
Article Figures & Data
Figures
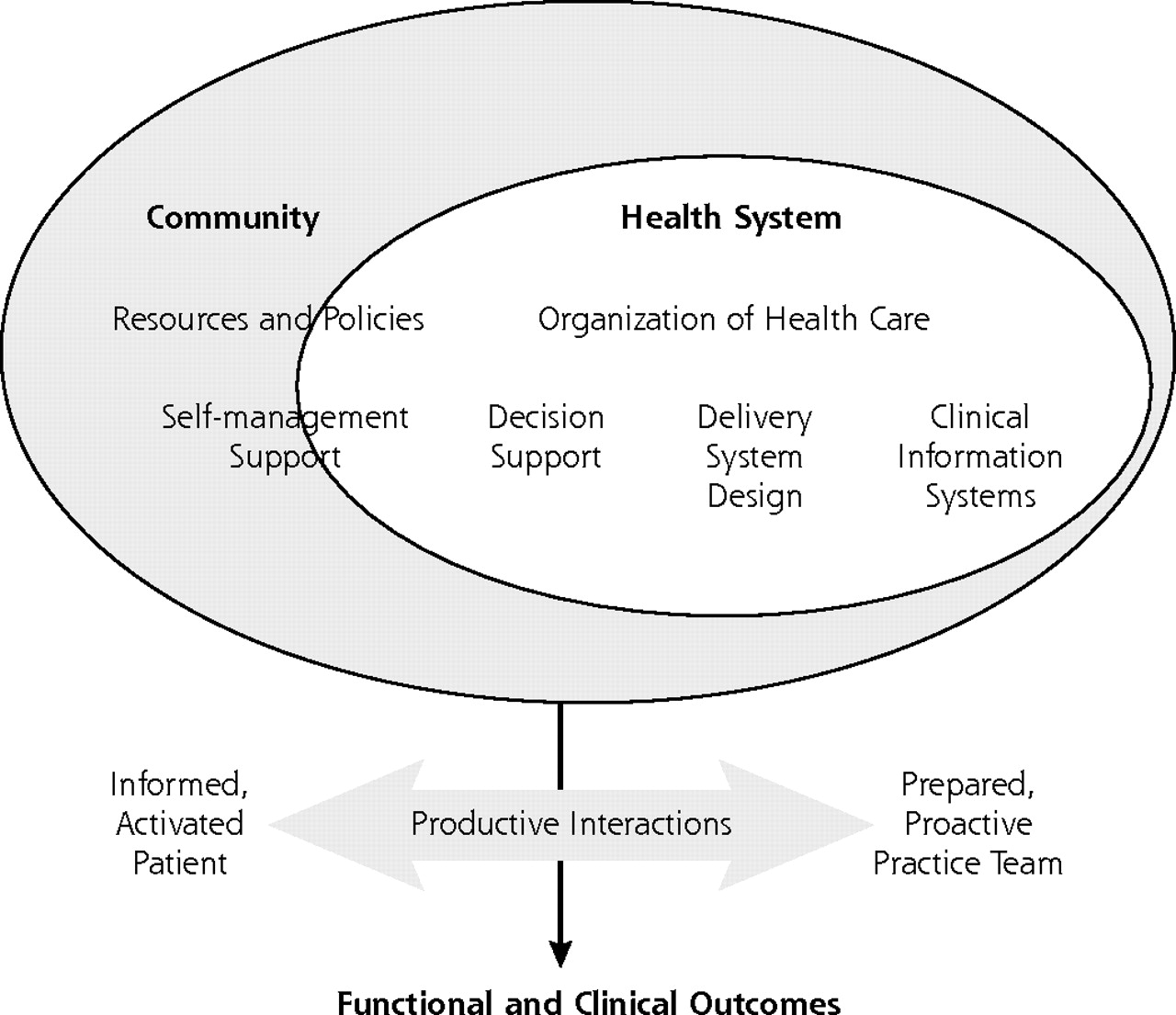
- Figure 1.
The Chronic Care Model.
Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Eff Clin Pract. 1998;1:2–4 . Reprinted with permission of the American College of Physicians. http://improvingchroniccare.org.

