


Abstract
PURPOSE The patient-physician relationship is the cornerstone of health care service delivery. The objectives of this study were to assess the contribution of relationship commitment along with trust to patient-physician relationships and to evaluate the association of commitment and trust with adherence to medical advice and healthy eating behaviors.
METHODS To test the proposed model, we developed a questionnaire that included both existing scales and a scale constructed specifically for the study; the questions addressed trust, commitment, adherence to physicians’ medical recommendations, and healthy eating behavior. The questionnaire was given to adult patients in the waiting rooms of 4 large clinics in central Texas.
RESULTS A total of 1,008 patients returned questionnaires; 869 patients’ questionnaires were complete and used in the analysis. A 3-stage least squares analysis that tested a system of 4 equations which included relationship commitment yielded a systemwide R2 of 0.71 that was 0.09 higher than a system of equations excluding relationship commitment. Trust and commitment were positively associated with adherence (P <.001 and P = .02, respectively). We also found positive relationships between adherence and commitment and between trust and commitment (P <.001 for each). Adherence and commitment were both associated with healthy eating behavior as well (P <.001 for each).
CONCLUSIONS Patients’ trust in their physician and commitment to the relationship offer a more complete understanding of the patient-physician relationship. In addition, trust and commitment favorably influence patients’ health behaviors.
- Physician-patient relations
- relationship commitment
- trust
- physician behavior
- patient adherence
- patient compliance
- healthy eating behavior
- primary care
INTRODUCTION
The intimacy, importance, complexity, and variability of medical services cause many patients to desire continuity with 1 physician as a primary source of care. Safran1 has summarized a series of studies in the United States starting in the 1970s indicating that most adults have a physician they consider to be their primary physician. The percentages reported range from 88% in 1975 to 77% in 1996.2–5 In 2005, 76% of 35,383 patients studied reported that they saw the same clinician always or most of the time.6 This figure is similar to the 68.3% of 16,435 patients that a group of primary care physicians identified from their patient panel as being their patients.7 A study of family practice patients in the United States and United Kingdom found that 79% of patients rated seeing the same physician for a health problem as important or very important.8 Fan et al6 found that those patients who reported seeing the same physician always or most of the time had patient satisfaction scores that were significantly higher than those of their counterparts who did not see the same physician. Clearly, most patients value continuity of care. Learning more about the patient-physician relationship motivated our study. We wanted to investigate whether strength of the patient-physician relationship was associated with positive patient attitudes and behaviors (ie, adherence to medical recommendations and healthy eating).
In general, patients remain in relationships with clinicians either by choice or because they perceive no alternative. The former can be termed dedication-based relationships; the latter, constraint-based relationships.9 For various reasons, including insurance plan design, unavailability of substitute clinicians, or patient passivity, patients may remain with physicians even when they do not want to; however, one should expect the patient-physician relationship to differ qualitatively based on why the patient maintains it. Accordingly, in this study, we distinguish between duration of care and patient commitment to the relationship. Relationship commitment is the degree to which a relationship is valued; with commitment, the patient wants the relationship to continue and invests energy toward its continuance.
Trust is considered a key component of relationships between patients and physicians.10–12 Trust exists when patients perceive their physician to be sincere, credible, honest, and benevolent.13,14 Trust can lead to important outcomes. For example, patients’ trust in their physician has been shown to predict patient satisfaction8 and adherence to a medical regimen.15 A study of hypertensive patients’ adherence to medication recommendations found that patients with the lowest levels of adherence do not trust their physicians.16 Yet, other research suggests that, depending on the method of analysis, there may be no “physician effect” (which includes trust) on patient outcomes.17
We explored the patient-physician relationship by including relationship commitment in our evaluation and specifically measuring its effects. We believe that trust strengthens relationship commitment, and measuring both constructs together could improve our understanding of patient-physician relationships. Morgan and Hunt18 hold that both trust and commitment are key to all commercial relationships. Such a conclusion should be no less true for the delivery of primary care health services. We therefore designed our study to explore the association of trust and relationship commitment with 2 desirable patient outcomes: medical adherence and healthy eating. We also wanted to learn more about the antecedents of strong patient-physician relationships, specifically, the antecedents of trust.
