


Abstract
PURPOSE We wanted to assess the impact of an electronic health record–based diabetes clinical decision support system on control of hemoglobin A1c (glycated hemoglobin), blood pressure, and low-density lipoprotein (LDL) cholesterol levels in adults with diabetes.
METHODS We conducted a clinic-randomized trial conducted from October 2006 to May 2007 in Minnesota. Included were 11 clinics with 41 consenting primary care physicians and the physicians’ 2,556 patients with diabetes. Patients were randomized either to receive or not to receive an electronic health record (EHR)–based clinical decision support system designed to improve care for those patients whose hemoglobin A1c, blood pressure, or LDL cholesterol levels were higher than goal at any office visit. Analysis used general and generalized linear mixed models with repeated time measurements to accommodate the nested data structure.
RESULTS The intervention group physicians used the EHR-based decision support system at 62.6% of all office visits made by adults with diabetes. The intervention group diabetes patients had significantly better hemoglobin A1c (intervention effect −0.26%; 95% confidence interval, −0.06% to −0.47%; P=.01), and better maintenance of systolic blood pressure control (80.2% vs 75.1%, P=.03) and borderline better maintenance of diastolic blood pressure control (85.6% vs 81.7%, P =.07), but not improved low-density lipoprotein cholesterol levels (P = .62) than patients of physicians randomized to the control arm of the study. Among intervention group physicians, 94% were satisfied or very satisfied with the intervention, and moderate use of the support system persisted for more than 1 year after feedback and incentives to encourage its use were discontinued.
CONCLUSIONS EHR-based diabetes clinical decision support significantly improved glucose control and some aspects of blood pressure control in adults with type 2 diabetes.
- Electronic health records
- diabetes mellitus
- quality of health care
- quality improvement
- glucose control
- blood pressure control
- primary health care
- randomized trial
INTRODUCTION
Despite recent improvement trends in the United States, in 2008 less than 20% of patients with diabetes concurrently reach evidence-based goals for hemoglobin A1c (glycated hemoglobin), systolic and diastolic blood pressure, and low-density lipoprotein (LDL) cholesterol levels.1,2 Care is unsatisfactory in both subspecialty and primary care settings, but because more than 80% of diabetes care is delivered by primary care physicians, effective strategies to improve diabetes care in primary care settings are urgently needed.
Among the major barriers to better diabetes care is lack of timely intensification of pharmacotherapy in patients who have not achieved recommended clinical goals. Many factors contribute to this problem, including competing demands at the time of the visit3 and medication nonadherence.4 Rates of treatment intensification when patients are not at goal, however, hover around 70% to 80%,5 and several studies have linked higher rates of treatment intensification by a primary care physician to better rates of hypertension, lipid, or glucose control in that primary care physician’s patients.6
In theory, treatment intensification and control of hemoglobin A1c, blood pressure, and lipid levels in patients with diabetes mellitus could be improved by providing patient-specific and drug-specific clinical decision support at the time of a clinical encounter. Electronic health records (EHRs) can be programmed to include sophisticated clinical algorithms that take advantage of current and past clinical information to provide detailed clinical recommendations at the time of a clinical encounter.7–9 Prior efforts have typically improved processes of care (such as rate of hemoglobin A1c or LDL cholesterol testing or eye examinations) but failed to improve key intermediate outcomes of care, such as control of hemoglobin A1c, blood pressure, or LDL cholesterol levels.10–16 It is especially important to improve hemoglobin A1c, blood pressure, and LDL cholesterol levels, because appropriate control of these risk factors can substantially influence the rate of major microvascular or macrovascular complications of diabetes.17–21
Beyond diabetes care, many studies document the failure of EHR-based clinical decision support to improve key intermediate clinical outcomes in patients with hypertension, congestive heart failure care, asthma, and other conditions.22–25 A careful reading of these failed studies, including several of our own, identified several possible reasons why EHR-based clinical decision support failed to improve intermediate outcomes of chronic disease care. First, most clinical decision support was limited to general prompts and reminders and did not include more detailed drug-specific advice. Second, introduction of EHR-based clinical decision support was usually not accompanied by changes in staff responsibilities and clinic workflow to enhance the impact of the clinical decision support on care. Third, rather than being used for visit planning, clinical decision support displays were usually provided late in the encounter and were often skipped over or not viewed by physicians. Finally, physicians typically received no tangible compensation or reward for the extra time and effort needed to adopt new and unfamiliar clinical routines.
Based on these observations, we developed, pilot tested, and refined a novel patient-customized EHR-based clinical decision support system for type 2 diabetes care designed to overcome obstacles to use observed in earlier studies. Here we report a clinic-randomized trial that assessed the impact of this EHR-based clinical decision support system on intermediate outcomes of diabetes care, including hemoglobin A1c, blood pressure, and LDL cholesterol control.
METHODS
The study was reviewed in advance, approved, and monitored on an ongoing basis by the HealthPartners Institutional Review Board, project #03-083, and by an independent data safety and monitoring board.
Design Overview
This group-randomized trial tested the hypothesis that an EHR-based clinical decision support system would improve hemoglobin A1c, blood pressure, and lipid control in adults with type 2 diabetes receiving care from primary care physicians.
Setting and Participants
The study was conducted at HealthPartners Medical Group (HPMG), a large medical group in Minnesota that provided care to approximately 9,000 adults with diabetes in 2007. Most diabetes care was provided by primary care physicians; 10% of type 2 patients each year see an endocrinologist, most for 1 visit.