Tables
Clinic Characteristic 1 2 3 4 5 CCM = Chronic Care Model; PPT = prepared practice team. * Small is <7,000 members, medium is 7,000 to 16, 000, and large is >16,000. † See Methods. Clinics were asked to select diabetes, depression, or preventive services as a focus for change progress toward the CCM. ‡ Based on 2002 diabetes care improvement data collected routinely by the medical group, a combined measure of patients with both A1c and low-density lipoprotein values up to date and in control. § Rating of the change effort as made by medical group leaders. || Based on organizational data collected periodically from the clinics during the change implementation. Membership size* Medium Medium Large Medium Small Condition focus selected for improvement† Diabetes Diabetes Depression Depression Diabetes Diabetes mellitus care performance‡ No rating No rating Strong or improved Strong or improved Strong or improved Progress in initial phases of the CCM change§ Some No rating More More More Self-report of initial PPT success vs challenges|| Success > challenges Success < challenges Success = challenges Success < challenges Success = challenges Clinic CCM Element (No. of Components) Points Possible* 1 No. (%)† 2 No. (%)† 3 No. (%)† 4 No. (%)† 5 No. (%)† Mean Scores Note: Scores are reported here at the CCM element level. For scoring at the element component level, see the expanded version of Table 2 in the online-only Supplemental Table. *Presence of each component is rated as: 0 = none, 1 = some, 2 = substantial. † Percent of possible total. Delivery system redesign (6) 12 2 (17) 5 (42) 6 (50) 6 (50) 9 (75) 5.6 (47) Self-management support (6) 12 2 (17) 2 (17) 2 (17) 1 (8) 5 (42) 2.4 (20) Decision support (3) 6 0 (0) 2 (33) 3 (50) 1 (17) 3 (50) 1.8 (30) Clinical information systems (3) 6 0 (0) 1 (17) 0 (0) 2 (33) 4 (67) 1.4 (23) Community linkages (2) 4 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0.0 (0) Health care organization (3) 6 1 (17) 0 (0) 0 (0) 1 (17) 2 (33) 0.8 (13) Total 46 5 (11) 10 (22) 11 (24) 11 (24) 23 (50) 12.0 (26) - Table 3.
Comparison of the Change Process Used for Implementing Different Models From the Perspective of the Organizational Experience of Change Implementation.
Dimension Advanced Access Chronic Care Model EMR = electronic medical record; CCM = Chronic Care Model. Desired state description Clear, simple, predefined, understandable, prescriptive— many examples of what others have done Theoretical, complex, composite of pieces from various settings—no overall examples or models Change benefits Simplifies work of clinician, staff, and patient Effects on stakeholders are as unclear as the model Overall focus of the organization Concentrated on this change effort Diffused over multiple priorities Leadership role Main priority for that year with high visibility, and many dedicated resources Many simultaneous changes and priorities, the largest being EMR implementation Communication Multiple avenues with frequent and specific messages and reports from and to leadership Frequent from leadership, limited in explaining shifting strategies; few avenues for clinic team feedback to central leaders Timeline Clear endpoint in 1 year Beginning of a long process without definite endpoints External experts Experienced with many other groups, knowledgeable about specifics, and available at local collaboratives, conference calls, and an ongoing listserv (medical group also provided expertise, eg, measurement, to experts) Primarily theoretical consultants available only to leaders; no actionable blueprint of an implemented, functional CCM available Pilots Proved in 3 sites Unclear process and results in 3 to 4 sites Testimonials Videos of newly converted skeptics Individual comments at meetings Measurement A few simple, visible, repeated measures of problems and progress Difficult to develop, varied, transient, with limited connection to process changes Local change management Specified local teams with clear tasks and responsibility to tailor implementation Largely dependent on self-organizing abilities within clinics Multiclinic collaborative learning sessions Quarterly meetings of all clinics’ teams, with follow-up through listserv and conference calls Three meetings of clinic teams to learn latest change in strategy Learning session follow-up Listserv and conference calls have profound and immediate results, related to concrete, specific content of changes Listserv has limited impact, related to fuzzy content of changes Local accountability Monthly reports required and each clinic’s data and status public Periodic oral or written reports—public measures available but have limited impact Level Facilitators (Where Present) Barriers (Where Present) RN = registered nurse; PPT = prepared practice team; EMR = electronic medical record; CCM = Chronic Care Model. Clinic Strong clinic leadership Chief physicians as role models for chronic care and doing change Supervisor support of this work Development of teams Enhancement of trust and communication Promotion of stable work relationships Strong RN leadership of PPT teams and their work Physicians’ passive assent to change Previsit work by