble obtaining payment for necessary specialty care to treat their chronic conditions given the narrow scope of the Indian Health Service (IHS).
4. Rural Life
Close-knit communities. Participants cited many positive aspects of rural life, including high levels of social support. Others referenced the convenience of living, working, and raising families in the same community as their local health care clinicians. This sense of a tight-knit community, however, was a double-edged sword for patients and caregivers in 13 studies, as this closeness was perceived to feed gossip and create a lack of personal privacy. When “everybody knows everybody’s business,”20 patients with chronic conditions, particularly those likely to be associated with stigma or blame for personal failings, may feel uncomfortable seeking care. In fact, nearly all included studies that focused on participants with sensitive or stigmatized conditions (eg, HIV/AIDS, mental health) mentioned a desire for privacy as a barrier to use. A participant in one study described her hesitation to seek treatment at a local HIV clinic because it was located on her town’s main thoroughfare: “When I first started, I wouldn’t come to my appointments. What scared me was the location. You know, I was scared that people would see me. Who would see me come in the doors or who would see me come out the doors, that kinda made me don’t want to come in.”14
Self-sufficiency and perceived need for formal health care services. In 21 of the 62 studies, participants characterized rural culture as one that values hard work, self-sufficiency, and stoicism in the face of hardship or illness. In the context of this deep-set cultural expectation, several studies explored themes of chronic disease as a failure to live up to one’s responsibilities in the family or community. In turn, this cultural expectation influenced individual patient care-seeking attitudes and behaviors. Participants described an attitude of “powering through” chronic illness. As one shared, “Possibly they feel that it’s something that they can live with. If they’re older they’ve gotten through it—in this community especially—they may think, ‘I don’t need help, I can get through this. I’ve had this condition all my life and I’ve managed.’ We’re not talking quality of life…We’re talking about pride.”21
Many patients and their caregivers expressed reluctance to seek formal health care services for their chronic illness out of shame. A sense of stigma was especially prevalent for psychological services or treatment for substance use disorders.
Cultural sensitivity in health care settings. Participants’ desire for greater cultural sensitivity among health care professionals and clinic support staff was evident across a sizable share of studies (12 studies). Some participants cited general concerns related to feeling belittled or stereotyped by clinicians simply for being a resident of a rural area. Studies with a focus on rural Native American experiences of accessing health services noted tremendous cultural barriers to patient-centered care. Participants characterized western practitioners as paternalistic, condescending, and openly skeptical of tribal healing practices. In addition, many clinicians were viewed as inadequately versed in tribal health-related beliefs, communication preferences, and social norms. For example, in one study of Native Hawaiian and Alaska Native patients, a participant described how discordant styles of speaking and listening resulted in missed opportunities for dialog during clinical encounters: “Like, if you say a big word to one of the [Native American] elders, by the time they’re thinking of what the big word is and doctor keep talking, he’s not really listening. The doctor’s trying to figure out, because we don’t speak right away. We process before we talk.”22
DISCUSSION
Key Findings
In this comprehensive systematic review and thematic synthesis of qualitative studies, we found that rural patient experiences in accessing health care for chronic conditions mirror structural issues outlined in existing conceptual frameworks and measures of health care access.23,24 Specifically, patients across the included studies clearly recognized and described the barriers posed by limitations to the physical and built environments (ie, travel distance and time, lack of transportation options, dangerous terrain or weather), inadequate supply and quality of health care professionals and services, widespread economic hardship, and distinct rural mores that discourage the use of formal health care services and supports. Many of these barriers to health care access are well documented in the literature. Our review of qualitative experiences, however, suggests that existing administrative or population-level measures of access may overlook important nuances of the realities of managing chronic conditions in rural areas.
Participants across several included studies identified geographic proximity (commonly termed accessibility) as a desirable but not sufficient element of health care availability if the perceived quality of clinicians, technology, or facilities (often termed acceptability) was subpar. Specifically, for many patients, the experience of receiving care from available local primary care clinicians or resources was viewed as rushed, inconsistent, culturally incompatible, and, perhaps most importantly, inadequate for the task of managing their complex health needs. Notably, specialized care and technology is often unavailable in rural areas, leaving patients with fewer local resources for chronic disease management.25 For those with chronic conditions who require ongoing use of health care services, it may be worth the extra distance and travel to obtain care from clinicians who more adequately fit their medical needs, values, and preferences. In turn, this may exacerbate existing socioeconomic disparities in health outcomes between rural patients who can afford to travel elsewhere for care and those who cannot. This phenomenon and others have implications for existing access metrics of health care resource availability within a given area, which may superficially reflect adequate access but fail to incorporate more experiential dimensions that affect patient care seeking and use and, ultimately, health outcomes.
