
Determinants of Diabetes Disease Management, 2011–2019

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Software
2.2. Dependent Variables
- About how often do you check your blood for glucose or sugar? (BLDSUGAR).
- About how many times in the past 12 months have you seen a doctor, nurse, or other health professional for your diabetes? (DOCTDIAB).
- About how many times in the past 12 months has a health professional checked your feet for any sores or irritations? (FEETCHK).
- About how many times in the past 12 months has a doctor, nurse, or other health professional checked you for A1C? (CKHEMO3).
- Have you ever taken a course or class in how to manage your diabetes yourself? (DIABEDU).
- When was the last time you had an eye exam in which the pupils were dilated, making you temporarily sensitive to bright light? (EYEEXAM1).
2.3. Independent Variables
2.3.1. Demographics
2.3.2. Socioeconomic Status
2.3.3. Health Status
2.4. Medicaid Expansion Linear Splines
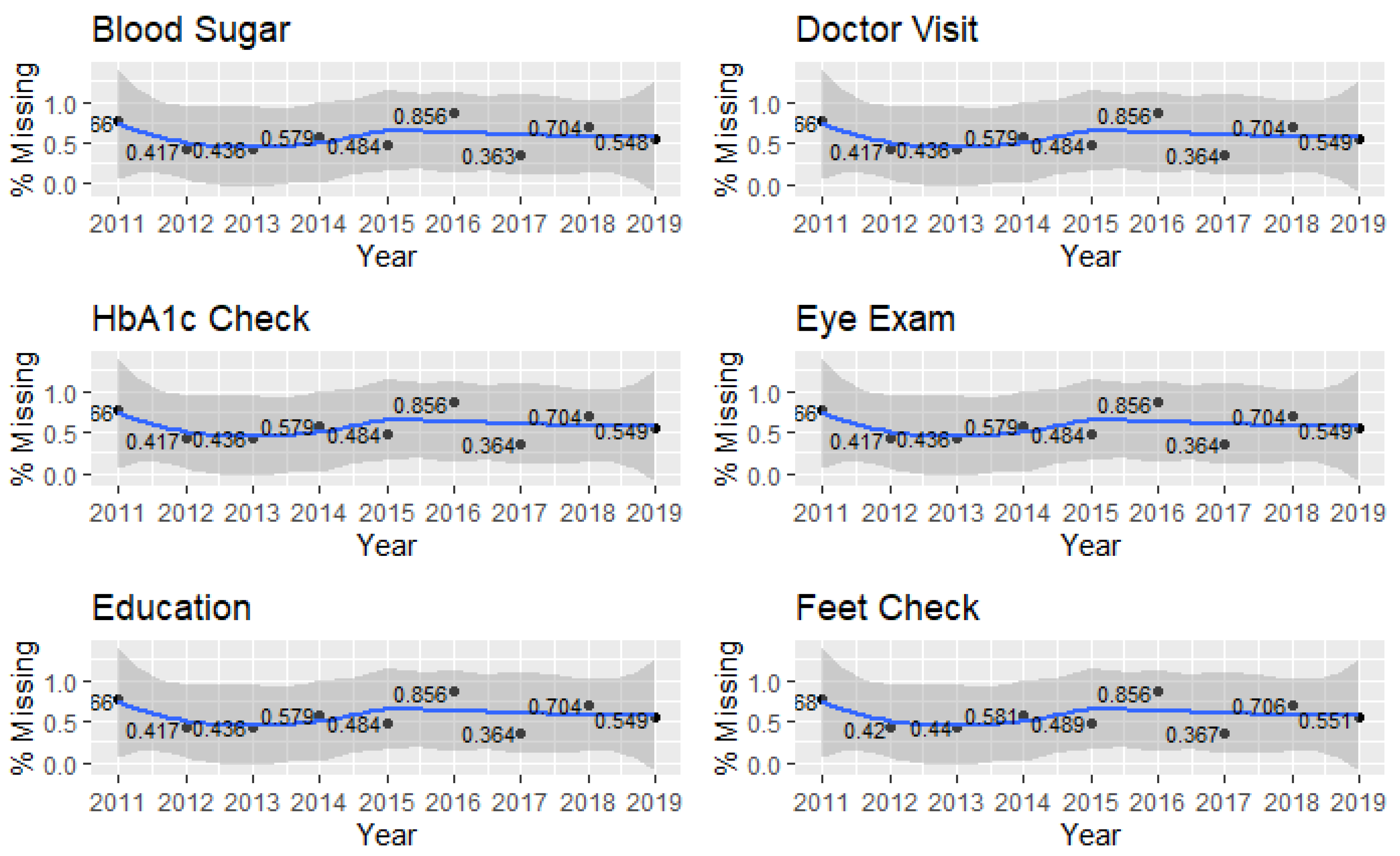
2.5. Missing Data
2.6. Inferential Methods
3. Results
3.1. Descriptive Statistics
3.1.1. Dependent Variables
3.1.2. Demographics
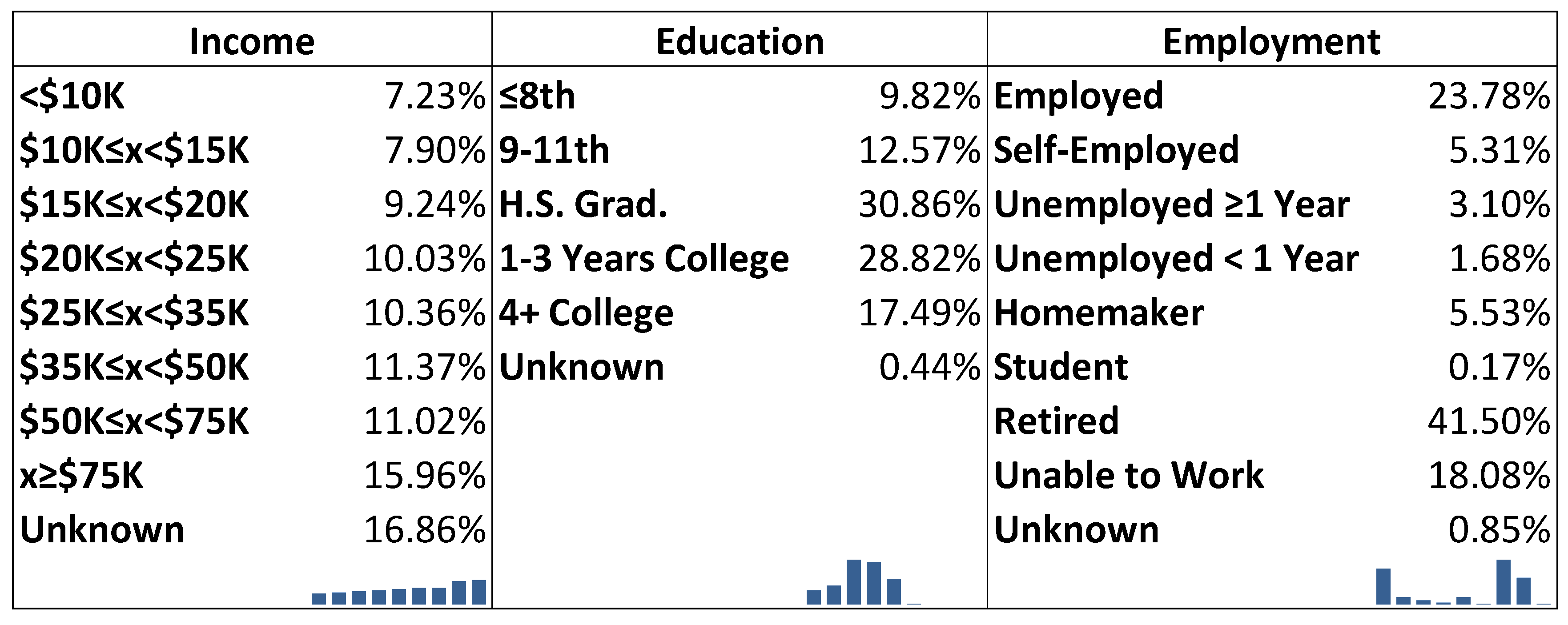
3.1.3. Socioeconomic Status
3.1.4. Health Status
3.2. Inferential Statistics
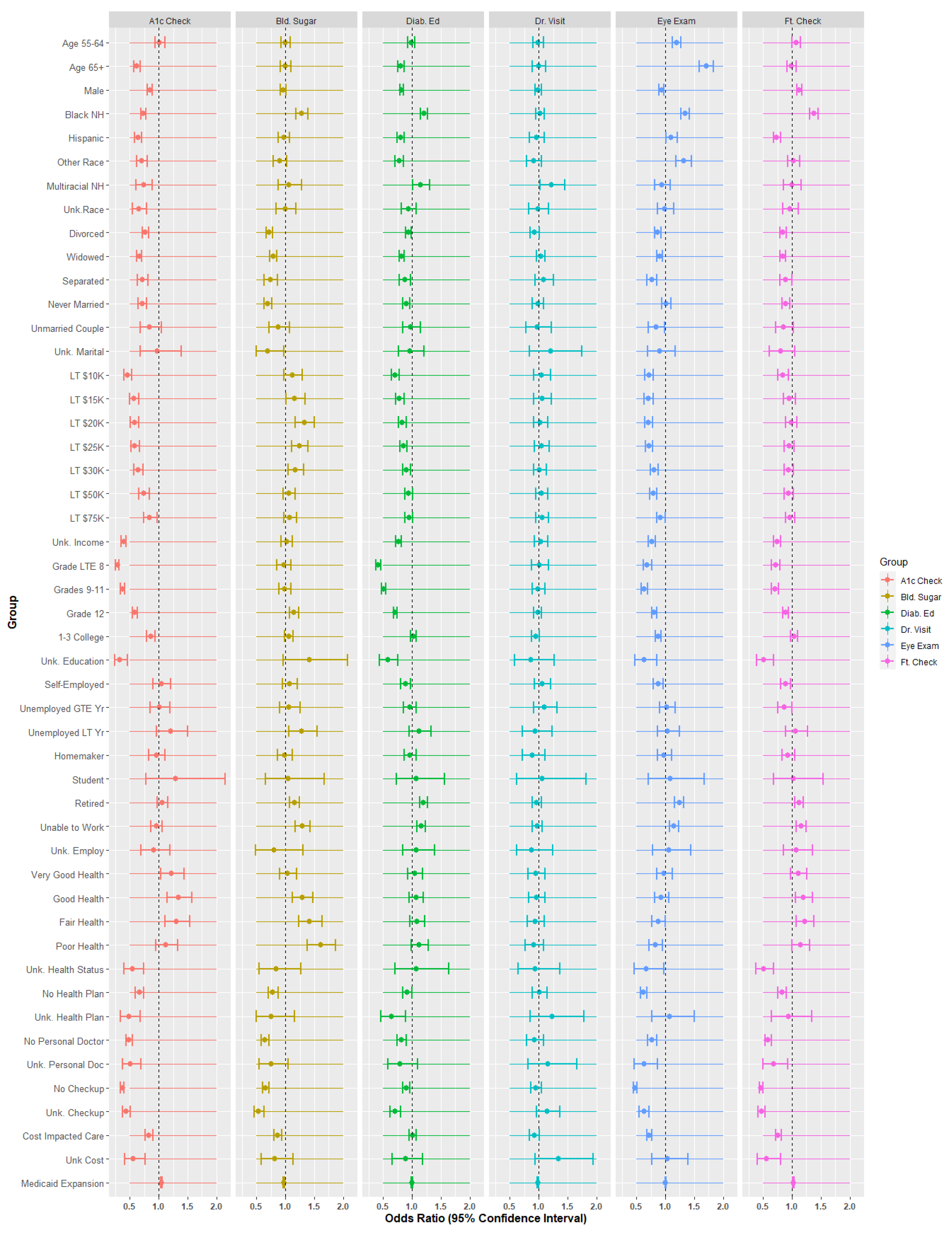
3.2.1. Effect Sizes
3.2.2. Demographic Analysis
3.2.3. Socioeconomic Status
3.2.4. Health Status
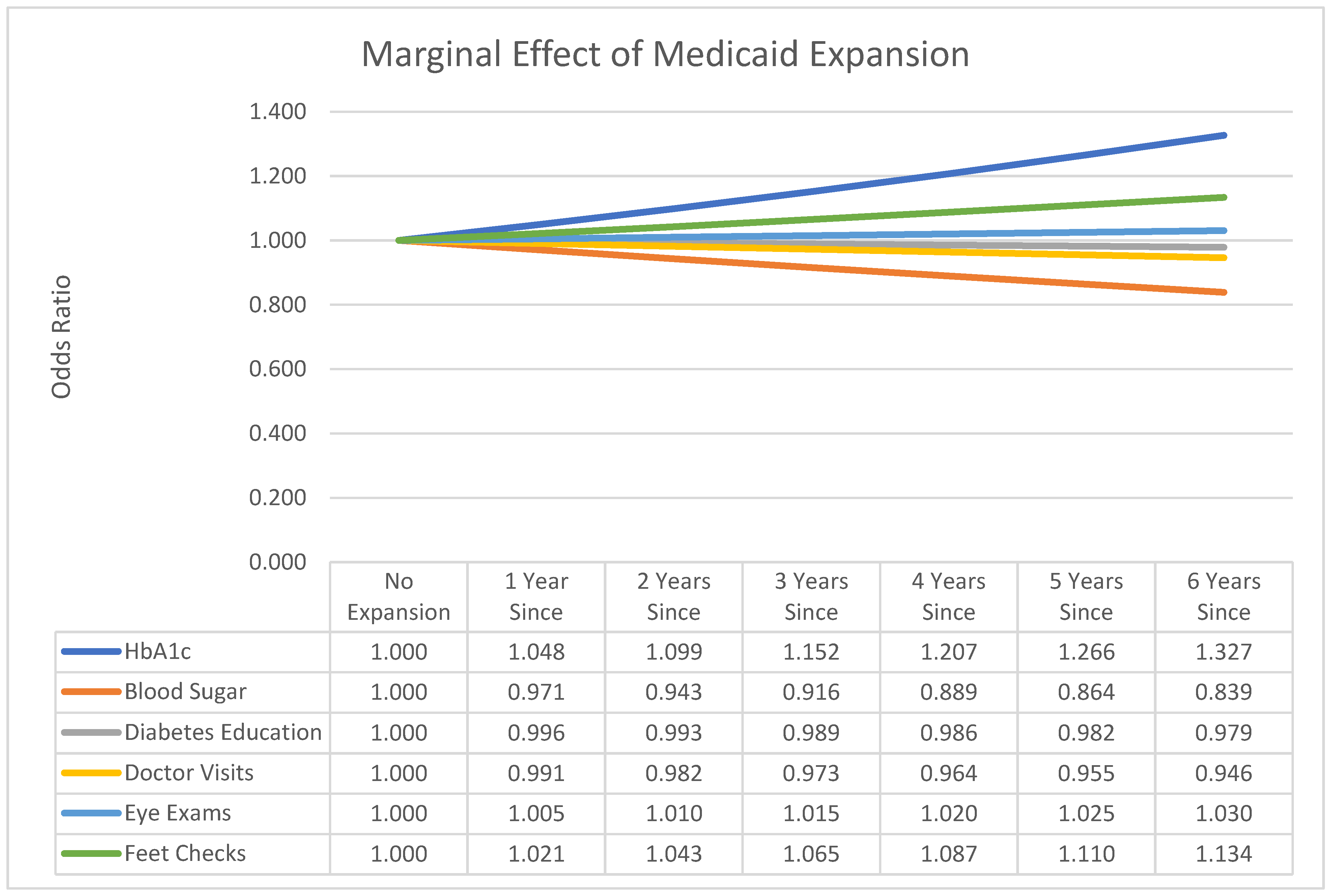
3.2.5. Medicaid Expansion
3.2.6. Sub-Model Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Protection, P.; Act, A.C. Patient protection and affordable care act. Public Law. 2010, 111, 759–762. [Google Scholar]
- Census. Health Insurance Coverage in the United States: 2014–2015. Available online: https://www.census.gov/library/publications/2015/demo/p60-253.html (accessed on 20 July 2021).