nurses and clerical staff, making life easier for physicians Staff unwilling to change leave clinic Natural changes (clinic remodeling, EMR implementation) that force changes in work relationships and flows Physician, staff, and clinic cultures not supportive of the desired changes Chief physicians relatively uninterested in or uncommitted to chronic care and the CCM Variable, often limited, leadership guidance of PPT development Few systematic change skills, strategies, or structures No standardization of PPT work flows (within and across clinics) No agreement on need for care standardization Physicians generally not engaged in the change process; change is built around them Large medical group size that filters and buffers external change motivators, eg, business competition Demands of simultaneous EMR implementation Union rules inhibit role changes Clinic staff are accountable to supervisors, not to physicians Change fatigue and apathy resulting from recent scope and pace of changes Organization leaders Clear articulation of a new conceptualization of the care cycle (previsit, visit, postvisit, between visit) Awareness of clinic attitudes and actions Clear, shared, and long-term commitment to need for change Flexible strategies for change Realistic expectations for minimal early measurable results Recognized need to change the foundation before building the house Organizational culture not supportive of the desired changes Lack of specific details and examples of desired care changes Broad scale of change required, encompassing multiple organizational facets Too many simultaneous priorities and changes Change goals and outcomes unclear Change process fuzzy and uncoordinated Lack of useful measures of change with periodic measurement Added complexities of grant funder expectations and distractions Leaders face multiple uncertainties and distractions, leading to limited change prototypes and measures, limited push, and accountability
Supplemental Table
Supplemental Table. Example of Chronic Care Model (CCM)Implementation Scoring
Files in this Data Supplement:
- Supplemental data: Table - PDF file, 1 page, 78 KB
The Article in Brief
Challenges of Change: Implementing the Chronic Care Model
Mary C. Hroscikoski, MD , and colleagues
Background Improving health care for people with chronic medical conditions is a major concern in the U.S. The Chronic Care Model (description below) suggests that care of the chronically ill should include prepared teams in the medical practice interacting with informed, involved patients. Although the Chronic Care Model (CCM) provides a well-developed framework for improving chronic medical care, there are no specific steps available to guide medical groups wanting to implement it. The purpose of this study is to examine and learn from the experience of a large medical group that implemented the CCM.
(Description: From: http://www.improvingchroniccare.org/change/model/components.html: �The Chronic Care Model identifies the essential elements of a health care system that encourage high-quality chronic disease care. These elements are the community, the health system, self-management support, delivery system design, decision support and clinical information systems. Evidence-based change concepts under each element, in combination, foster productive interactions between informed patients who take an active part in their care and providers with resources and expertise. The model can be applied to a variety of chronic illnesses, health care settings and target populations. The bottom line is healthier patients, more satisfied providers, and cost savings.�)What This Study Found This medical group�s effort to transform its approach to care by implementing the CCM concepts appears to have produced some changes, in particular partial changes in the structure, roles, and function of medical teams and the introduction of an electronic medical record. Medical practices implementing the CCM should select care processes that have been well worked out in similar settings, or before tackling implementation, they should devote time to careful design and pilot testing. The CCM may be best suited as a backdrop for understanding the relationships and roles of specific care changes that are needed, rather than as a blueprint or training model for change.
Implications
- The team changes in this study were small and varied, but they may represent a first step in creating a new foundation for transformed care.
- Changing traditional care patterns is very difficult, requiring enormous attention and focus with clear specifications, strong leadership, and attention to many details at both local and central levels of an organization.
Annals Journal Club Selections:
Jul/Aug 2006
The Annals Journal Club is designed to encourage a learning community of those seeking to improve health care and health through enhanced primary care. Additional information is available on the Journal Club home page.Articles for Discussion
- Solberg LI, Crain AL, Sperl-Hillen JM, Hroscikoski MC, Engebretson KI, O�Connor PJ. Care quality and implementation of the Chronic Care Model: a quantitative study. Ann Fam Med. 2006;4:310-316.
