
Factors That Impact the Adoption of Clinical Decision Support Systems (CDSS) for Antibiotic Management


Abstract
:1. Introduction
2. Materials and Methods
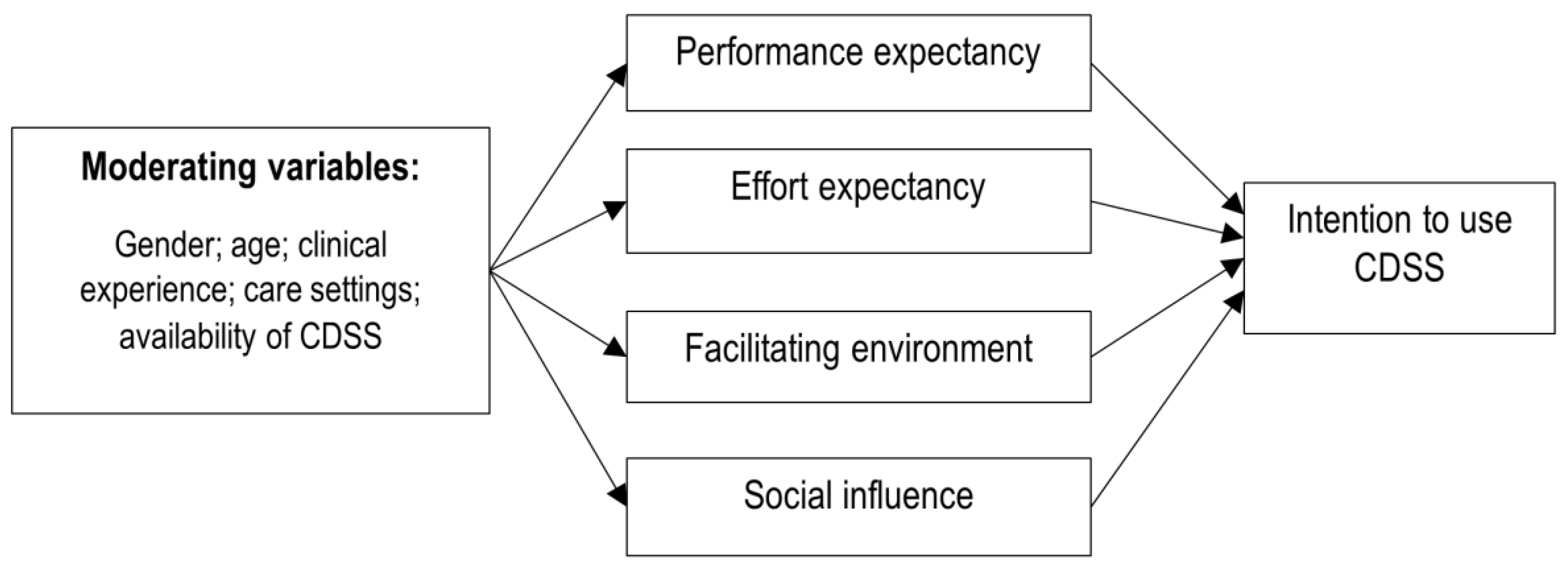
2.1. Theoretical Framework
2.2. Study Design
2.3. Study Participants
2.4. Questionnaire Instrument