Primary care physicians play a key role in encouraging adherence to prescribed medical regimens and healthy lifestyles.15,19–23 Adherence is a salient issue. A meta-analysis of 63 studies assessing patient adherence and medical treatment outcomes concluded that, on average, 26% more patients had a good outcome through adherence vs nonadherence.24 Yet, research shows that patient adherence in taking prescribed medications is suboptimal, with little relation to social and demographic characteristics.23–27 A systematic review of published randomized controlled trials of interventions to increase patients’ adherence to prescribed medications showed that even the most effective interventions did not lead to large improvements in adherence and treatment outcomes.28 We conceptualize adherence as an attitude toward following physician suggestions; therefore, in our model, adherence is a mediator between trust and healthy eating behaviors.
We selected healthy eating behaviors for study because of the alarming rise of obesity in America and obesity’s role as a well-known risk factor for multiple diseases, including hypertension, type 2 diabetes, osteoarthritis, cardiovascular disease, stroke, certain types of cancer, and dementia.29–33 Any association between strength of the patient-physician relationship and patients’ healthy eating behavior would merit further attention and research.
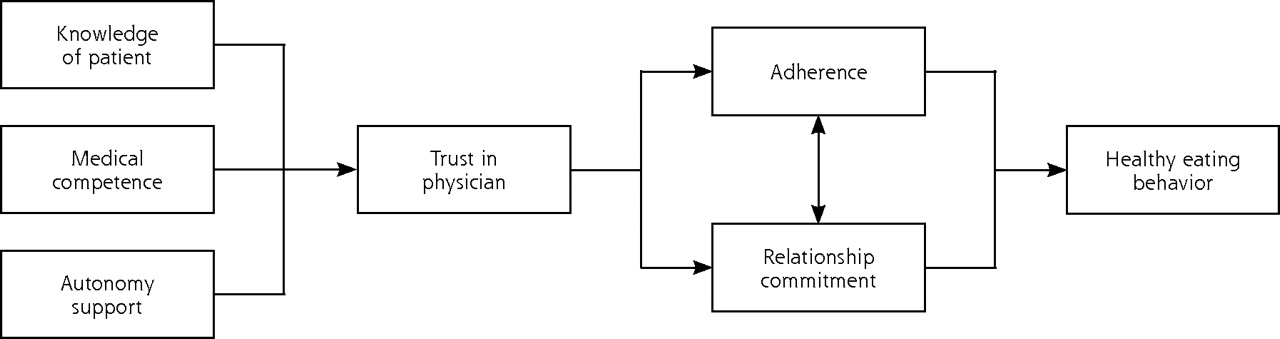
The model that we tested (Figure 1⇓) posits that patients’ trust of their physician is associated with 3 composite physician behaviors: developing knowledge of the patient, demonstrating medical competence, and supporting patient autonomy.17,34,35 Knowledge of the patient refers to patients’ perceptions that their physician knows their medical history and knows them as a person. Competence is defined as the degree to which patients perceive that physicians have the skills and knowledge required to provide for their health care needs.36 Patient autonomy refers to patients’ perceptions that their physician encourages questions and listens to their requests.37 We postulated that patients’ commitment to their relationship with their physician is linked to their trust perceptions. We also posited that both trust and commitment influence adherence to medical recommendations. We further hypothesized that commitment and adherence are associated and both contribute to healthy eating behaviors. Patients’ trust in and commitment to their primary physician are thus instrumental in improving adherence and diet.
