Excluding venous thromboembolism using point of care D-dimer tests in outpatients: a diagnostic meta-analysis
BMJ 2009; 339 doi: https://doi.org/10.1136/bmj.b2990 (Published 14 August 2009) Cite this as: BMJ 2009;339:b2990
- G J Geersing, general practitioner 1,
- K J M Janssen, clinical epidemiologist1,
- R Oudega, general practitioner1,
- L Bax, clinical epidemiologist 12,
- A W Hoes, professor of clinical epidemiology and primary care1,
- J B Reitsma, clinical epidemiologist3,
- K G M Moons, professor of clinical epidemiology 1
- 1Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, Netherlands
- 2Kitasato Clinical Research Center, Kitasato University, Japan
- 3Department of Clinical Epidemiology and Biostatistics, Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands
- Correspondence to: G J Geersing g.j.geersing{at}umcutrecht.nl
- Accepted 28 April 2009
Abstract
Objective To review the evidence on the diagnostic accuracy of the currently available point of care D-dimer tests for excluding venous thromboembolism.
Design Systematic review of research on the accuracy of point of care D-dimer tests, using bivariate regression to examine sources of variation and to estimate sensitivity and specificity.
Data sources Studies on the diagnostic accuracy of point of care D-dimer tests published between January 1995 and September 2008 and available in either Medline or Embase.
Review methods The analysis included studies that compared point of care D-dimer tests with predefined reference criteria for venous thromboembolism, enrolled consecutive outpatients, and allowed for construction of a 2×2 table.
Results 23 studies (total number of patients 13 959, range in mean age 38-65 years, range of venous thromboembolism prevalence 4-51%) were included in the meta-analysis. The studies reported two qualitative point of care D-dimer tests (SimpliRED D-dimer (n=12) and Clearview Simplify D-dimer (n=7)) and two quantitative point of care D-dimer tests (Cardiac D-dimer (n=4) and Triage D-dimer (n=2)). Overall sensitivity ranged from 0.85 (95% confidence interval 0.78 to 0.90) to 0.96 (0.91 to 0.98) and overall specificity from 0.48 (0.33 to 0.62) to 0.74 (0.69 to 0.78). The two quantitative tests Cardiac D-dimer and Triage D-dimer scored most favourably.
Conclusions In outpatients suspected of venous thromboembolism, point of care D-dimer tests can contribute important information and guide patient management, notably in low risk patients (that is, those patients with a low score on a clinical decision rule).
Introduction
Diagnosing patients suspected of venous thromboembolism—that is, deep venous thrombosis (DVT) or pulmonary embolism (PE)—is a major challenge because the signs and symptoms are often mild and non-specific.1 2 Primary care physicians in particular, who in many countries are faced with the initial presentation of venous thromboembolism and have to decide whether to refer patients for subsequent testing or not, can have difficulty diagnosing venous thromboembolism.
D-dimer testing can be used to improve the cost effectiveness of the diagnostic process. D-dimers are degradation products of cross linked fibrin that are generated during fibrinolysis, and circulating levels are typically elevated in patients with venous thromboembolism. A negative result in a D-dimer test in combination with a low pre-test probability of venous thromboembolism (as assessed by a validated clinical decision rule) can safely rule out DVT as well as PE.3 4 5 6 A large variety of laboratory D-dimer tests are currently available and their accuracy has been described extensively.7 8
Recently, various point of care or “near patient” D-dimer tests have been introduced. These D-dimer tests can be performed during the consultation of a patient and results are already available within 10-15 minutes. Using these tests could avoid the need for more labour intensive and time consuming laboratory D-dimer testing. This advantage is especially useful for primary care physicians, as they often have to decide on further patient management during the consultation of a patient with suspected venous thromboembolism. In this setting, referral for conventional laboratory D-dimer testing could be either impractical owing to limited access to central laboratories or time consuming for both patient and doctor. Furthermore, venous thromboembolism is confirmed by subsequent imaging tests in only 10-20% of all referred patients.6 Application of point of care D-dimer tests could, therefore, be cost effective not only in primary care patients suspected of venous thromboembolism but also in secondary care outpatients, notably those presenting at emergency departments. Another advantage in this setting is that a test result can be obtained more rapidly than when using conventional laboratory testing.