2.5. Piloting
2.6. Measures
2.7. Statistical Analysis
2.8. Qualitative Analysis
2.9. Ethics Approval
3. Results
3.1. Characteristics of Study Participants
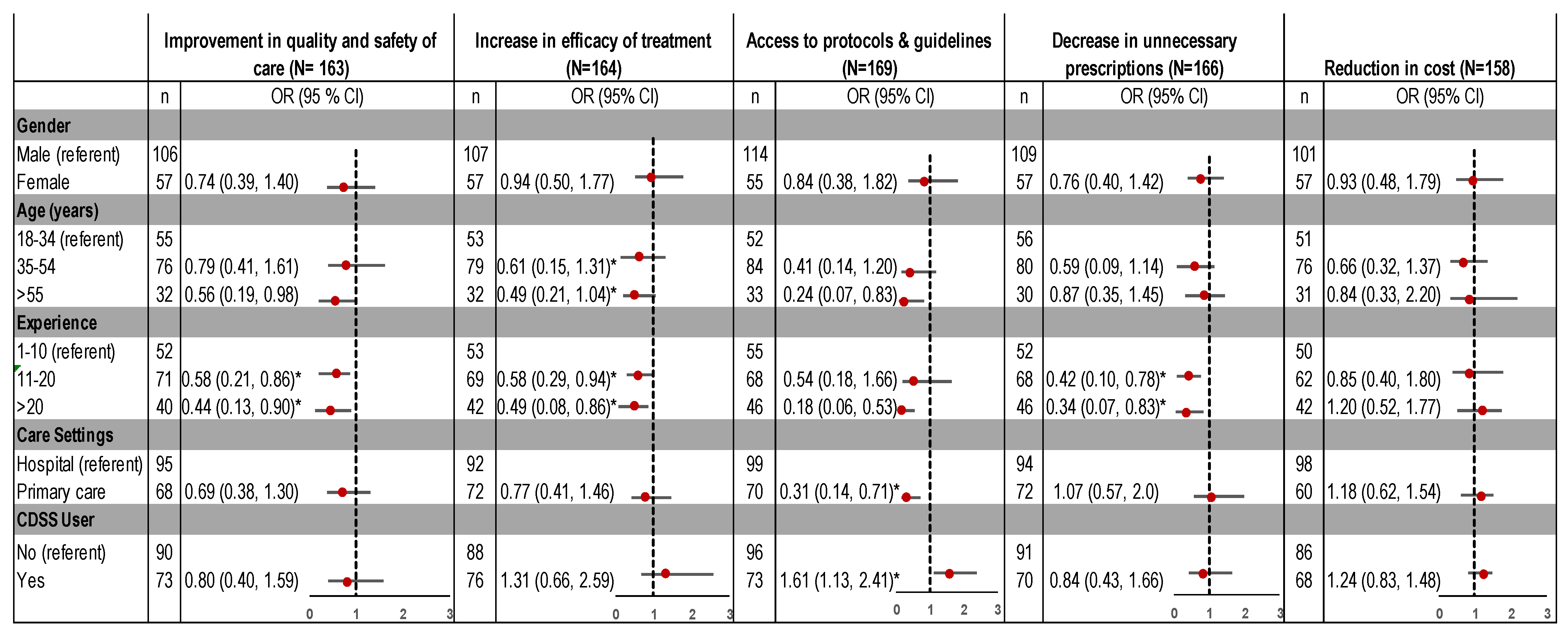
3.2. Perceived Benefit of CDSS
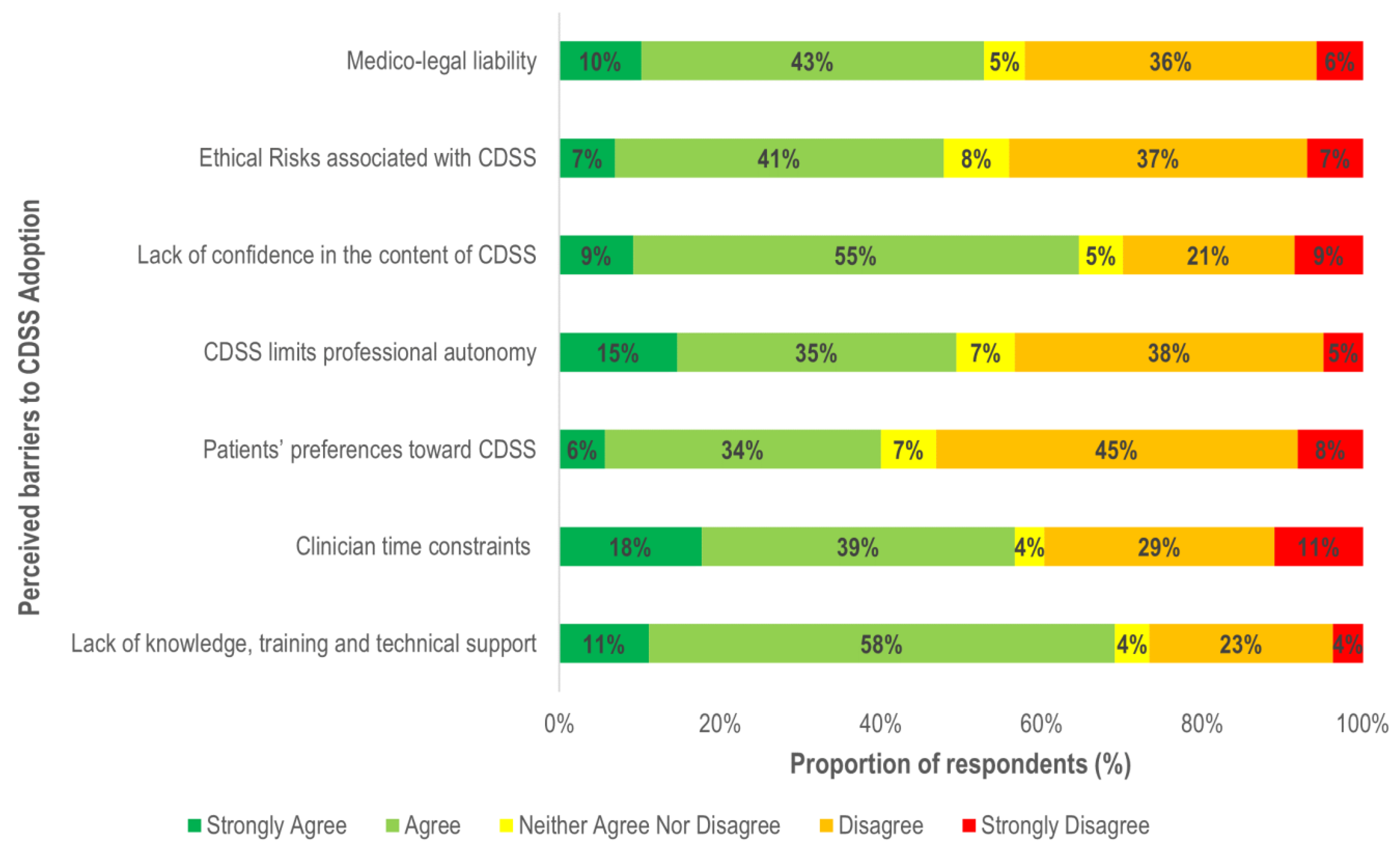
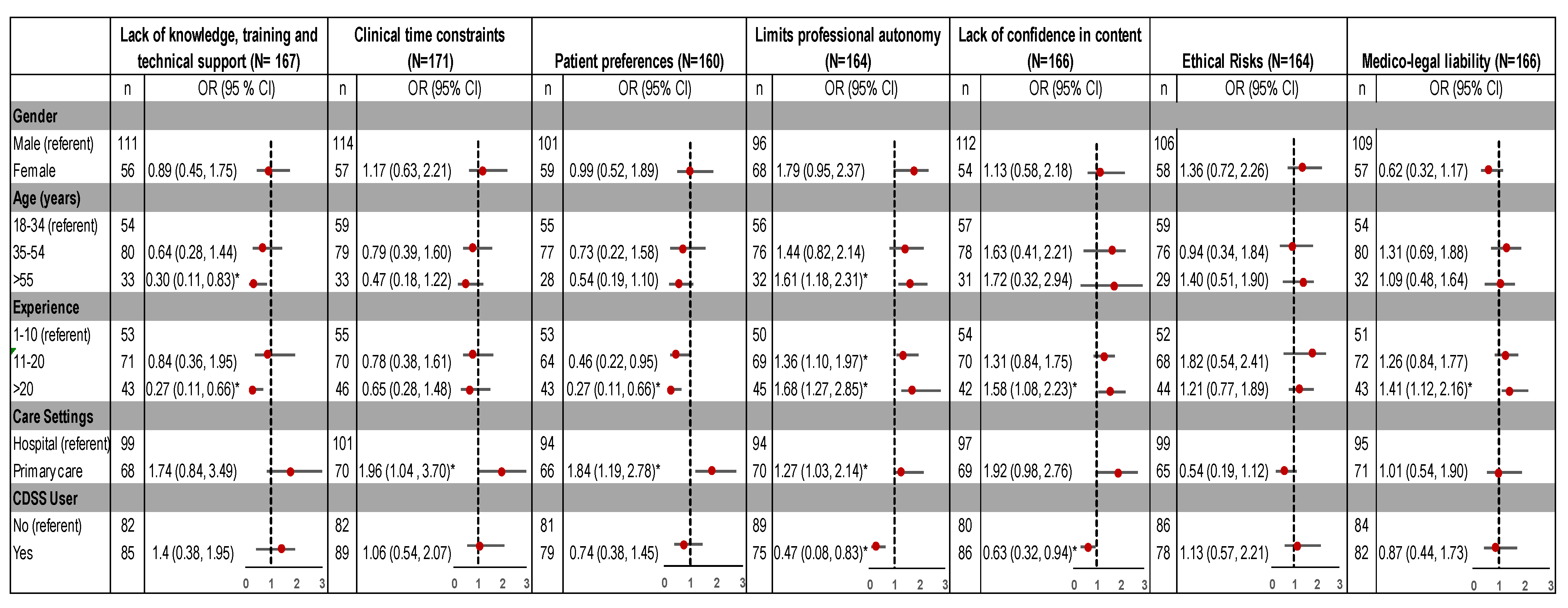