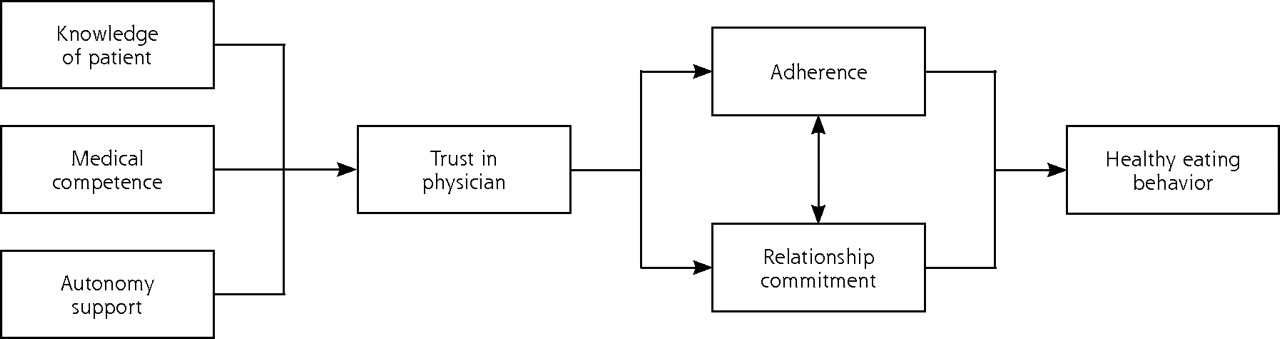
Conceptual diagram of proposed model relationships.
METHODS
Questionnaire
To test the proposed model, we developed a questionnaire that included existing scales that were adapted for this study and a new scale for competence. The scales, as well as their sources, means, reliabilities, and items are displayed in Table 1⇓. We measured attitudinal commitment (eg, “The relationship … is important to me”). We pretested and refined our questionnaire in several phases. First, we convened a group of 10 adults to complete the questionnaire and then provide feedback on instructions or questions that were problematic. We then mailed a revised questionnaire with a cover letter on a test basis to a random sample of 750 adults living in a 5-county area in the central United States. We received 93 completed questionnaires and further revised the questionnaire based on the results of exploratory factor analysis and reliability analysis.
Measures, Sources, Means, Reliabilities (α), and Items
Study Setting, Data Collection, and Respondents
The final self-administered questionnaire and cover letter were distributed and collected by a group of trained research assistants in family practice patient waiting rooms in 4 clinics in central Texas. Waiting room samples are often used in studies of this type, as they provide access to the appropriate population.40–42 The clinics are staffed by family physicians employed by a large multispecialty group practice that is academically affiliated with a university and a medical school. These are continuity clinics that provide routine chronic care and wellness care. Approximately 50% of the appointments are for same-day acute medical problems. The 4 clinics were chosen because they serve a demographically diverse patient population and are relatively large, providing care to between 2,400 and 8,200 patients per month with 6 to 20 primary care physicians per clinic. In November 2005 data were collected for 8 full days at each of the clinics covering each weekday. No data were collected during night or weekend hours. All adult patients entering the waiting room were approached.
Statistical Analysis
Using the SAS statistical analysis software (SAS v9.1, SAS Institute, Cary, North Carolina), we selected a system of 4 equations to study the proposed relationships among the variables of interest (Figure 2⇓). In this system, the variables adherence, commitment, and trust that appear as regressors in equations (1), (2), and (3) also appear as dependent variables in equations (2), (3), and (4), respectively. It is well established that estimating the above system of equations by ordinary least squares (OLS) analysis will yield inconsistent estimates43; furthermore, the errors across equations (1) through (4) may be correlated. As a result, consistent with literature in economics and marketing,44,45 we used a 3-stage least squares (3SLS) procedure that accounts for the correlation across the error terms and thus yields consistent estimates. We conducted this analysis both with and without the relationship commitment variable. Finally, while analyzing the effect of the relationship variables on healthy eating behavior, we accounted for other control variables, such as the presence of a chronic illness and patient demographics (Figure 2⇓).

System of 4 equations used to assess relationships among the variables of interest.
RESULTS
Respondents
Approximately 75% of patients approached agreed to participate in the study. Questionnaires were collected from 1,008 patients; 869 patients’ questionnaires were deemed complete and usable for the analysis. The majority of our respondents were female (66%), college educated (72% had at least some college), and white (81%), and had incomes between $25,000 and $75,000 (74%). The average age of the respondents was 50 years.
Patient-Physician Relationship
Table 2⇓ displays the results of the 3SLS estimation for the system of equations (1) through (4). The proposed system of equations fits the data well, with the systemwide R2 for the proposed set of equations equal to 0.71. When we repeated the 3SLS without the relationship commitment variable, the systemwide R2 decreased to 0.62, empirically demonstrating the value of relationship commitment in understanding the patient-physician relationship.