Two systematic reviews concluded that a low clinical probability (as assessed by the clinical decision rule developed by Wells et al6) and a negative result on SimpliRED D-dimer (a point of care assay; Agen Biomedical, Brisbane, Australia) could safely exclude venous thromboembolism.9 10 There has nevertheless been much discussion about the diagnostic accuracy and applicability of this semiqualitative point of care D-dimer test, mainly because of the low interobserver agreement associated with this assay.11 12 Perhaps as a consequence, several new point of care D-dimer tests have been introduced in recent years. Such tests have never been subject to a formal (diagnostic) meta-analysis because studies on their diagnostic performance were not available at the time of the two latest systematic reviews.9 10 Before these new point of care tests are widely implemented in daily practice, however, their diagnostic performance has to be thoroughly evaluated. We conducted a diagnostic meta-analysis to assess the accuracy of all currently available point of care D-dimer tests, with particular focus on their ability to exclude either DVT or PE in suspected outpatients.
Methods
Data sources and searches
We performed a systematic search of two online databases to identify studies evaluating the diagnostic accuracy of point of care D-dimer tests for the exclusion of DVT and PE. Sources were articles in Medline and Embase published between 1995 and 1 September 2008. The search strategy included (“fibrin fibrinogen degradation products” OR “D-dimer” ) combined with (“venous thrombosis” OR “pulmonary embolism”. We restricted our search to studies published in English only. Duplicate articles identified in both Medline and Embase were manually deleted using Reference Manager, version 11 (Thomson Reuters, Philadelphia, PA, USA). The reference lists of identified studies were checked for further relevant studies, and experts in the field recommended further articles to complement the electronic searches.
Point of care D-dimer tests under study
D-dimers are degradation products of cross linked fibrin generated during fibrinolysis. D-dimer, however, is not a single entity in plasma but a mixture of heterogeneous fibrin degradation products. Different assays measure different types of D-dimer; consequently, test results are reported as μg/ml D-dimer units (D-DU), μg/ml fibrinogen equivalent units (FEU), or ng/ml. No single cut off value for all assays exists, and attempts to standardise D-dimer testing have failed.13 Hence, any D-dimer test can only be correctly validated against a reference standard for venous thromboembolism (for example, compression ultrasonography for DVT). We included four different point of care D-dimer tests in our meta-analysis: two qualitative tests and two quantitative tests.
SimpliRED D-dimer
SimpliRED D-dimer is a semiqualitative test performed by mixing capillary or venous blood with a drop of test reagent in the test well. A positive result is defined as any visible agglutination within two minutes. Visible agglutination will occur if D-dimer levels exceed 200 μg/l.
Clearview Simplify D-dimer
Clearview Simplify D-dimer (Inverness Medical, Bedford, UK) is a qualitative test and is performed by mixing 35 μl of capillary or venous blood with two drops of test reagent. A positive test result occurs when D-dimer levels exceed 80 ng/ml and is indicated by a visible pink-purple coloured line that forms at the test zone. Test results are valid if a pink-purple line is also present at the control zone. The test can be read within 10 minutes.
Cardiac D-dimer
Cardiac D-dimer (Roche Diagnostics, Mannheim, Germany) is performed with 150 μl whole venous blood and a small portable instrument (Cobas h 232; Roche Diagnostics). The instrument displays a quantitative result within a range of 0.1-4.0 μg/ml FEU. A threshold value of 0.5 μg/ml FEU is used, above which a test result is called positive. Test results are available within 10-15 minutes.
Triage D-dimer
Triage D-dimer (Biosite, San Diego, CA, USA) is performed with 250 μl of whole blood treated with EDTA and a small portable instrument (Triage Meter Plus; Biosite). The Triage Meter Plus displays a quantitative result within a range of 0.1-5 μg/ml D-DU, using a cut off value of 0.35 μg/ml D-DU. Test results are available within 10-15 minutes.