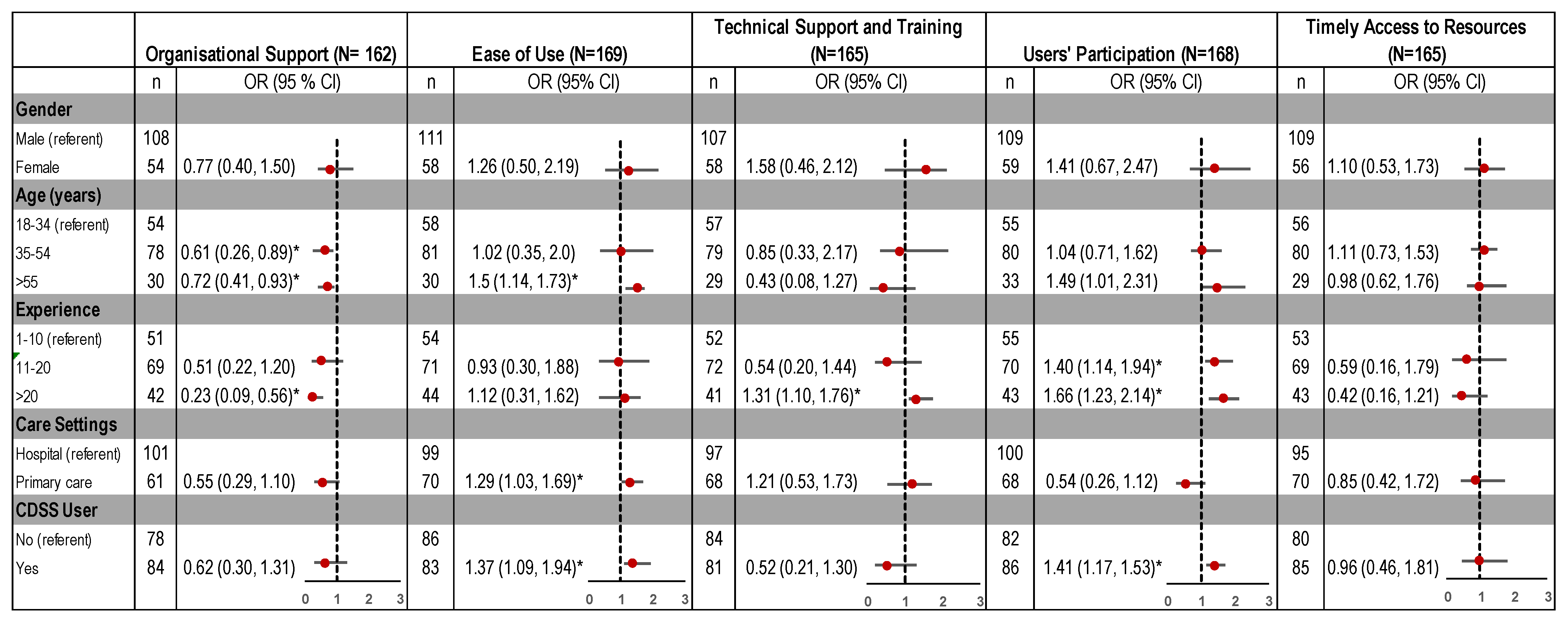
3.3. Perceived Barriers
3.4. Perceived Facilitators
3.5. Qualitative Analysis
- i.
- Lack of Flexibility
“Systems I have experienced are comically bad in design mainly because they are inflexible in their ability to change.”(Hospital)
“There is never a ‘one size fits all’. So there must always be room to make exceptions.”(Primary care)
- ii.
- Information Overload
“My major frustration with it [CDSS] in terms of antibiotic therapy is the presence of excessive alerts, which do nothing to protect patients and simply lead to alert fatigue.”(Hospital)
- iii.