Our review found that rural cultural attitudes may represent a considerable barrier to access and use of health care services—again demonstrating that traditional metrics such as geographic proximity are not sufficient for understanding rural access. This finding supports and expands on previous work identifying rural residents as nearly twice as likely as urban counterparts to avoid seeking medical care, even when it is perceived as needed.26 The patient experiences synthesized in our review suggest that avoidance may stem from concerns about privacy and a widespread cultural emphasis on self-sufficiency. Health systems have a role in addressing these issues and beliefs through tailored interventions or communication efforts and additional training for clinicians working in these communities. In addition, the use of telehealth, which has gained popularity over the course of the COVID-19 pandemic, may also be useful in mitigating some of the privacy and self-sufficiency concerns that were discussed with some patients, especially when they are concerned about relying on others for transportation to a health care facility or being physically seen at one.
Notably, little attention was paid to telehealth or related services across the included studies, all of which took place in 2010 or more recently. Although remote technology is frequently cited as a promising mechanism for reducing physical barriers to health care access,27,28 and is specifically included as a dimension of access in the expanded conceptualization of health care access proposed by Fortney et al,24 only 3 studies included in our review explicitly focused on rural patient attitudes toward or use of telemedicine services.22,29,30 In addition, few studies included even brief discussions of the role of telemedicine or other digital health care services (eg, patient portals, mobile health [mHealth] applications and technologies) in the rural patient experience. The use of telehealth visits for outpatient care is estimated to have risen 154% during the COVID-19 pandemic,31 and this is likely a durable change.32-34 Adoption of telemedicine to access care during the pandemic, however, has been less for patients in rural compared with urban areas.35,36 Future work is needed to explore the ways in which telehealth services impact the experience of care access for rural patients with chronic health conditions, including how existing rural-urban disparities in broadband Internet access and cellular coverage influence access.37
Similarly, a minority of studies reported use of remote technologies as a mode of data collection for rural participants. Given previously documented difficulties in recruiting and retaining participants from rural areas,7,8 remote modes of participant contact represent a promising means of addressing these challenges. In addition, use of these methods may strengthen the generalizability of the evidence base by increasing the reach of research studies beyond participants already seeking clinical or community services. Future work, however, should also explore the acceptability of remote data collection methods and what impact these modes may have on participant trust and willingness to participate in qualitative research.
Strengths and Limitations
A strength of our review was our use of a systematic, comprehensive search strategy and review process to identify the greatest number of relevant studies. In addition, we used a well-established method of synthesizing data across included studies.
Limitations included variability across studies in definitions of key concepts such as rural, access, and chronic health conditions, creating the potential for an overly broad sample of included studies. We used strict, predetermined criteria, however, for study inclusion and exclusion based on accepted definitions of these concepts that were applied consistently during the review process. Finally, studies in this review reflect only qualitative research published from January 2010 through October 2019, narrowly missing the start of the COVID-19 pandemic.
Implications for Future Research and Practice
Improving access to health care in rural communities is a national imperative.25,38 Our findings may help health systems and researchers in the design and implementation of interventions that reflect underlying challenges and beliefs of rural patients struggling to effectively manage chronic health conditions. In addition, future research should explore the role of telehealth and other remote technologies in addressing the challenges described by participants in included studies, as well as the utility and acceptability of these technologies for data collection among rural participants. Finally, although the focus of this review was patients with existing chronic conditions, the importance of chronic disease prevention in rural communities should not be ignored. Many of the barriers to accessing care described by rural patients and caregivers in our review are inextricably tied to the same social determinants (eg, transportation issues, economic insecurity) that would affect prevention of chronic disease in these communities. Future research and practice efforts should explore the ways in which health prevention and promotion efforts can be synergized with interventions to enhance access to care for rural patients with existing chronic health conditions.
Footnotes
Conflicts of interest: authors report none.
Funding support: This work was supported by an internal award from the Center for Clinical and Translational Sciences (CCaTS) at Mayo Clinic.
Disclaimer: The views expressed are solely those of the authors and do not necessarily represent official views of the authors’ affiliated institutions or funder.
- Received for publication March 30, 2021.
- Revision received September 9, 2021.
- Accepted for publication September 29, 2021.
- © 2022 Annals of Family Medicine, Inc.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.