- Smith, J.C.; Medalia, C. Health Insurance Coverage in the United States: 2013; US Department of Commerce, Economics and Statistics Administration, Bureau: Washington, DC, USA, 2014.
- Berchick, E.R.; Hood, E.; Barnett, J.C. Health Insurance Coverage in the United States: 2018; Department of Commerce: Washington, DC, USA, 2019.
- Karpman, M.; Long, S.K.; Bart, L. The Affordable Care Act’s Marketplaces Expanded Insurance Coverage for Adults with Chronic Health Conditions. Health Aff. 2018, 37, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Burge, M.R.; Schade, D.S. Diabetes and the Affordable Care Act. Diabetes Technol. Ther. 2014, 16, 399–413. [Google Scholar] [CrossRef]
- KFF. Status of State Medicaid Decisions: Interactive Map 2020. Available online: https://www.kff.org/medicaid/issue-brief/status-of-state-medicaid-expansion-decisions-interactive-map/ (accessed on 20 July 2021).
- CDC. National Diabetes Statistics Report, 2020. Atlanta, GA: Centers for Disease Control and Prevention; US Department of Health and Human Services: Washington, DC, USA, 2020; pp. 12–15.
- Nagi, D.; Hambling, C.; Taylor, R. Remission of type 2 diabetes: A position statement from the Association of British Clinical Diabetologists (ABCD) and the Primary Care Diabetes Society (PCDS). Br. J. Diabetes Vasc. Dis. 2019, 19, 73–76. [Google Scholar] [CrossRef] [Green Version]
- Oh, W.; Kim, E.; Castro, M.R.; Caraballo, P.J.; Kumar, V.; Steinbach, M.S.; Simon, G.J. Type 2 Diabetes Mellitus Trajectories and Associated Risks. Big Data 2016, 4, 25–30. [Google Scholar] [CrossRef]
- Molinaro, R.; Dauscher, C. Complications resulting from uncontrolled diabetes. MLO Med. Lab. Obs. 2017, 49, 20–22. [Google Scholar]