- Information Accuracy
“I, as a user, need to know on what basis any recommendation is provided, what is the source of this knowledge and how often it is updated.”(Primary care)
“…[W]ithout knowing how often guidelines are updated in the system, we cannot rely on system alerts.”(Hospital)
4. Discussion
4.1. Barriers and Facilitators
4.1.1. External Factors
4.1.2. Internal Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sugden, R.; Kelly, R.; Davies, S. Combatting antimicrobial resistance globally. Nat. Microbiol. 2016, 1, 16187. [Google Scholar] [CrossRef]
- Flynn, H.W.; Batra, N.R.; Schwartz, S.G.; Grzybowski, A. Antibiotic stewardship. In Endophthalmitis in Clinical Practice; Springer International Publishing: Cham, Germany, 2018; pp. 171–173. [Google Scholar]
- Forrest, G.N.; Van Schooneveld, T.C.; Kullar, R.; Schulz, L.T.; Duong, P.; Postelnick, M. Use of electronic health records and clinical decision support systems for antimicrobial stewardship. Clin. Infect. Dis 2014, 59 (Suppl. 3), S122–S133. [Google Scholar] [CrossRef]
- Freundlich, R.E.; Wanderer, J.P.; Ehrenfeld, J.M. Clinical decision support tools need to improve more than just process outcomes. Anesthesiol. J. Am. Soc. Anesthesiol. 2018, 129, 614. [Google Scholar] [CrossRef]
- Jaspers, M.W.; Smeulers, M.; Vermeulen, H.; Peute, L.W. Effects of clinical decision-support systems on practitioner performance and patient outcomes: A synthesis of high-quality systematic review findings. J. Am. Med. Inform. Assoc. 2011, 18, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Curtis, C.E.; Al Bahar, F.; Marriott, J.F. The effectiveness of computerised decision support on antibiotic use in hospitals: A systematic review. PLoS ONE 2017, 12, e0183062. [Google Scholar] [CrossRef] [Green Version]
- Simões, A.; Maia, M.; Gregório, J.; Couto, I.; Asfeldt, A.; Simonsen, G.; Póvoa, P.; Viveiros, M.; Lapão, L. Participatory implementation of an antibiotic stewardship programme supported by an innovative surveillance and clinical decision-support system. J. Hosp. Infect. 2018, 100, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Laka, M.; Milazzo, A.; Merlin, T. Can evidence-based decision support tools transform antibiotic management? A systematic review and meta-analyses. J. Antimicrob. Chemother. 2020, 75, 1099–1111. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.L.; Lo, L.; Ferguson, J.; Goldberg, H.; Diaz-Martinez, J.P.; Tomlinson, G.; Grimshaw, J.M.; Shojania, K.G. Computerised clinical decision support systems and absolute improvements in care: Meta-analysis of controlled clinical trials. BMJ 2020, 370, m3216. [Google Scholar] [CrossRef] [PubMed]
- Holstiege, J.; Mathes, T.; Pieper, D. Effects of computer-aided clinical decision support systems in improving antibiotic prescribing by primary care providers: A systematic review. J. Am. Med. Inf. Assoc. 2015, 22, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Varonen, H.; Kortteisto, T.; Kaila, M.; for the EBMeDS Study Group. What may help or hinder the implementation of computerized decision support systems (cdsss): A focus group study with physicians. Fam. Pract. 2008, 25, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.L.; Ang, A.; Chow, C.Z.; Ng, T.M.; Teng, C.; Ling, L.M.; Ang, B.S.; Lye, D.C. Implementation hurdles of an interactive, integrated, point-of-care computerised decision support system for hospital antibiotic prescription. Int. J. Antimicrob. Agents 2016, 47, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Liberati, E.G.; Ruggiero, F.; Galuppo, L.; Gorli, M.; González-Lorenzo, M.; Maraldi, M.; Ruggieri, P.; Polo Friz, H.; Scaratti, G.; Kwag, K.H.; et al. What hinders the uptake of computerized decision support systems in hospitals? A qualitative study and framework for implementation. Implement. Sci. 2017, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Moxey, A.; Robertson, J.; Newby, D.; Hains, I.; Williamson, M.; Pearson, S.-A. Computerized clinical decision support for prescribing: Provision does not guarantee uptake. J. Am. Med. Inform. Assoc. 2010, 17, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Chung, P.; Scandlyn, J.; Dayan, P.S.; Mistry, R.D. Working at the intersection of context, culture, and technology: Provider perspectives on antimicrobial stewardship in the emergency department using electronic health record clinical decision support. Am. J. Infect. Control 2017, 45, 1198–1202. [Google Scholar] [CrossRef]