Study selection
To be eligible for inclusion, the studies had to fulfil the following criteria:
1) Have a study population of consecutive outpatients (age >18 years) in primary or secondary care who were clinically suspected of DVT (proximal or distal) and/or PE
2) Assess a point of care D-dimer test; that is, a test that is performed in a near patient situation in the emergency department or at the physician’s office and not on a routine laboratory machine
3) Use compression ultrasonography, venography, impedance plethysmography, or uneventful follow-up (that is, no DVT or PE in at least three months, an accepted reference standard in this field of research6)as a reference test for DVT
4) Use computerised tomography pulmonary angiography, ventilation-perfusion lung scanning, pulmonary angiography, or uneventful follow-up as a reference test for PE
5) Include calculation of sensitivity, specificity, negative and positive predictive values, and prevalence of DVT or PE.
Data extraction
Two reviewers (GJG and KJMJ) independently extracted the following characteristics from each study: prevalence of DVT and PE; percentage males; percentage of patients with an active malignancy; percentage of patients with recent surgery (<4 weeks); and mean age of the patients. If the study addressed DVT, the percentage of patients with a distal (calf) vein thrombosis and the percentage of patients with a previous DVT were also extracted. Finally, the number of true positives, false positives, true negatives, and false negatives for the index test were extracted from the studies and a 2×2 table was constructed. Discrepancies were resolved by discussion between the two reviewers and if agreement could not be reached, a third or fourth reviewer was consulted (RO and KGMM). Authors of the respective studies were contacted to provide further details in cases where information was missing from the articles.
Quality assessment
The methodological quality of the selected studies was graded independently by two reviewers (GJG and KJMJ) with the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool, a validated tool for the quality assessment of diagnostic accuracy studies.14 In case of doubt, a third and fourth reviewer (RO and KGMM) were consulted.
Data synthesis and analysis
We used the bivariate model for diagnostic meta-analysis to obtain an overall sensitivity and an overall specificity.15 Instead of using the diagnostic odds ratio, as used in conventional diagnostic meta-analytical methods,16 the bivariate approach uses pairs of sensitivity and specificity as the starting point of the analysis. Besides accounting for study size, the bivariate model estimates and incorporates the negative correlation that may arise between the sensitivity and specificity of the index test within studies as a result of differences in test positive/negative threshold between studies. These threshold differences are particularly important for the qualitative point of care D-dimer tests, as the threshold underlying a positive result in such tests is unknown or implicit. The bivariate model uses a random effects approach for both sensitivity and specificity, which allows for heterogeneity beyond chance as a result of clinical and methodological differences between studies. To examine sources of heterogeneity, different study characteristics were added to the model as covariates. For reasons of statistical power, we performed such a meta-regression analysis for only point of care D-dimer tests assessed in at least 10 studies. For the remaining tests, we simply performed a subgroup analysis across relevant subgroups of the covariate. Evidence for publication bias through small study effects was explored with a regression test on the diagnostic odds ratio.17
We defined a priori the following clinical and design characteristics of a study as potential relevant covariates: type of venous thromboembolism (DVT or PE); proportion of patients with a proximal DVT (for DVT studies only); proportion of patients with a recurrent DVT (for DVT studies only); proportion of patients with an active malignancy; and proportion of patients with recent surgery (<4 weeks). The QUADAS tool criteria, in particular differential verification and incorporation bias, were also examined as potential sources of bias.
To graphically present the results, we plotted the individual and summary points of sensitivity and specificity in a receiver operating characteristic graph, plotting the index test’s sensitivity (true positive rate) on the y axis against 1-specificity (false negative rate) on the x axis. In addition, we plotted the 95% confidence region and a 95% prediction region around the pooled estimates to illustrate the precision with which the pooled values were estimated (confidence ellipse of a mean) and to show the amount of between study variation (prediction ellipse; the likely range of values for a new study).