Primary care physicians were eligible for the study if they practiced in a study clinic, provided care to at least 10 adults with type 2 diabetes, and provided written informed consent to participate. Patients were classified as having diabetes if they had 2 or more out-patient diabetes International Classification of Diseases, Ninth Revision (ICD-9) codes (250.xx) or used 1 or more diabetes-specific medications in the 1-year period before randomization.26 This diabetes identification method has estimated sensitivity of 0.91 and positive predictive value of 0.94.26
Randomization and Interventions
Eleven HPMG clinics that used EHRs for 2 or more years were included in this study. Pairs of clinics having a similar proportion of patients at a composite diabetes care goal were placed into strata. Within each stratum a clinic was randomly assigned to either the intervention or control arm.
The EHR-based diabetes clinical decision support system (referred to as Diabetes Wizard) was provided to physicians at the 6 intervention clinics. Nursing staff and physicians participated in a 1-hour training session during which they were instructed that the Diabetes Wizard was not meant to override or supersede clinical judgment, and that its use was limited to type 2 diabetes patients aged 18 to 75 years. Adults aged 75 years and older and those with a Charlson comorbidity scores of 3 or more (indicating high short-term risk of mortality) were excluded from the study because of legitimate debate about appropriate clinical goals in such patients.27–29
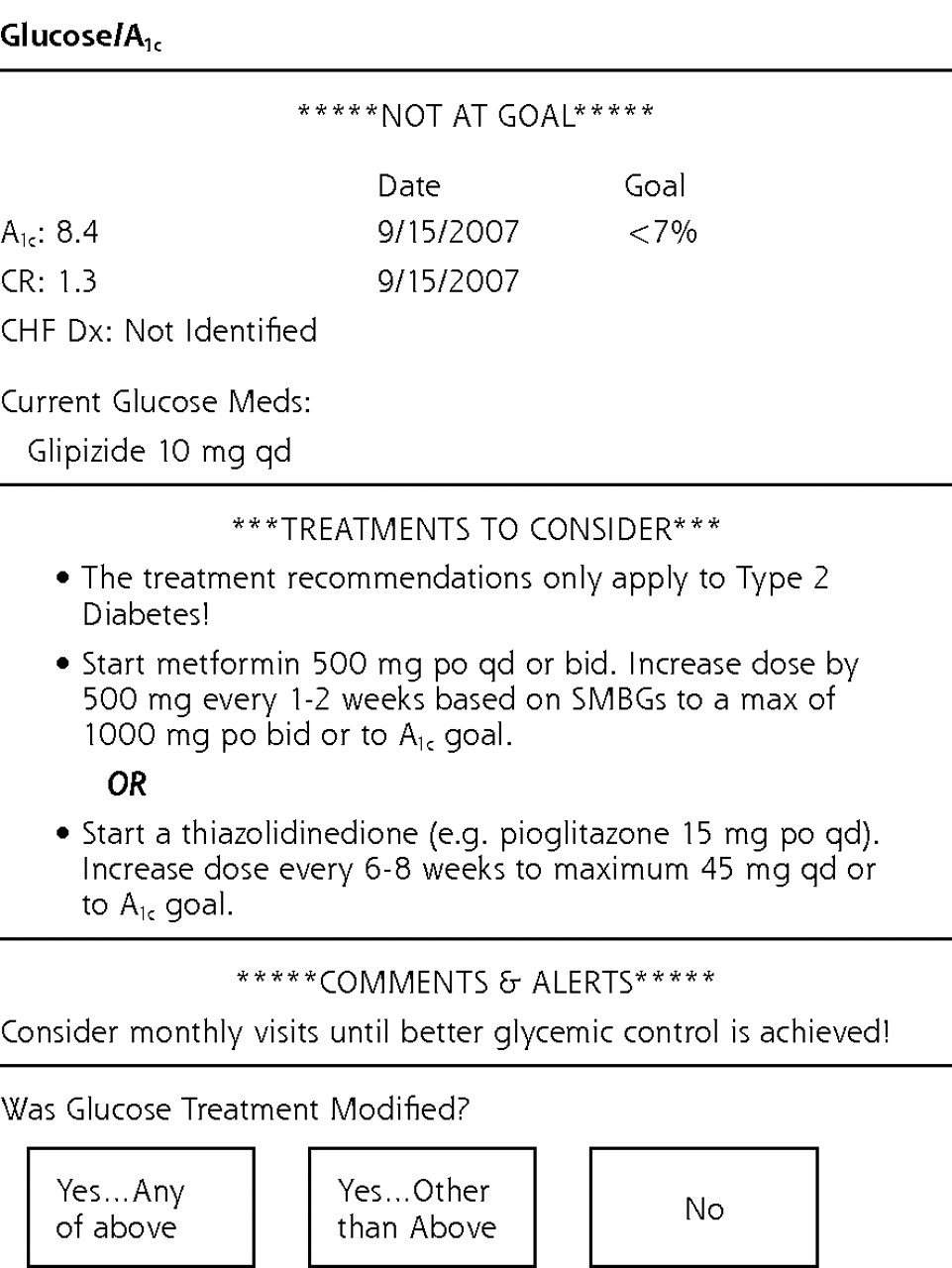
Diabetes Wizard implementation included the following changes in clinic workflow at intervention clinics. (1) The rooming nurse enters blood pressure readings into EHR as usual. (2) If the patient has diabetes, the rooming nurse opens the Diabetes Wizard in the EHR with a single click on the navigation bar, prints the EHR-generated Diabetes Wizard form (Figure 1⇓), and closes the form in the EHR. (3) The rooming nurse places the printed form on top of the visit summary sheet on the examination room door. (4) The physician reviews the available diabetes treatment options printed on the form just before entering the room and proceeds with the visit. (5) After the visit but before closing the encounter, the physician opens the Diabetes Wizard form in the EHR visit navigator and completes the brief visit resolution form.