- Kortteisto, T.; Komulainen, J.; Mäkelä, M.; Kunnamo, I.; Kaila, M. Clinical decision support must be useful, functional is not enough: A qualitative study of computer-based clinical decision support in primary care. BMC Health Serv. Res. 2012, 12, 349. [Google Scholar] [CrossRef]
- Ozkaynak, M.; Wu, D.T.Y.; Hannah, K.; Dayan, P.S.; Mistry, R.D. Examining workflow in a pediatric emergency department to develop a clinical decision support for an antimicrobial stewardship program. Appl. Clin. Inform. 2018, 9, 248–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilsdonk, E.; Peute, L.W.; Jaspers, M.W.M. Factors influencing implementation success of guideline-based clinical decision support systems: A systematic review and gaps analysis. Int. J. Med. Inform. 2017, 98, 56–64. [Google Scholar] [CrossRef]
- Yusof, M.M.; Kuljis, J.; Papazafeiropoulou, A.; Stergioulas, L.K. An evaluation framework for health information systems: Human, organization and technology-fit factors (hot-fit). Int. J. Med. Inform. 2008, 77, 386–398. [Google Scholar] [CrossRef]
- Sutton, R.T.; Pincock, D.; Baumgart, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An overview of clinical decision support systems: Benefits, risks, and strategies for success. NPJ Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camacho, J.; Zanoletti-Mannello, M.; Landis-Lewis, Z.; Kane-Gill, S.L.; Boyce, R.D. A conceptual framework to study the implementation of clinical decision support systems (bear): Literature review and concept mapping. J. Med. Internet Res. 2020, 22, e18388. [Google Scholar] [CrossRef]
- Catho, G.; Centemero, N.S.; Catho, H.; Ranzani, A.; Balmelli, C.; Landelle, C.; Zanichelli, V.; Huttner, B.D. Factors determining the adherence to antimicrobial guidelines and the adoption of computerised decision support systems by physicians: A qualitative study in three european hospitals. Int. J. Med. Inf. 2020, 141, 104233. [Google Scholar] [CrossRef]
- Jung, S.Y.; Hwang, H.; Lee, K.; Lee, H.Y.; Kim, E.; Kim, M.; Cho, I.Y. Barriers and facilitators to implementation of medication decision support systems in electronic medical records: Mixed methods approach based on structural equation modeling and qualitative analysis. JMIR Med. Inf. 2020, 8, e18758. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Unified theory of acceptance and use of technology: A synthesis and the road ahead. J. Assoc. Inf. Syst. 2016, 17, 328–376. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Kelley, K.; Clark, B.; Brown, V.; Sitzia, J. Good practice in the conduct and reporting of survey research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulaziz, K.; Brehaut, J.; Taljaard, M.; Émond, M.; Sirois, M.-J.; Lee, J.S.; Wilding, L.; Perry, J.J. National survey of physicians to determine the effect of unconditional incentives on response rates of physician postal surveys. BMJ Open 2015, 5, e007166. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, C.T.; Quan, H.; Hemmelgarn, B.; Noseworthy, T.; Beck, C.A.; Dixon, E.; Samuel, S.; Ghali, W.A.; Sykes, L.L.; Jetté, N. Exploring physician specialist response rates to web-based surveys. BMC Med. Res. Methodol. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, T.; Scott, A. Do physicians prefer to complete online or mail surveys? Findings from a national longitudinal survey. Eval. Health Prof. 2019, 42, 41–70. [Google Scholar] [CrossRef] [PubMed]