- Lorig, K.R.; Sobel, D.S.; Stewart, A.L.; Brown, B.W., Jr.; Bandura, A.; Ritter, P.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial. Med. Care 1999, 37, 5–14. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E. A Practical Model of Diabetes Management and Education. Diabetes Care 1995, 18, 117–126. [Google Scholar] [CrossRef]
- Lee, J.; Callaghan, T.; Ory, M.; Zhao, H.; Bolin, J.N. The Impact of Medicaid Expansion on Diabetes Management. Diabetes Care 2019, 43, 1094–1101. [Google Scholar] [CrossRef] [Green Version]
- Association, A.D. Glycemic targets: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43 (Suppl. 1), S66–S76. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Grothaus, L.C.; Sandhu, N.; Galvin, M.S.; McGregor, M.; Artz, K.; Coleman, E.A. Chronic care clinics for diabetes in primary care: A system-wide randomized trial. Diabetes Care 2001, 24, 695–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myerson, R.; Laiteerapong, N. The Affordable Care Act and Diabetes Diagnosis and Care: Exploring the Potential Impacts. Curr. Diabetes Rep. 2016, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Huguet, N.; Springer, R.; Marino, M.; Angier, H.; Hoopes, M.; Holderness, H.; DeVoe, J.E. The Impact of the Affordable Care Act (ACA) Medicaid Expansion on Visit Rates for Diabetes in Safety Net Health Centers. J. Am. Board Fam. Med. 2018, 31, 905–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, M.; Angier, H.; Springer, R.; Valenzuela, S.; Hoopes, M.; O’Malley, J.; Suchocki, A.; Heintzman, J.; DeVoe, J.; Huguet, N. The Affordable Care Act: Effects of Insurance on Diabetes Biomarkers. Diabetes Care 2020, 43, 2074–2081. [Google Scholar] [CrossRef]