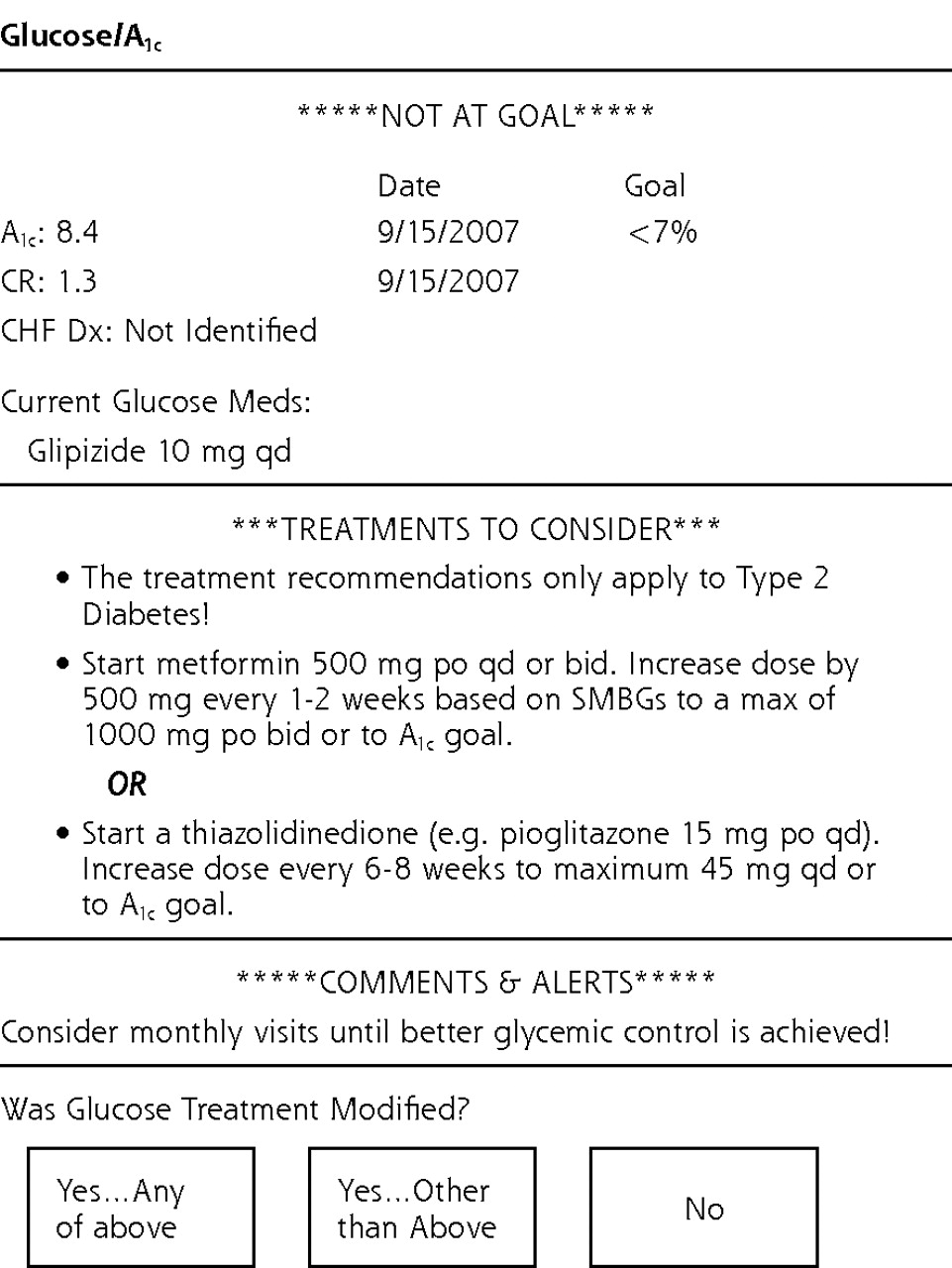
Example of Diabetes Wizard.
Diabetes Wizard recommendations are based on detailed clinical algorithms constructed by the research team (J.S.H., P.J.O.) consistent with evidence-based diabetes guidelines from the Institute for Clinical Systems Improvement and from other evidence-based sources.30–31 Diabetes Wizard provides recommendations in the following categories: (1) suggests specific changes in medications for patients not at individualized hemoglobin A1c, blood pressure, or lipid goals; (2) suggests changes in treatment for patients with contraindications to existing treatments (eg, metformin use in renal insufficiency or congestive heart failure), or being treated with potentially risky drug combinations (eg, concomitant β-blocker and nondihydropyridine calcium channel blocker); (3) suggests obtaining overdue laboratory tests, such as for potassium, serum creatinine, creatinine kinase, or liver function tests; and (4) suggests short follow-up intervals, such as monthly visits, for patients not at goal, because more frequent visits are associated with better chronic disease outcomes in many clinical trials.
After each office visit at which the Diabetes Wizard was deployed, the physician was asked to complete a brief (15 seconds per clinical domain) visit resolution form to indicate whether treatment was intensified at the time of the visit. The fastest way to complete the visit resolution form was to intensify pharmacotherapy for patients not at goal. Lifestyle advice was also considered an intervention. If no intervention occurred, physicians were asked to specify why not.