Estimates Derived With the System of Equations
Influence of Trust and Commitment
Specific results from our proposed model showed that all of the significant coefficients had the expected signs (Table 2⇑). As expected, knowledge of the patient, competence, and autonomy support were significantly related to patient trust (P <.001 for all 3 variables). Both trust (P <.001) and commitment (P = .02) were positively associated with adherence. The results also supported the hypotheses of positive relationships between adherence and commitment (P <.001) and between trust and commitment (P <.001). In other words, the greater patients’ levels of adherence and trust, the greater their level of commitment to the physician. Additionally, the results supported our model by indicating that adherence (P <.001) and commitment (P <.001) are associated with healthy eating behavior.
Influence of Control Variables
With respect to the control variables, patients who were older (P <.001), had higher incomes (P = .047), and were more educated (P = .01) had healthier eating patterns (Table 2⇑). All other factors remaining the same, female patients had healthier eating behavior than their male counterparts (P = .001). Higher education and income as well as female sex have been linked to healthier eating in previous research, with education being the most influential factor.46 We also controlled for chronic illness and found that it had no significant effect on eating behavior.
DISCUSSION
Most patients want a strong relationship with a primary doctor.1,21,47,48 The vulnerability and dependency inherent in being ill and at a knowledge disadvantage, the necessity of revealing personal information, and the sheer importance of the service make finding—and keeping—a “good doctor” a consumer priority. Literature converges on patients’ valuing relationships with physicians who evoke trust and convey respect. Physicians evoke patients’ trust and convey respect by listening carefully to their patients, developing whole-person knowledge about them, explaining issues clearly and forthrightly, treating patients as partners in their own care, showing compassion, and being thorough.1,8,12,15,47,49–56
We designed our study to specifically include relationship commitment because its measurement should yield a richer understanding of the patient-physician relationship. Although trust is an essential component of relationship commitment, it is not its equivalent. Patients may trust their physicians but not necessarily feel strongly about continuing their relationship with them. Our measure of relationship commitment assesses the degree to which patients value the relationship and want it to continue.
Results for our sample show a significant association between the patient-physician relationship and patients’ adherence to their physician’s medical recommendations and healthy eating behavior. Strength of the relationship matters. Patients’ trust in the physician and commitment to the relationship offer a more complete understanding of the relationship. The patient-physician relationship is built not only from physicians’ medical competence, but also from their interpersonal behavioral competence. If a “good doctor” is one who positively influences health-related behaviors, then our findings support the conclusion that good doctors are both interpersonally proficient and technically proficient, not just the latter. They know their patients and work with them in a spirit of partnership (conceptualized as autonomy in this study). Both knowledge of patients and support of their autonomy are consistent with conveying respect.
In a joint presentation at the 2006 Institute of Healthcare Improvement National Quality Forum, primary care physicians Douglas Eby, MD, and Charles Kilo, MD, argued that the real work of advancing health is physicians affecting the choices made by individuals with regard to eating, drinking, smoking, exercising, managing stress, parenting, taking prescribed medications, and other behaviors. Their position is supported by data-based estimates on the relative impact of 5 domains on US deaths: genetics, social circumstances, environmental conditions, behavioral choices, and medical care.57 While recognizing the interconnectedness of the categories, the researchers concluded that approximately 40% of deaths are caused by modifiable behavior patterns, such as poor diet, physical inactivity, substance abuse, and poor coping strategies for stress.
What is most intriguing about our findings is the influence that primary care physicians with strong patient relationships appear to have on their patients’ behavior. Other research also suggests the positive influence that good physicians can have on patients’ health-related behaviors. In another study, primary care visits characterized by higher levels of physician-patient concordance (as reported by physicians) were associated with one-third higher medication compliance.58 The Diabetes Prevention Program, a randomized controlled trial, found intensive lifestyle modification to be more effective than metformin for reducing the incidence of type 2 diabetes.59 Patient adherence to lifestyle recommendations (including healthy eating) was a central feature for successful interventions, and adherence was optimized when physicians developed a coaching approach to encourage patients to make positive choices and develop self-sufficiency and assist them in identifying and overcoming barriers.60 These interventions are most effective when physicians are part of a larger team of allied health professionals.