- Benitez, J.A.; Adams, E.K.; Seiber, E.E. Did Health Care Reform Help Kentucky Address Disparities in Coverage and Access to Care among the Poor? Health Serv. Res. 2017, 53, 1387–1406. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.E.; Holtzman, D.; Bolen, J.; Stanwyck, C.A.; Mack, K.A. Reliability and validity of measures from the Behavioral Risk Factor Surveillance System (BRFSS). Soz. Prav. 2001, 46, S3–S42. [Google Scholar]
- Iachan, R.; Pierannunzi, C.; Healey, K.; Greenlund, K.J.; Town, M. National weighting of data from the Behavioral Risk Factor Surveillance System (BRFSS). BMC Med Res. Methodol. 2016, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Team DTF. Diabetes. 2021. Available online: https://rpubs.com/R-Minator/diabetes2 (accessed on 20 July 2021).
- R Core Team. R: A Language and Environment for Statistical Computing. 2018. Available online: https://www.r-project.org/ (accessed on 22 July 2021).
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Kagerer, K. A Short Introduction to Splines in Least Squares Regression Analysis. 2013. Available online: https://epub.uni-regensburg.de/27968/ (accessed on 22 July 2021).
- Fox, J.; Weisberg, S. An R Companion to Applied Regression: Sage Publications. 2018. Available online: https://socialsciences.mcmaster.ca/jfox/Books/Companion/ (accessed on 22 July 2021).
- Census. QuickFacts. 2020. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045219 (accessed on 20 July 2021).
- Stone, M. An asymptotic equivalence of choice of model by cross-validation and Akaike’s criterion. J. R. Stat. Soc. Ser. B Methodol. 1977, 39, 44–47. [Google Scholar] [CrossRef]
- Ryan, A.M.; Gee, G.C.; Griffith, D. The Effects of Perceived Discrimination on Diabetes Management. J. Health Care Poor Underserved 2008, 19, 149–163. [Google Scholar] [CrossRef]
- Krämer, H.U.; Rüter, G.; Schöttker, B.; Rothenbacher, D.; Rosemann, T.; Szecsenyi, J.; Brenner, H.; Raum, E. Gender differences in healthcare utilization of patients with diabetes. Am. J. Manag. Care 2012, 18, 362–369. [Google Scholar] [PubMed]