During the 6-month intervention period, physicians and clinics received monthly summaries and feedback to encourage high rates of Diabetes Wizard use and visit resolution form completion. Compensation was provided to encourage Diabetes Wizard use. Nursing staff at each intervention clinic collectively received $500 compensation for training time and increased workload during the 6-month intervention period. Consenting intervention group physicians were compensated $800 at the start of the intervention and another $800 after 6 months if they completed visit resolution forms for at least 70% of all diabetes encounters. After 6 months both compensation and feedback stopped, but intervention physicians were encouraged to continue to use the Diabetes Wizard, and use was tracked electronically for 15 more months.
Outcomes and Follow-up
The principal dependent variable was the preintervention to postintervention change in hemoglobin A1c, blood pressure, and LDL cholesterol levels. The baseline test value for hemoglobin A1c and LDL cholesterol was the first test during the intervention (or last preintervention test if there was no intervention value). For systolic and diastolic blood pressures, the baseline was the last preintervention value. For all tests, postintervention status was based on the last postintervention test value. All hemoglobin A1c assays were done at a single accredited clinical chemistry laboratory using a standard liquid chromatographic assay with a normal range of 4.5% to 6.1% and a coefficient of variation of 0.58% at a hemoglobin A1c value of 8.8%.32 LDL cholesterol values were calculated based on standard assays of total cholesterol, high-density lipoprotein (HDL) cholesterol, and 12-hour fasting triglycerides only when the triglyceride level was less than 400 mg/dL.33 No changes in these laboratory assay methods occurred during the study period. Blood pressure was measured according to office routine by nursing staff or physicians, who were periodically trained in proper blood pressure measurement technique. The blood pressure value in the primary EHR vital signs slot was selected for analysis.
Statistical Analysis
The independent variable of major interest was an indicator variable for the study arm. The interaction of study arm with time assessed the differential impact of the intervention across study arms on prespecified outcomes of hemoglobin A1c, systolic and diastolic blood pressure, and LDL cholesterol values. Because the trial was randomized at the clinic level, imbalance in patient characteristics was likely. Patient-level independent variables included age, sex, and validated indicator variables for coronary heart disease and congestive heart failure.34
This nested cohort pretest-posttest control group design accommodated clustering of occasion of measurement (baseline and postintervention) within patients who were nested within physicians who were nested within clinics. General and generalized linear mixed models with a repeated time measurement (baseline and postintervention) were used to analyze continuous (eg, laboratory values) and binary (eg, proportion of patients with a hemoglobin A1c test) outcomes using SAS Proc Mixed and Proc Glimmix (SAS Institute, Cary, North Carolina). These models included a term for study arm, time (baseline or postintervention), a time × study arm interaction term, and random intercepts to account for multiple levels of nesting. The time × study arm interaction term tested the effect of the intervention arm over time relative to the effect of the control arm over time. The analyses on test values were also conducted predicting postintervention values from study arm, preintervention test value, and patient covariates. Because of the similarity in results from these two approaches, we report the findings from the time × study arm approach.
Denominators for the analysis of test rates, encounter rates, and numbers of tests and encounters included the full set of eligible patients linked to study-consenting physicians. Patients with diabetes encounters in the postintervention period and not at goal at baseline (eg, hemoglobin A1c ≥7%, blood pressure ≥130/80 mm Hg, LDL cholesterol ≥100 mg/dL [≥70 mg/dL for coronary heart disease]) comprised the denominator for analysis examining change in hemoglobin A1c levels. Patients with diabetes encounters and at goal at baseline (eg, hemoglobin A1c <7%, systolic blood pressure <130 mm Hg, diastolic blood pressure <80 mm Hg, LDL cholesterol <100 mg/dL [<70 mg/dL for coronary heart disease]) comprised the denominator for analysis examining maintenance of clinical goals at the last follow-up measurement. For analyses of laboratory values, patients missing a value at baseline were not included in the analysis because we were unable to determine whether such cases were at goal at baseline. Patients without a postintervention value, however, were included through restricted maximum likelihood estimation, which uses information from patients with partially missing data.35 A priori sample size calculations assumed an analytic sample of 500 diabetes patients per study arm, based on 20 physicians with 25 diabetes patients not at goal on hemoglobin A1c measurements. Effective patient sample size was estimated as n = 291 per arm because of clustering of patients within physicians (estimated intraclass correlation coefficient = 0.03). This study was designed with 80% power to detect a difference of 0.3% in hemoglobin A1c levels between study arms, with a 2-tailed α=.05; α levels were not adjusted for testing 3 principal dependent variables.