Finally, we estimated the predictive value of the point of care D-dimer tests. Given that D-dimer testing is predominately used to exclude venous thromboembolism, the post-test probability of a negative D-dimer test—that is, the negative predictive value—is of highest importance. As the incidence of venous thromboembolism following normal results from imaging tests is around 2% for patients suspected of DVT,6 a post-test probability of 2% or less would be accepted as safe. According to Bayes’ theorem, the post-test probability of a negative test can be calculated using the negative likelihood ratio; that is, the pre-test odds multiplied by the likelihood ratio of a negative test result (LR-), where pre-test odds is calculated by dividing pre-test probability by (1-pre-test probability) and the post-test probability comprises post-test odds divided by (1+post-test odds).18 The pooled estimates of sensitivity and specificity were used to calculate the average LR- by dividing (1-sensitivity) over specificity. Subsequently, we estimated the negative predictive value of the different point of care D-dimer tests for three different clinically relevant prevalences of venous thromboembolism:6 19 5% prevalence (low risk patients); 20% prevalence (moderate risk patients); and 50% prevalence (high risk patients). Where appropriate, 95% confidence intervals were calculated.
We used STATA version 10.0 (StataCorp, College Station, TX, USA), in particular the midas and metandi commands, for all statistical analyses.20 21
Results
Identification of studies and study quality
Our search yielded 2022 citations (fig 1⇓), 203 of which were retrieved for full text review. Of these, 180 articles were excluded, mainly because the particular D-dimer test examined was not a point of care assay. A total of 23 citations were included in the final analysis. The 23 studies included a large management study (1002 patients suspected of DVT) that has recently been accepted for publication and a recently conducted study on the accuracy of different point of care D-dimer tests.w1 w2 The final analysis included 12 studies evaluating SimpliRED D-dimer,w3-w14 seven looking at Clearview Simplify D-dimer,w1 w2 w15-w19 four examining Cardiac D-dimer,w2 w20-w22 and two assessing Triage D-dimer.w2 w23

Fig 1 Flowchart of included studies. *Instead an aetiological study; for example, a study on risk factors for venous thromboembolism or number of ventilation-perfusion lung scans ordered as a function of D-dimer testing. †Studies investigating other biomarkers, such as P-selectin, or other tests, such as electrocardiography. ‡Studies that did not use venous thromboembolism as the outcome, but aortic dissection or mesenterial thrombosis, for example. §156 of 203 studies were found in both Embase and Medline. ¶For example, because D-dimer testing was only performed in patients with a positive ultrasonogram. **One study compared three different point of care D-dimer tests. Abbreviations: POC, point of care; VTE, venous thromboembolism
{kind=link}
In total, we included 6796 patients tested with SimpliRED D-dimer, 5730 patients tested with Clearview Simplify D-dimer, 925 patients tested with Cardiac D-dimer, and 508 patients tested with Triage D-dimer, of which 1272/6796 (18.7%), 470/5730 (8.2%), 317/925 (33.9%), and 67/508 (13.2%) were diagnosed with venous thromboembolism, respectively. Mean age of included patients varied across studies from 38 years to 65 years, and percentage males ranged from 30% to 55%.
Overall, the quality of the included studies was good (fig 2⇓). All studies used a prospective study design and enrolled consecutive outpatients suspected of venous thromboembolism. Among the possible sources of bias in diagnostic accuracy studies, differential verification and incorporation bias were present most often at 30% and 31%, respectively. Also, blinding of index and reference test results was poorly reported, as was the presence of uninterpretable test results.

Fig 2 Proportion of all 14 Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool criteria that were fulfilled
{kind=link}
Study and population characteristics
Of the 12 SimpliRED D-dimer studies, eight evaluated patients suspected of DVT, three studied patients suspected of PE, and one studied both types of patient (table 1⇓). Of the seven Clearview Simplify D-dimer studies, four assessed patients suspected of DVT and three evaluated patients suspected of PE, whereas one of the two Triage D-dimer studies included patients suspected of DVT or PE and the other only patients suspected of DVT. All four Cardiac D-dimer studies focused on DVT only. Table 1 lists the other study and population characteristics of all 25 patient populations.