- Asmelash, D.; Abdu, N.; Tefera, S.; Baynes, H.W.; Derbew, C. Knowledge, Attitude, and Practice towards Glycemic Control and Its Associated Factors among Diabetes Mellitus Patients. J. Diabetes Res. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, P.; Savage, C.; Niederbaumer, P.; Anthony, J. A Study of the Level of Knowledge about Diabetes Management of Low-Income Persons with Diabetes. J. Community Health Nurs. 2005, 22, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Al-Rasheedi, A.A.S. The role of educational level in glycemic control among patients with type II diabetes mellitus. Int. J. Health Sci. 2014, 8, 177. [Google Scholar] [CrossRef]
- Blaum, C.S.; Velez, L.; Hiss, R.G.; Halter, J.B. Characteristics Related to Poor Glycemic Control in NIDDM Patients in Community Practice. Diabetes Care 1997, 20, 7–11. [Google Scholar] [CrossRef]
- Chaturvedi, N.; Stephenson, J.M.; Fuller, J.H. The relationship between socioeconomic status and diabetes control and complications in the EURODIAB IDDM Complications Study. Diabetes Care 1996, 19, 423–430. [Google Scholar] [CrossRef]
- Myerson, R.; Lu, T.; Peters, A.; Fox, S.; Huang, E. Impact of Health Insurance Policy on Diabetes Management; Springer Science and Business Media LLC: Berlin, Germany, 2020; pp. 491–504. [Google Scholar]
- Heisler, M.; Bouknight, R.R.; Hayward, R.A.; Smith, D.M.; Kerr, E.A. The relative importance of physician communication, participatory decision making, and patient understanding in diabetes self-management. J. Gen. Intern. Med. 2002, 17, 243–252. [Google Scholar] [CrossRef] [Green Version]
- Census. Income, Poverty, and Health Insurance: 2018; U.S. Department of Commerce: Washington, DC, USA, 2019.