RESULTS
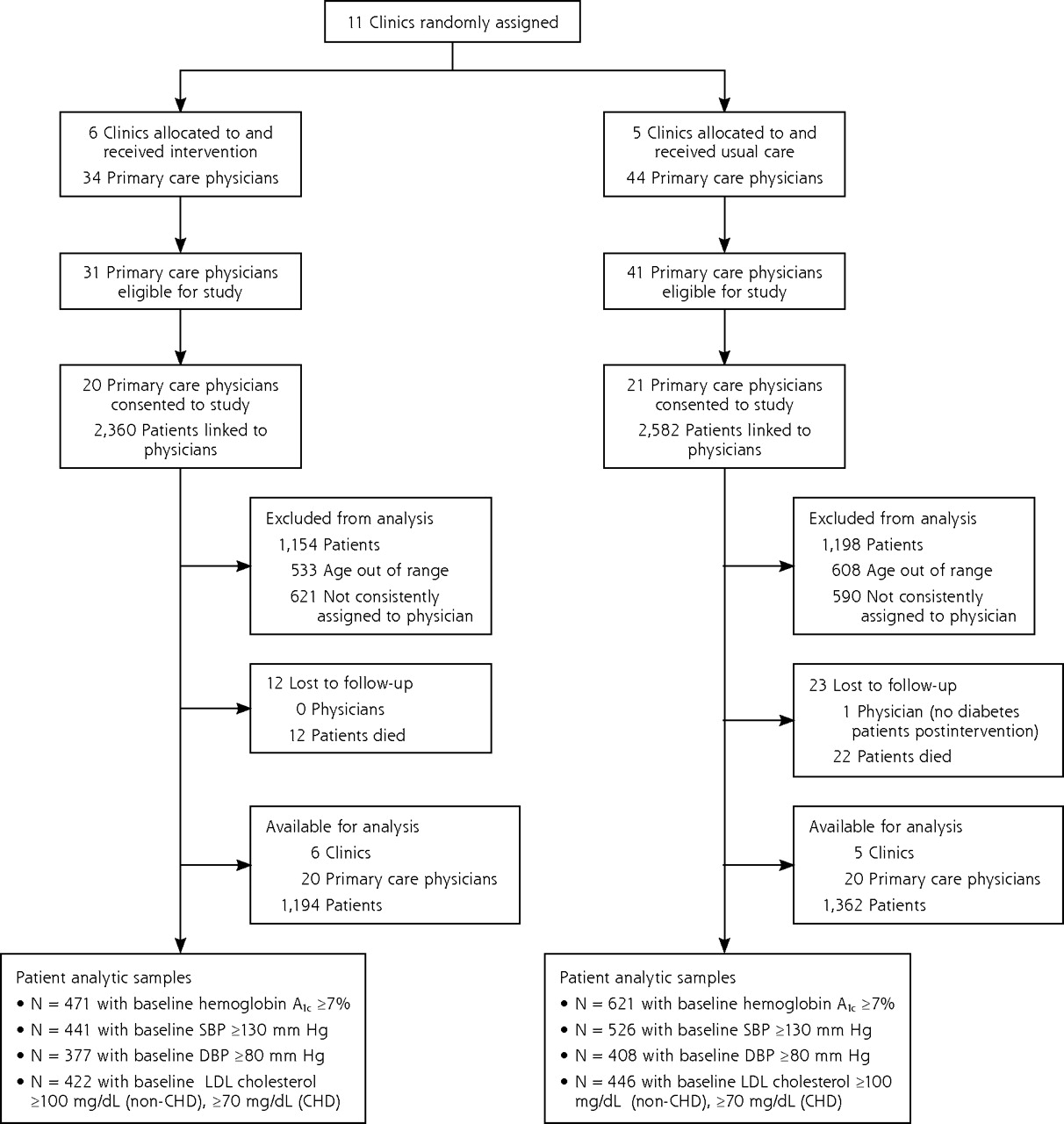
Of the 11 clinics, 6 were randomly allocated to the study arm, and 5 to the usual care arm. From these clinics 40 physicians enrolled in the study, 20 in each study arm, with 2,556 eligible patients, 1,194 in the intervention arm, and 1,362 in the control arm. The allocation of clinics, physicians, and patients to study arm is shown in Figure 2⇓.
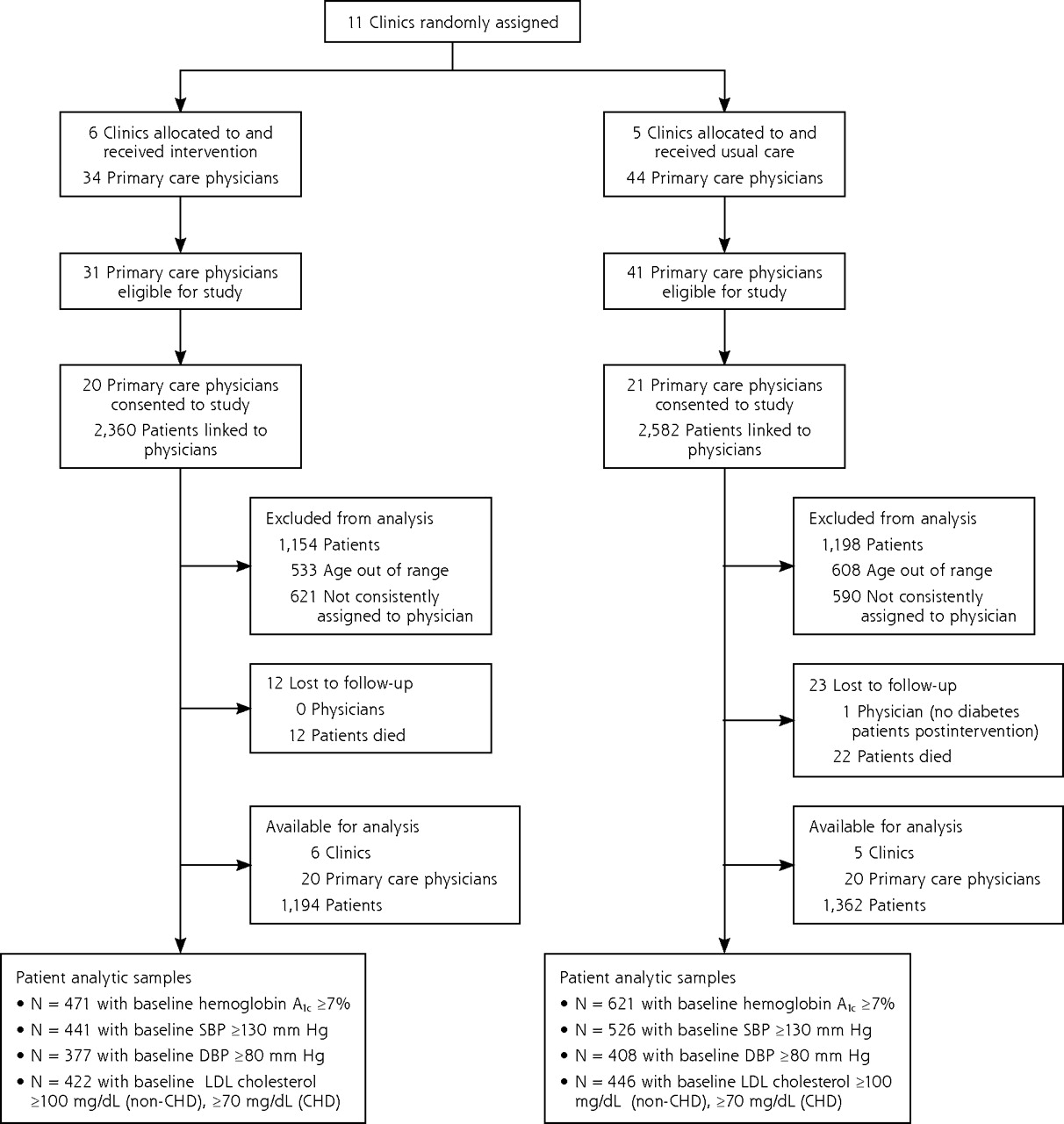
Diagram illustrating randomization and disposition of clinics, primary care physicians, and diabetes patients.
Attributes of study participants are displayed in Table 1⇓. At baseline, 47.8% of diabetes patients had hemoglobin A1c levels of <7%, 59.1% had systolic blood pressures of <130 mm Hg, 65.6% had diastolic blood pressures of <80 mm Hg, and 59.9% had LDL cholesterol <100 mg/dL. The range of diabetes patients per study-enrolled physician was 10 to 100 with a mean of 49.7 (SD = 25.0). Randomization at the clinic level resulted in an intervention arm with a higher proportion of male and white patients, and with higher baseline diastolic blood pressure and LDL cholesterol values than patients in the control arm. Intervention arm clinics had a higher proportion of family practice physicians than control arm clinics.
Characteristics of Study Physicians and Diabetes Patients Linked to Those Study Physicians at Intervention and Control Clinics
In 4-level random intercept models (measurement occasion nested within patient, physician, and clinic), intraclass correlations (ICCs) at the clinic level were small, with values of ICC ≤0.0002 for hemoglobin A1c, systolic and diastolic blood pressures, and LDL cholesterol. Because of the low ICCs at the clinic level, 3-level models are presented by dropping the random intercept term for clinic.