Population and study characteristics of included studies
Diagnostic accuracy indices of point of care D-dimer tests
Overall analysis
The pooled sensitivity and specificity of all studies combined was 0.88 (95% confidence interval 0.83 to 0.92) and 0.70 (0.62 to 0.77), respectively. As anticipated, the between study variability beyond what could be expected by sampling error was substantial, with an I2 of 80% for the sensitivity results and 96% for the specificity results. Analysis of small study effects, potentially a result of publication bias, yielded no significant evidence for such effects (P=0.23).
Per-test analyses
The pooled sensitivity (based on the bivariate model) of SimpliRED, Clearview Simplify, and Cardiac D-dimer was 0.85 (95% confidence interval 0.78 to 0.90), 0.87 (0.81 to 0.91), and 0.96 (0.91 to 0.98), respectively (fig 3, table 2⇓ ⇓); the overall specificity was 0.74 (0.69 to 0.78), 0.62 (0.54 to 0.69), and 0.57 (0.52 to 0.62), respectively. As only two studies evaluated Triage D-dimer, an overall sensitivity and specificity could not be calculated using the bivariate approach. The traditional sample size weighted approach yielded an average sensitivity of 0.93 (0.88 to 0.97) and specificity of 0.48 (0.33 to 0.62).16

Fig 3 Receiver operating characteristic graphs with 95% confidence region and 95% prediction region for SimpliRED, Clearview Simplify, and Cardiac D-dimer. The pooled sensitivity of SimpliRED, Clearview Simplify, and Cardiac D-dimer was 0.85, 0.87, and 0.96, respectively; pooled specificity was 0.74, 0.62, and 0.57, respectively. Pooled sensitivity and specificity could not be calculated using the bivariate model for Triage D-dimer owing to the small number of studies assessing this test; the traditional sample size weighted approach yielded an average sensitivity of 0.93 and specificity of 0.48.16 Abbreviation: HSROC, hierarchical summary receiver operating characteristic
{kind=link}
Overall and covariate analysis for point of care D-dimer tests
Covariate analysis
Results from the covariate analysis are presented in table 2. Both the sensitivity and specificity of SimpliRED D-dimer and Clearview Simplify D-dimer did not vary across covariates and were essentially the same as in the overall analysis (table 2).
Negative predictive value
Table 3⇓ shows to what extent the different point of care D-dimer assays changed the post-test probability of venous thromboembolism—that is, the incidence of venous thromboembolism following normal results from a point of care D-dimer test —for different clinically relevant pre-test probabilities. For example, if the prevalence of venous thromboembolism is high (50%) in a suspected population, a negative Clearview Simplify D-dimer test yields a post-test probability of 18%. If, however, venous thromboembolism prevalence in the population is low (5%), a negative Clearview Simplify D-dimer test reduces this prevalence to a post-test probability of 1.1%. Figure 4⇓ can be used to estimate post-test probabilities for other pre-test probabilities.