- Broom, J.; Broom, A.; Plage, S.; Adams, K.; Post, J.J. Barriers to uptake of antimicrobial advice in a uk hospital: A qualitative study. J. Hosp. Infect. 2016, 93, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, S.; Sharma, S.K.; Fausto, D.J.; Viernes, S.; Kharrazi, H. Barriers and facilitators to clinical decision support systems adoption: A systematic review. J. Bus. Adm. Res. 2014, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Esmaeilzadeh, P.; Sambasivan, M.; Kumar, N.; Nezakati, H. Adoption of clinical decision support systems in a developing country: Antecedents and outcomes of physician’s threat to perceived professional autonomy. Int. J. Med. Inform. 2015, 84, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Goh, W.P.; Tao, X.; Zhang, J.; Yong, J. Decision support systems for adoption in dental clinics: A survey. Knowl. Based Syst. 2016, 104, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Rigopoulos, G.; Psarras, J.; Askounis, D. A tam model to evaluate user’s attitude towards adoption of decision support systems. J. Appl. Sci. 2008, 8, 899–902. [Google Scholar] [CrossRef]
- Short, D.; Frischer, M.; Bashford, J. Barriers to the adoption of computerised decision support systems in general practice consultations: A qualitative study of gps’ perspectives. Int. J. Med. Inform. 2004, 73, 357–362. [Google Scholar] [CrossRef]
- Zheng, K.; Padman, R.; Johnson, M.P.; Diamond, H.S. Understanding technology adoption in clinical care: Clinician adoption behavior of a point-of-care reminder system. Int. J. Med. Inform. 2005, 74, 535–543. [Google Scholar] [CrossRef]
- May, L.; Gudger, G.; Armstrong, P.; Brooks, G.; Hinds, P.; Bhat, R.; Moran, G.J.; Schwartz, L.; Cosgrove, S.E.; Klein, E.Y.; et al. Multisite exploration of clinical decision making for antibiotic use by emergency medicine providers using quantitative and qualitative methods. Infect. Control Hosp. Epidemiol. 2014, 35, 1114–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Lai, F.; Macmillan, J.; Daudelin, D.H.; Kent, D.M. The potential of training to increase acceptance and use of computerized decision support systems for medical diagnosis. Hum. Factors 2006, 48, 95–108. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Kern, J.; Marcee, A.; Grannemann, B.; Kleiber, B.; Bettinger, T.; Altshuler, K.; McClelland, A. Development and implementation of computerized clinical guidelines: Barriers and solutions. Methods Inf. Med. 2002, 41, 435–442. [Google Scholar] [CrossRef]
- Tsiknakis, M.; Kouroubali, A. Organizational factors affecting successful adoption of innovative ehealth services: A case study employing the fitt framework. Int. J. Med. Inf. 2009, 78, 39–52. [Google Scholar] [CrossRef]
- Chan, T.; Brew, S. Overcoming the barriers to using information systems. Nurs. Times 2004, 100, 44–46. [Google Scholar] [PubMed]
- Delone, W.H.; Mclean, E.R. Measuring e-commerce success: Applying the delone & mclean information systems success model. Int. J. Electron. Commer. 2004, 9, 31–47. [Google Scholar]
- Lugtenberg, M.; Pasveer, D.; van der Weijden, T.; Westert, G.P.; Kool, R.B. Exposure to and experiences with a computerized decision support intervention in primary care: Results from a process evaluation. BMC Fam. Pract. 2015, 16, 141. [Google Scholar] [CrossRef] [Green Version]
- Lugtenberg, M.; Weenink, J.-W.; van der Weijden, T.; Westert, G.P.; Kool, R.B. Implementation of multiple-domain covering computerized decision support systems in primary care: A focus group study on perceived barriers. BMC Med. Inform. Decis. Mak. 2015, 15, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, D.; Frischer, M.; Bashford, J. The development and evaluation of a computerised decision support system for primary care based upon ‘patient profile decision analysis’. J. Innov. Health Inform. 2003, 11, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Khairat, S.; Marc, D.; Crosby, W.; Al Sanousi, A. Reasons for physicians not adopting clinical decision support systems: Critical analysis. JMIR Med. Inf. 2018, 6, e24. [Google Scholar] [CrossRef]
- Shibl, R.; Lawley, M.; Debuse, J. Factors influencing decision support system acceptance. Decis. Support Syst. 2013, 54, 953–961. [Google Scholar] [CrossRef]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.A.; Rubin, H.R. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999, 282, 1458–1465. [Google Scholar] [CrossRef] [PubMed]