Table 2⇓ shows relatively high baseline and follow-up blood pressure and LDL cholesterol test rates, and little intervention effect on these measures during the study period. Proportion of patients with a hemoglobin A1c test increased more in the intervention than control group (P = .045), but the mean number of hemoglobin A1c (P = .09) and LDL cholesterol tests (P = .09) per patient was not affected by the intervention.
Rates and Counts of Diabetes Encounters, Glycated Hemoglobin Tests, Low-Density Lipoprotein Cholesterol Tests, and Blood Pressure Measures, Comparing Intervention and Control Clinics in the Preintervention and Postintervention Periods
Table 3⇓ shows that hemoglobin A1c levels, systolic and diastolic blood pressures, and LDL cholesterol values each significantly improved with time in both study arms (all P <.001). Intervention arm patients had a significantly greater (−0.26%) improvement in hemoglobin A1c levels than control arm patients (95% confidence interval [CI], −0.06% to −0.47%; time ×condition P=.01). Although intervention and control arm patients had similar decreases in systolic blood pressures, intervention arm patients with controlled systolic blood pressure at baseline were more likely to remain in control than control arm patients (80.2% vs 75.1%, P=.03). The intervention had no significant positive or negative impact on diastolic blood pressure and LDL cholesterol values or proportion remaining in control for hemoglobin A1c, diastolic blood pressure, or LDL cholesterol values. Intervention benefits on hemoglobin A1c levels occurred in both sexes and in both white and nonwhite patients.