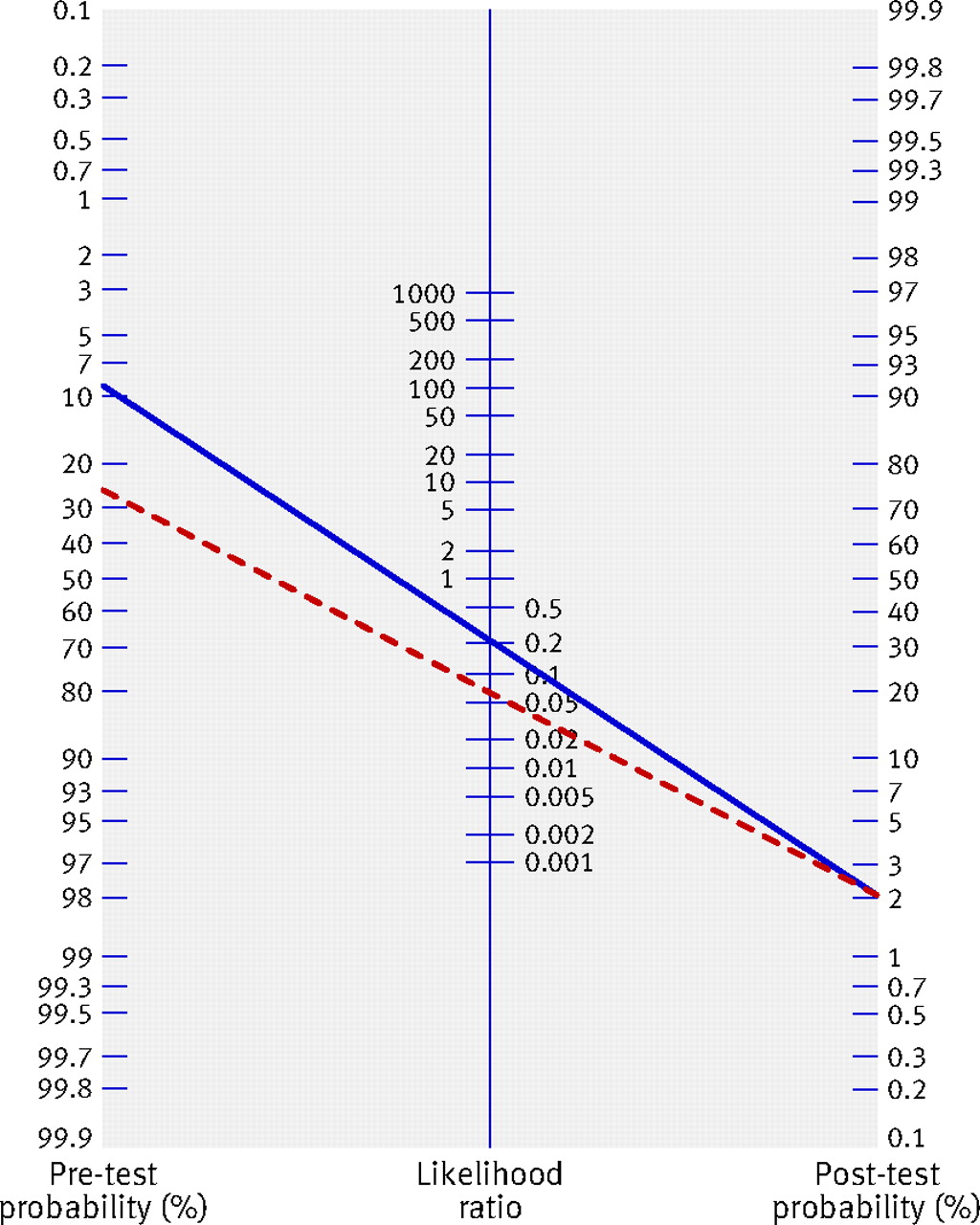
Fig 4 Fagan’s nomogram for Cardiac D-dimer (dashed red line) and Clearview Simplify D-dimer (solid blue line), with a fixed post-test probability of 2%. If post-test probability is fixed at the accepted safety standard of 2%, Cardiac D-dimer can exclude venous thromboembolism in patients with a pre-test probability of up to 27%, compared with 9% with Clearview Simplify D-dimer. For other pre-test probabilities, the post-test probability can be calculated by simply drawing a line through the negative likelihood ratio of the respective point of care D-dimer test (see table 3) and the chosen pre-test probability
{kind=link}
Analysis of the negative predictive value of point of care D-dimer tests for patients at low, moderate, and high risk of VTE
Discussion
This is the first meta-analysis of studies on the currently available point of care D-dimer tests. Measuring D-dimer levels is an important step in the diagnostic investigation of patients suspected of venous thromboembolism. A negative D-dimer test result in combination with a low pre-test probability of venous thromboembolism is widely used to exclude the diagnosis and thus safely reduce the number of unnecessary referrals for imaging.10 A meta-analysis performed by Fancher et al in 2004 concluded that a negative result on SimpliRED D-dimer could exclude venous thromboembolism in low risk patients9; however, after 2004 various newer point of care D-dimer tests (qualitative as well as quantitative) have become available. We summarised the literature on the diagnostic accuracy of these point of care assays, including the older SimpliRED D-dimer. Our meta-analysis shows that the qualitative assays (SimpliRED D-dimer and Clearview Simplify D-dimer) have a lower sensitivity (that is, a higher number of false negatives) but higher specificity (that is, a lower number of false positives) than the quantitative assays (Cardiac D-dimer and Triage D-dimer). The latter seem, therefore, better suited to rule out DVT in suspected patients: they decrease the pre-test probability of venous thromboembolism more effectively. In this regard, Cardiac D-dimer outperforms Triage D-dimer, as it is able to rule out DVT both in patients with a low pre-test risk and in those with a moderate pre-test risk.