The conceptualization and measurement of relationship commitment in the present study may help explain the nature of physicians’ influence on their patients’ behavior. Strong relationships require that both parties desire to maintain them. Relationships inevitably suffer and frequently end when one party does not reciprocate the investment of the other. One possible interpretation of our findings is of patients investing in the quality of a valued relationship with their physician through positive, healthy behavior.
To invest in stronger patient relationships while managing the pressures of time, physicians need to consider and develop new approaches to educate patients. Needed are methods or processes that make counseling and education more available to patients and more practical for physicians to provide from both time and financial standpoints. For example, physicians could schedule group educational appointments, create physician and nonphysician teams, and seek more progressive health insurance plans that reimburse preventive and education services.61,62
We can draw conclusions from this study about our sample—but not about a broader group of patients because of sampling limitations. Our data come from patients in 4 clinics of a single regional health care organization. A larger, geographically dispersed sample could reveal important regional differences. Our respondents were largely white and relatively well educated; a more demographically diverse sample could reveal salient differences, as could a sample of patients less established with primary care physicians. Also, we studied patients’ relationship with their primary care physicians and cannot claim that our findings apply to other types of physicians; moreover, patients’ relationships with clinicians other than their primary care physicians may have played a role in the outcomes we report. Waiting room samples offer the advantages of access to respondents and good participation rates, but have the disadvantage of favoring patients who make frequent appointments. Only patients visiting the clinics during the 8-day data collection period had an opportunity to participate in the study.
Our study’s design creates the possibility of self-report bias. In particular, the adherence and healthy eating behavior constructs may be subject to socially desirable responses, leading participants to underestimate or overestimate their responses. Even so, literature suggests that self-reported measures are useful for developing hypotheses and in initial investigations.63,64 Some studies suggest that the response bias that occurs from self-reported measures is not a grave concern when this bias does not vary systematically.65,66 Given the focus of this research, we do not believe that any self-reporting bias that exists will affect the substantive findings or vary systematically, but we recognize it as a potential threat to validity. The addition of objective measures, however, especially of the adherence and healthy eating behavior constructs, could help solidify the validity of findings. A social desirability bias scale could also be incorporated in future research. As an example, the Crowne-Marlowe Scale67 helps researchers establish discriminant validity by comparing inter-correlations between the social desirability scale and other scales of interest.68
Additional research is needed to both replicate and extend our findings. Future study could include other patient behaviors, the application of the model to different types of physicians, and possible changes among associations of model variables over time. Also, our study focuses on the patient-physician relationship from the patient’s perspective. Research that simultaneously assesses patient and physician commitment to the relationship could be useful.
The patient-physician relationship is central to the delivery of high-quality health care. Relationship commitment is a construct that merits further research. Continued research on what contributes to and detracts from strong patient-physician relationships should help clinicians craft improved practice strategies and lead to healthier patients.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This work was supported by Scott & White, Texas A&M University.
- Received for publication January 26, 2007.
- Revision received July 13, 2007.
- Accepted for publication July 31, 2007.
- © 2008 Annals of Family Medicine, Inc.
REFERENCES





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploring the psychometric properties of the Working Alliance Inventory in general practice: a cross-sectional study
- Discrimination and Medical Mistrust in a Racially and Ethnically Diverse Sample of California Adults
- Continuity of care as a predictor of ongoing frequent attendance in primary care: a retrospective cohort study
- Patient Commitment and Its Relationship to A1C
- Patients perceptions of access to primary care: Analysis of the QUALICOPC Patient Experiences Survey
- Association between interpersonal continuity of care and medication adherence in type 2 diabetes: an observational cohort study
- Provider Practice Characteristics That Promote Interpersonal Continuity
- Look Who's (Not) Talking: Diabetic patients' willingness to discuss self-care with physicians
- Implications of Reassigning Patients for the Medical Home: A Case Study
- The Medical Home: Growing Evidence to Support a New Approach to Primary Care
- Journey to the Future of Family Medicine
- In This Issue: Mental Health and Care Management, Health Behavior Change, and Reflection in Primary Care