- Hroscikoski MC, Solberg LI, Sperl-Hillen JM, Harper PG, McGrail M, Crabtree BF. The challenges of change: implementing the Chronic Care Model. Ann Fam Med. 2006;4:317-326.
Discussion Tips
This issue of Annals features multimethod research that integrates both quantitative and qualitative methods. These methods have complementary strengths and weaknesses, and their conjoint use often can provide a fuller picture than studies using either type of method alone.1 The intervention being evaluated in the articles for this journal club is based on the Chronic Care Model.2 This theoretical framework is being widely used to develop infrastructure to promote informed, activated patients interacting with a prepared, proactive practice team to improve patients� functional and clinical outcomes.Discussion Questions
- What is the Chronic Care Model, and why might it matter (http://improvingchroniccare .org/change/model/components.html)?
- Was the design of each study appropriate to its research question?
- What designs and measures would be stronger?
- What characteristics of the study practices and health care system are different from your practice in ways that affect the transportability of the findings?
- To what degree can the findings be accounted for by:
- Inadequate sample size?
- Selection bias in who was included in the study?
- Poorly measured or irrelevant constructs?
- Poor implementation of the model?
- High baseline performance in the participating practices?
- Changes not attributable to the intervention?
- What are the strengths and weaknesses of the quantitative study (Solberg et al)? What are the strengths and weaknesses of the qualitative study (Hroscikoski et al)? How do the strengths of one bolster the weaknesses of the other?
- What are some relative weakness in your practice�s ability to provide good chronic care (see the elements of the Chronic Care Model in Solberg or Figure 1 in Hroscikoski)? What office systems or other process changes would improve chronic care? Which changes would have the greatest impact on quality of chronic care? Which changes would be easy to implement?
- Given the lessons learned by the authors, what would be your strategy for making change in your practice?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4:196-197. Available at: http://annfammed.org/cgi/content/full/4/3/ 196.
- Wagner EH, Glasgow RE, Davis C, et al. Quality improvement in chronic illness care: a collaborative approach. Jt Comm J Qual Improv. 2001;27:63-80.




{kind=link}
Jump to section
Related Articles
Cited By...
- A framework for chronic care quality: results of a scoping review and Delphi survey
- Quality of care for chronic conditions: Identifying specificities of quality aims based on scoping review and Delphi survey
- Improving Quality Improvement Capacity and Clinical Performance in Small Primary Care Practices
- A Randomized Trial of External Practice Support to Improve Cardiovascular Risk Factors in Primary Care
- UK guideline on transition of adolescent and young persons with chronic digestive diseases from paediatric to adult care
- Strategies for Achieving Whole-Practice Engagement and Buy-in to the Patient-Centered Medical Home
- Support and Strategies for Change Among Small Patient-Centered Medical Home Practices
- How Eight Primary Care Practices Initiated and Maintained Quality Monitoring and Reporting
- Impact of EHR-Based Clinical Decision Support on Adherence to Guidelines for Patients on NSAIDs: A Randomized Controlled Trial
- Features of the Chronic Care Model (CCM) Associated with Behavioral Counseling and Diabetes Care in Community Primary Care
- Guidelines in the United Kingdom and How They Are Used
- The Patient-Centered Medical Home For Chronic Illness: Is It Ready For Prime Time?
- It takes a village to prevent falls: reconceptualizing fall prevention and management for older adults
- Beyond Fighting Fires and Chasing Tails? Chronic Illness Care Plans in Ontario, Canada
- The Missing Link: Improving Quality With a Chronic Disease Management Intervention for the Primary Care Office
- Improving Medical Practice: A Conceptual Framework
- Different Paths to High-Quality Care: Three Archetypes of Top-Performing Practice Sites
- On TRACK: 'Allows Readers and Authors to Go One Step Further'
- In this Issue: Mixed Methods and Diverse Perspectives
- Care Quality and Implementation of the Chronic Care Model: A Quantitative Study
- Annals Journal Club: Implementing the Chronic Care Model
- Publishing Multimethod Research