Changes and Proportion of Adult Diabetes Patients at Goal on Glycated Hemoglobin, Blood Pressure, and LDL Cholesterol Measures Among Intervention and Control Group Primary Care Physicians and Clinics in the Preintervention (Baseline) and Postintervention Periods
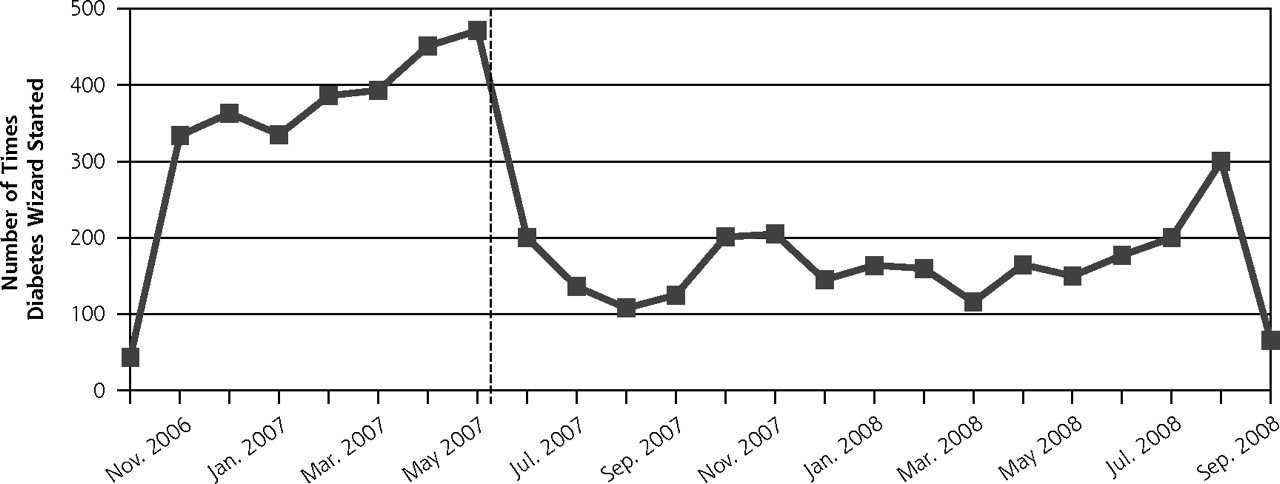
During the 6-month period when use of the EHR-based clinical decision support system was reinforced by financial incentives and feedback, the Diabetes Wizard was opened at 62.6% of all visits made by diabetes patients to intervention physicians. After discontinuation of incentives and feedback, use of the Diabetes Wizard at the intervention clinics persisted at a lower level for 12 more months (Figure 3⇓). Control group clinics did not have access to the intervention during the 18-month study. In a postintervention survey of 20 intervention group physicians, 17 of 18 respondents reported being completely satisfied or satisfied with this decision support system.
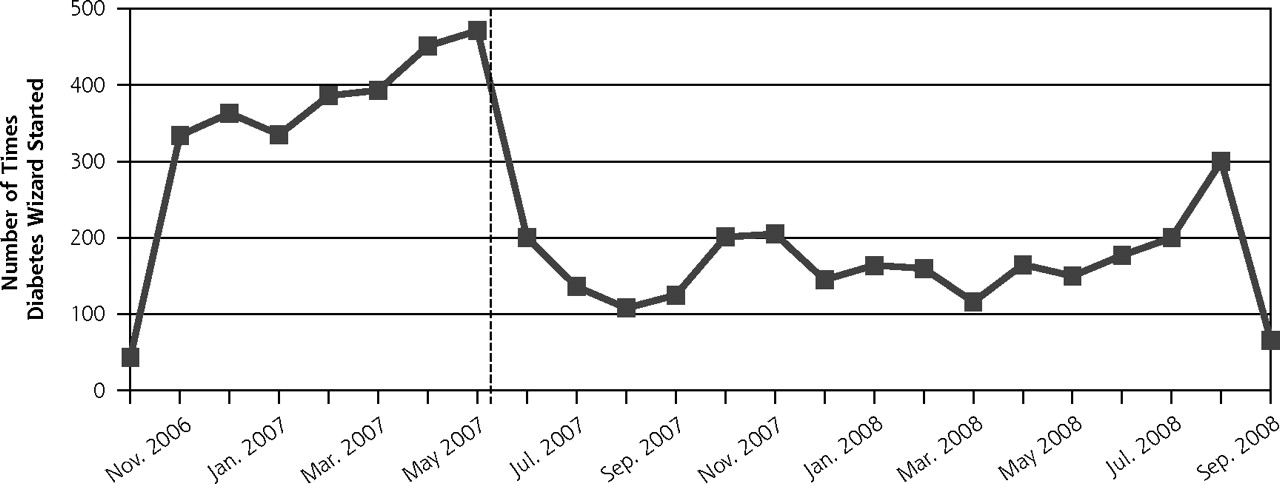
Diabetes Wizard use during and after intervention for the intervention group only.
During the 6-month intervention period, physicians were asked to complete the Visit Resolution Form at the conclusion of each visit at which the Diabetes Wizard was used. Physicians reported intensifying glucose treatment in 536 of 866 (61.9%) visits when the hemoglobin A1c level was >7%. Blood pressure treatment was intensified at 363 of 832 visits (43.6%) when blood pressure was >130/80 mm Hg at that visit; note that Diabetes Wizard deployed whenever the current blood pressure was ≥130/80 mm Hg, even if the patient’s blood pressure was within target range at the prior visit. Rates of lipid treatment intensification were lower at 310 of 1,652 visits (18.8%) when lipids were not at goal. Analysis of EHR data on newly prescribed drugs, however, did not show significantly different rates for those with a hemoglobin A1c level of ≥7% (10.7% vs 10.5%, P = .86) or blood pressure of ≥130/80 mm Hg (13.9% vs.14.0%, P = .98), although new lipid drugs were prescribed more often in the intervention group for those with a LDL cholesterol value of ≥100 mg/dL (9.1% vs 5.6%, P = .001). These data, taken together, suggest that many of the treatment intensifications reported by intervention group physicians were related to drug dose titrations (rather than newly prescribed drugs), or to lifestyle advice or interventions.
DISCUSSION
These data show that an EHR-based clinical decision support system led to modest but significant improvements in glucose control and some aspects of blood pressure control. Primary care physicians reported high levels of satisfaction with the intervention and had high rates of use of the clinical decision support system during the intervention period and continued to use the technology for more a year after incentives and feedback were discontinued, although at a lower rate. Patients of intervention physicians who were and were not exposed directly to the clinical decision support system had comparable improvement in hemoglobin A1c levels and systolic blood pressure during the follow-up period. This finding suggests that physicians were able to transfer what they learned from using the clinical decision support system with some patients to the care of other patients—an important challenge and desirable finding in learning research.