- Garfield, R.; Orgera, K.; Damico, A. The uninsured and the ACA: A primer-key facts about health insurance and the uninsured amidst changes to the affordable care act. Kaiser Fam. Found. 2019, 25, 1–28. [Google Scholar]
- Casagrande, S.S.; McEwen, L.N.; Herman, W.H. Changes in Health Insurance Coverage under the Affordable Care Act: A National Sample of U.S. Adults with Diabetes, 2009 and 2016. Diabetes Care 2018, 41, 956–962. [Google Scholar] [CrossRef] [Green Version]
- Myerson, R.; Romley, J.; Chiou, T.; Peters, A.L.; Goldman, D. The Affordable Care Act and Health Insurance Coverage among People with Diagnosed and Undiagnosed Diabetes: Data from the National Health and Nutrition Examination Survey. Diabetes Care 2019, 42, e179–e180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Salm, M.; van Soest, A. The effect of retirement on healthcare utilization: Evidence from China. J. Health Econ. 2018, 62, 165–177. [Google Scholar] [CrossRef]
- McCulloch, D.K.; Price, M.J.; Hindmarsh, M.; Wagner, E.H. A population-based approach to diabetes management in a primary care setting: Early results and lessons learned. Eff. Clin. Pract. ECP 1998, 1, 12–22. [Google Scholar] [PubMed]
- Marshall, M.; Roland, M. The Future of the Quality and Outcomes Framework in England. Br. Med J. 2017, 359, j4681. [Google Scholar] [CrossRef]
- Zhang, D.; Ritchey, M.R.; Park, C.; Li, J.; Chapel, J.; Wang, G. Association between Medicaid Coverage and Income Status on Health Care Use and Costs among Hypertensive Adults after Enactment of the Affordable Care Act. Am. J. Hypertens. 2019, 32, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A.L.; Sommers, B.D. Among Low-Income Adults Enrolled in Medicaid, Churning Decreased after The Affordable Care Act: This study examines whether the Affordable Care Act’s expansion of Medicaid eligibility had an impact on coverage disruptions–known as “churning”–among Medicaid enrollees. Health Aff. 2020, 39, 85–93. [Google Scholar]
- CDC. Survey Data & Documentation. 2020. Available online: https://www.cdc.gov/brfss/data_documentation/index.htm (accessed on 20 July 2021).
- Garfield, R.L.; Damico, A. Medicaid Expansion Under Health Reform May Increase Service Use and Improve Access for Low-Income Adults with Diabetes. Health Aff. 2012, 31, 159–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | # of Factor Levels | Unknown | % Unknown | |
|---|---|---|---|---|
| Age | Categorical | 3 | - | 0.00% |
| Race | Categorical | 6 | 9701 | 1.90% |
| Gender | Categorical | 3 | 207 | 0.04% |
| Marital Status | Categorical | 7 | 2612 | 0.51% |
| Income | Categorical | 9 | 88,018 | 17.22% |
| Education | Categorical | 6 | 2169 | 0.42% |
| Work Status | Categorical | 9 | 3704 | 0.72% |
| Health Plan | Categorical | 3 | 1452 | 0.28% |
| Personal Doctor | Categorical | 3 | 1826 | 0.36% |
| Annual Checkup | Categorical | 3 | 8075 | 1.58% |
| Cost Affected Care | Categorical | 3 | 1890 | 0.37% |
| Health Status | Categorical | 6 | 2252 | 0.44% |
| Medicaid Expansion | Quantitative | N/A | - | 0.00% |
| HbA1c | Bld. Sugar | Diab. Ed. | Dr. Visit | Eye Exam | Ft. Check | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | 26.418 | *** | 4.808 | *** | 1.915 | *** | 6.731 | *** | 3.135 | *** | 3.055 | *** |