- Goud, R.; van Engen-Verheul, M.; de Keizer, N.F.; Bal, R.; Hasman, A.; Hellemans, I.M.; Peek, N. The effect of computerized decision support on barriers to guideline implementation: A qualitative study in outpatient cardiac rehabilitation. Int. J. Med. Inform. 2010, 79, 430–437. [Google Scholar] [CrossRef]
- Leslie, S.J.; Hartswood, M.; Meurig, C.; McKee, S.P.; Slack, R.; Procter, R.; Denvir, M.A. Clinical decision support software for management of chronic heart failure: Development and evaluation. Comput. Biol. Med. 2006, 36, 495–506. [Google Scholar] [CrossRef]
- Belard, A.; Buchman, T.; Forsberg, J.; Potter, B.K.; Dente, C.J.; Kirk, A.; Elster, E. Precision diagnosis: A view of the clinical decision support systems (cdss) landscape through the lens of critical care. J. Clin. Monit. Comput. 2017, 31, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Hor, C.P.; O’Donnell, J.M.; Murphy, A.W.; O’Brien, T.; Kropmans, T.J.B. General practitioners’ attitudes and preparedness towards clinical decision support in e-prescribing (cds-ep) adoption in the west of ireland: A cross sectional study. BMC Med. Inform. Decis. Mak. 2010, 10, 2. [Google Scholar] [CrossRef]
- Afonso, C.M.; Roldán Salgueiro, J.L.; Sánchez Franco, M.J.; González, M.d.l.O. The moderator role of gender in the unified theory of acceptance and use of technology (utaut): A study on users of electronic document management systems. In Proceedings of the 7th International Conference on Partial Least Squares and Related Methods, Houston, TX, USA, 19–22 May 2012. [Google Scholar]
- Zuiderwijk, A.; Janssen, M.; Dwivedi, Y.K. Acceptance and use predictors of open data technologies: Drawing upon the unified theory of acceptance and use of technology. Gov. Inf. Q. 2015, 32, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Bandyopadhyay, K.; Barnes, C. An analysis of factors affecting user acceptance of erp systems in the united states. Int. J. Hum. Cap. Inf. Technol. Prof. (IJHCITP) 2012, 3, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.I.; Johnson, T.P.; VanGeest, J.B. Enhancing surveys of health care professionals: A meta-analysis of techniques to improve response. Eval. Health Prof. 2013, 36, 382–407. [Google Scholar] [CrossRef] [PubMed]
- Joyce, C.M.; Scott, A.; Jeon, S.-H.; Humphreys, J.; Kalb, G.; Witt, J.; Leahy, A. The “medicine in australia: Balancing employment and life (mabel)” longitudinal survey-protocol and baseline data for a prospective cohort study of australian doctors’ workforce participation. BMC Health Serv. Res. 2010, 10, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 180 (%) | |
|---|---|---|
| Gender | ||
| Male | 118 (66) | |
| Female | 62 (34) | |
| Age-Group | ||
| 18–34 years | 61 (34) | |
| 35–54 years | 84 (47) | |
| 55 years and over | 35 (19) | |
| Years of Experience | ||
| 1–10 years | 57 (32) | |
| 11–20 years | 75 (42) | |
| More than 20 years | 48 (27) | |
| Care setting and Type of Practice * | ||
| Hospital(s) | Public | 44 (24) |
| Private | 14 (8) | |
| Mixed | 35 (19) | |
| Total | 93 (51) | |
| Primary care | Private | 15 (8) |
| Community clinic | 11 (6) | |
| Hospital-based clinic | 12 (7) | |
| Mixed | 25 (14) | |
| Total | 63 (35) | |
| State and Territory, Australia (n = 139) * | ||
| Eastern (ACT/NSW/QLD/TAS/VIC) | 101 (73) | |
| Central (SA/NT) | 21 (15) | |
| Western (WA) | 17 (12) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laka, M.; Milazzo, A.; Merlin, T. Factors That Impact the Adoption of Clinical Decision Support Systems (CDSS) for Antibiotic Management. Int. J. Environ. Res. Public Health 2021, 18, 1901. https://doi.org/10.3390/ijerph18041901
Laka M, Milazzo A, Merlin T. Factors That Impact the Adoption of Clinical Decision Support Systems (CDSS) for Antibiotic Management. International Journal of Environmental Research and Public Health. 2021; 18(4):1901. https://doi.org/10.3390/ijerph18041901
Chicago/Turabian StyleLaka, Mah, Adriana Milazzo, and Tracy Merlin. 2021. "Factors That Impact the Adoption of Clinical Decision Support Systems (CDSS) for Antibiotic Management" International Journal of Environmental Research and Public Health 18, no. 4: 1901. https://doi.org/10.3390/ijerph18041901