This clinical decision support system used a strategy of personalization. As Figure 2⇑ shows, clinical decision support went beyond prompts and reminders to include drug-specific treatment suggestions based on each patient’s current treatment; distance from clinical goal, comorbidities, and renal and hepatic function. This type of clinical decision support system simultaneously standardizes and personalizes diabetes care. As personalization of chronic disease care increases in the coming era of genomic medicine, EHR-embedded clinical decision support may become an essential tool needed to systematically process complex risk prediction data and then accurately identify appropriate clinical goals and high-priority treatment options for each patient at each clinical encounter.36,37
In this study, the use of EHR-based clinical decision support technology was reinforced by changes in clinic rooming procedures, changes in nurse roles, and provision of incentives to physicians and clinic staff—elements that were lacking in previous failed attempts to implement EHR-based clinical decision support. Physicians were provided clinical decision support information immediately before the start of the visit to facilitate visit planning.8,38 Although this intervention was well-received by physicians, it is uncertain whether high levels of use and satisfaction can be replicated when financial compensation is replaced by other incentives, such as pay-for-performance programs or public reporting of chronic disease quality of care.39
The study was conducted in a medical group with relatively good baseline diabetes care, and the magnitude of clinical improvement was quite modest. Even so, these modest results provide proof of concept that (1) under certain circumstance primary care physicians will use sophisticated point-of-care clinical decision support systems, and (2) when such clinical decision support systems are used, they can improve several intermediate outcomes of chronic disease care. Further efforts to strengthen the impact of clinical decision support on chronic disease care are justified and are already underway. Such efforts include prioritizing care recommendations based on benefit to the patient, enhancing the clinical decision support interface with physicians, and developing engaging and informative interfaces with patients that elicit and integrate patient preferences for care.40
Interpretation of our results is limited by several factors. First, the study site had relatively good baseline levels of diabetes care. The impact of clinical decision support in other practice settings may be greater or less than what we observed. Second, studies that explore alternative and less-expensive incentive strategies are needed.41 Third, additional work is needed to elucidate more precisely the specific mechanisms that were responsible for the observed effects of this intervention.
Despite these limitations, our data provide proof-of-concept that an EHR-based clinical decision support system can improve key intermediate outcomes of diabetes care in primary care settings. The observed clinical impact, although modest, is comparable to that achieved by many disease management or patient education programs that are more expensive.42–46 EHR-based clinical decision support is scalable and can be used in conjunction with additional care improvement strategies. In the coming era of personalized medicine, clinical decision support strategies capable of simultaneously standardizing and personalizing clinical care will likely become an essential tool in primary care, and investments to further enhance the effectiveness of this technology are urgently needed.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: This project was funded by National Institute of Diabetes, Digestive, and Kidney Diseases (NIDDK) grant # R01 DK068314 to HealthPartners Research Foundation.
-
Trial Registration: clinicaltrials.gov NCT00272402.
- Received for publication March 29, 2010.
- Revision received August 23, 2010.
- Accepted for publication August 27, 2010.
- © 2011 Annals of Family Medicine, Inc.
REFERENCES





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Harnessing the power of clinical decision support systems: challenges and opportunities
- Does Clinical Decision Support Increase Appropriate Medication Prescribing for Cardiovascular Risk Reduction?
- A systematic review of ontology-based clinical decision support system rules: usage, management, and interoperability
- CONSORT extension for the reporting of randomised controlled trials conducted using cohorts and routinely collected data (CONSORT-ROUTINE): checklist with explanation and elaboration
- Benefits and harms of intensive glycemic control in patients with type 2 diabetes
- CM-SHARE: Development, Integration, and Adoption of an Electronic Health Record-Linked Digital Health Solution to Support Care for Diabetes in Primary Care
- Interventional study to improve diabetic guidelines adherence using mobile health (m-Health) technology in Lahore, Pakistan
- Strategies to Prioritize Clinical Options in Primary Care
- The breadth and burden of data collection in clinical practice
- Refutation : Les dossiers medicaux electroniques ameliorent-ils la qualite des soins?: Oui
- Rebuttal: Do electronic medical records improve quality of care?: Yes
- Horses and buggies have some advantages over cars, but no one is turning back
- An Internet-Based Diabetes Management Platform Improves Team Care and Outcomes in an Urban Latino Population
- Response to Comment on O'Connor et al. Randomized Trial of Telephone Outreach to Improve Medication Adherence and Metabolic Control in Adults With Diabetes. Diabetes Care 2014;37:3317-3324
- Randomized Trial of Telephone Outreach to Improve Medication Adherence and Metabolic Control in Adults With Diabetes
- Standards of Medical Care in Diabetes--2014
- Standards of Medical Care in Diabetes--2013
- Quality improvement collaboratives in the age of health informatics--new wine in new wineskins
- Validation of prescribing appropriateness criteria for older Australians using the RAND/UCLA appropriateness method
- Typical Electronic Health Record Use in Primary Care Practices and the Quality of Diabetes Care
- Standards of Medical Care in Diabetes--2012
- Consensus Report: Diabetes Performance Measures: Current Status and Future Directions
- Diabetes Performance Measures: Current Status and Future Directions
- Courage and Change
- In This Issue: Clinical Decision Support