| Age 55–64 | 1.015 | 0.998 | 0.985 | 0.986 | 1.190 | *** | 1.072 | * | ||||
| Age 65+ | 0.623 | *** | 1.001 | 0.805 | *** | 1.000 | 1.704 | *** | 0.992 | |||
| Male | 0.846 | *** | 0.961 | 0.820 | *** | 0.991 | 0.932 | *** | 1.128 | *** | ||
| Black | 0.731 | *** | 1.283 | *** | 1.205 | *** | 1.021 | 1.337 | *** | 1.375 | *** | |
| Hispanic | 0.638 | *** | 0.968 | 0.802 | *** | 0.961 | 1.103 | * | 0.736 | *** | ||
| Other | 0.709 | *** | 0.899 | 0.776 | *** | 0.912 | 1.314 | *** | 1.024 | |||
| Multirace | 0.736 | ** | 1.060 | 1.149 | * | 1.214 | * | 0.936 | 0.995 | |||
| Unk. Race | 0.660 | *** | 0.995 | 0.938 | 0.985 | 0.991 | 0.961 | |||||
| Divorced | 0.769 | *** | 0.719 | *** | 0.940 | * | 0.929 | + | 0.869 | *** | 0.845 | *** |
| Widowed | 0.662 | *** | 0.790 | *** | 0.821 | *** | 1.036 | 0.896 | *** | 0.844 | *** | |
| Separated | 0.716 | *** | 0.740 | *** | 0.872 | * | 1.083 | 0.764 | *** | 0.894 | + | |
| Nvr. Married | 0.711 | *** | 0.692 | *** | 0.899 | ** | 0.987 | 1.016 | 0.895 | ** | ||
| Unm. Couple | 0.840 | 0.880 | 0.979 | 0.977 | 0.835 | * | 0.859 | + | ||||
| Unk. Relationship | 0.974 | 0.695 | * | 0.964 | 1.211 | 0.900 | 0.802 | |||||
| <$10 K | 0.466 | *** | 1.123 | 0.709 | *** | 1.047 | 0.712 | *** | 0.839 | ** | ||
| <$15 K | 0.571 | *** | 1.162 | * | 0.784 | *** | 1.055 | 0.707 | *** | 0.952 | ||
| <$20 K | 0.579 | *** | 1.323 | *** | 0.830 | *** | 1.026 | 0.703 | *** | 0.986 | ||
| <$25 K | 0.588 | *** | 1.241 | *** | 0.849 | *** | 1.046 | 0.712 | *** | 0.950 | ||
| <$30 K | 0.643 | *** | 1.174 | ** | 0.902 | ** | 1.017 | 0.803 | *** | 0.939 | ||
| <$50 K | 0.744 | *** | 1.061 | 0.939 | + | 1.054 | 0.789 | *** | 0.943 | |||
| <$75 K | 0.845 | * | 1.077 | 0.945 | 1.057 | 0.919 | * | 0.969 | ||||
| Unk. $ | 0.393 | *** | 1.018 | 0.765 | *** | 1.040 | 0.762 | *** | 0.739 | *** | ||
| 1th–8th | 0.284 | *** | 0.970 | 0.415 | *** | 1.016 | 0.685 | *** | 0.718 | *** | ||
| 9th–12th | 0.377 | *** | 0.992 | 0.507 | *** | 0.992 | 0.633 | *** | 0.702 | *** | ||
| 12th | 0.586 | *** | 1.148 | *** | 0.711 | *** | 0.982 | 0.807 | *** | 0.889 | *** | |
| 1–3 College | 0.864 | *** | 1.060 | + | 1.027 | 0.946 | 0.872 | *** | 1.036 | |||
| Unk. Ed. | 0.329 | *** | 1.413 | + | 0.577 | *** | 0.861 | 0.637 | ** | 0.512 | *** | |
| Self-Employed | 1.046 | 1.070 | 0.885 | ** | 1.059 | 0.872 | ** | 0.884 | * | |||
| No Work 1 yr.+ | 1.008 | 1.064 | 0.956 | 1.096 | 1.023 | 0.864 | * | |||||
| No Work <1 yr. | 1.204 | + | 1.279 | * | 1.124 | 0.940 | 1.036 | 1.066 | ||||
| Homemaker | 0.962 | 0.983 | 0.959 | 0.894 | 0.978 | 0.929 | ||||||
| Student | 1.293 | 1.051 | 1.070 | 1.060 | 1.084 | 1.020 | ||||||
| Retired | 1.058 | 1.154 | *** | 1.195 | *** | 0.964 | 1.240 | *** | 1.118 | *** | ||
| Cannot Work | 0.958 | 1.295 | *** | 1.158 | *** | 0.969 | 1.151 | *** | 1.156 | *** | ||
| Unk. Work | 0.913 | 0.798 | 1.077 | 0.875 | 1.061 | 1.074 | ||||||
| Very Good | 1.220 | * | 1.036 | 1.044 | 0.946 | 0.977 | 1.111 | |||||
| Good | 1.343 | *** | 1.290 | *** | 1.067 | 0.957 | 0.929 | 1.199 | ** | |||
| Fair | 1.305 | ** | 1.416 | *** | 1.086 | 0.941 | 0.877 | * | 1.218 | ** | ||
| Poor | 1.124 | 1.608 | *** | 1.125 | + | 0.913 | 0.827 | ** | 1.145 | * | ||
| Unk. Health | 0.542 | *** | 0.836 | 1.074 | 0.936 | 0.672 | * | 0.509 | *** | |||
| No Hlth Plan | 0.663 | *** | 0.784 | *** | 0.915 | * | 1.013 | 0.625 | *** | 0.828 | *** | |
| Unk. Hlth Plan | 0.479 | *** | 0.757 | 0.644 | ** | 1.231 | 1.075 | 0.932 | ||||
| No Doctor | 0.484 | *** | 0.646 | *** | 0.818 | *** | 0.927 | 0.770 | *** | 0.588 | *** | |
| Unk. Doctor | 0.512 | *** | 0.760 | + | 0.796 | 1.160 | 0.632 | ** | 0.677 | * | ||
| No Checkup | 0.369 | *** | 0.662 | *** | 0.895 | ** | 0.956 | 0.478 | *** | 0.463 | *** | |
| Unk. Checkup | 0.434 | *** | 0.538 | *** | 0.705 | *** | 1.145 | 0.626 | *** | 0.470 | *** | |
| Cost Affected | 0.831 | *** | 0.862 | *** | 1.013 | 0.924 | 0.719 | *** | 0.760 | *** | ||
| Unk. Cost | 0.559 | *** | 0.816 | 0.885 | 1.345 | 1.033 | 0.564 | ** | ||||
| Medicaid Expansion | 1.048 | *** | 0.971 | *** | 0.996 | 0.991 | 1.005 | 1.021 | *** |
| Variable | Effect Size |
|---|---|
| Blood Sugar | 0.020 |
| Doctor Visits | 0.001 |
| HbA1c Checks | 0.125 |
| Feet Checks | 0.042 |
| Diabetes Education | 0.033 |
| Eye Checks | 0.054 |
| Group | Blood Sugar | Doctor Visit | HbA1c Checks | Feet Checks | Education | Eye Exam |
|---|---|---|---|---|---|---|
| Demographics | 158,197 | 161,170 | 171,814 | 226,600 | 269,802 | 237,409 |
| SES | 158,199 | 161,273 | 164,780 | 225,991 | 265,841 | 237,076 |
| Health | 156,833 | 161,142 | 169,671 | 223,338 | 271,800 | 234,101 |
| Medicaid Expansion | 158,731 | 161,096 | 178,049 | 229,191 | 272,790 | 242,692 |
| Demographics + SES | 157,615 | 161,337 | 162,816 | 224,604 | 264,410 | 234,478 |
| SES + Health | 156,547 | 161,318 | 158,972 | 221,271 | 265,570 | 231,622 |
| Demographics + Health | 156,390 | 161,222 | 163,559 | 221,366 | 269,090 | 231,463 |
| Demographics + Medicaid Expansion | 158,148 | 161,172 | 171,410 | 226,472 | 269,799 | 237,341 |
| SES + Medicaid Expansion | 158,143 | 161,274 | 164,568 | 225,918 | 265,843 | 237,056 |
| Health + Medicaid Expansion | 156,752 | 161,165 | 167,452 | 223,195 | 271,241 | 232,153 |
| Demographics + SES + Health | 156,045 | 161,386 | 156,825 | 220,074 | 264,184 | 230,006 |
| Demographics + SES + Medicaid Expansion | 157,576 | 161,338 | 162,594 | 224,520 | 264,415 | 234,461 |
| Demographics + Health + Medicaid Expansion | 156,322 | 161,222 | 163,315 | 221,311 | 269,094 | 231,455 |
| SES + Health + Medicaid Expansion | 156,466 | 161,318 | 158,839 | 221,241 | 265,571 | 231,626 |
| Full Model | 155,986 | 161,387 | 156,684 | 220,033 | 264,189 | 230,010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulton, L.V.; Adepoju, O.E.; Dolezel, D.; Ekin, T.; Gibbs, D.; Hewitt, B.; McLeod, A.; Liaw, W.; Lieneck, C.; Ramamonjiarivelo, Z.; et al. Determinants of Diabetes Disease Management, 2011–2019. Healthcare 2021, 9, 944. https://doi.org/10.3390/healthcare9080944
Fulton LV, Adepoju OE, Dolezel D, Ekin T, Gibbs D, Hewitt B, McLeod A, Liaw W, Lieneck C, Ramamonjiarivelo Z, et al. Determinants of Diabetes Disease Management, 2011–2019. Healthcare. 2021; 9(8):944. https://doi.org/10.3390/healthcare9080944
Chicago/Turabian StyleFulton, Lawrence V., Omolola E. Adepoju, Diane Dolezel, Tahir Ekin, David Gibbs, Barbara Hewitt, Alexander McLeod, Winston Liaw, Cristian Lieneck, Zo Ramamonjiarivelo, and et al. 2021. "Determinants of Diabetes Disease Management, 2011–2019" Healthcare 9, no. 8: 944. https://doi.org/10.3390/healthcare9080944