Strengths and limitations
Some methodological issues need to be considered. Firstly, we found substantial heterogeneity across the SimpliRED D-dimer studies. This variation could not be corrected for or explained by adding covariates in the bivariate meta-regression model. In the summary receiver operating characteristic graph, all but three of the 12 ‘sensitivity - (1-specificity)’ combinations of the individual SimpliRED D-dimer studies lie on or near the receiver operating characteristic curve; therefore, studies with a higher sensitivity have a lower specificity and vice versa. This pattern is commonly attributed to differences in the threshold for test positivity used in the different studies.16 Indeed, the heterogeneity across the SimpliRED studies could well be explained by threshold differences, as defining a positive test result for this point of care D-dimer test is subjective and depends on the amount of visible agglutination seen. This assessment may have low interobserver agreement and, therefore, different thresholds for test positivity.11 12 Threshold differences across diagnostic studies are implicit, so they cannot be accounted for in the analysis. Hence, calculating a common underlying sensitivity and specificity of SimpliRED D-dimer might not be possible with the currently available data. The use of quantitative point of care assays and further standardising the interpretation of qualitative point of care tests will surely reduce this problem.
Secondly, most of the studies in our review included patients suspected of DVT. Only six studies evaluated patients suspected of PE. In patients with PE, there is a strong correlation between embolus location and D-dimer levels. Small sub-segmental thrombi result in less D-dimer formation, so D-dimer tests have lower sensitivity in patients suspected of PE.22 Indeed, the two of the three Clearview Simplify D-dimer studies that included patients suspected of PE had lower sensitivity than the studies that only included patients suspected of DVT.w15 w16 No studies on the diagnostic accuracy of the Cardiac D-dimer for patients suspected of PE were available; therefore, our results for patients suspected of PE should be interpreted with more caution than those relating to patients with DVT.
Thirdly, different studies used different reference standards to diagnose or exclude venous thromboembolism. As with many reference standards, none was a 24 carat gold standard. For example, compression ultrasonography is used as the reference standard in most DVT studies. A meta-analysis by Goodacre et al found a pooled sensitivity of compression ultrasonography for detection of proximal DVT of 0.94, compared with venography as reference standard.23 This finding implies that even compression ultrasonography might miss a small proportion of DVT cases. Given that most of the DVT studies in our analysis used compression ultrasonography as the reference standard, the reported pooled sensitivity of the point of care D-dimer tests could thus be slightly overestimated. Compression ultrasonography is now the accepted reference standard in daily clinical practice, however, and the use of a reference standard with a higher sensitivity—such as venography—is no longer advocated in guidelines. Also, many studies use uneventful follow-up to exclude venous thromboembolism, a common approach in this field of research. The inclusion in our analysis of studies that used uneventful follow-up could lead to a small overestimation of the sensitivity of point of care D-dimer tests, as patients with negative test results but mild DVT and/or PE could be missed if they were managed with uneventful follow-up only.
Fourthly, we restricted our search to studies published in English only, which could have been a potential source of bias. We complemented our electronic searches with recommendations from experts in the field, however, and this approach retrieved no non-English studies. In addition, non-English studies often have little effect on summary estimates in meta-analyses.24
Fifthly, although the quality of included studies was good in general, several studies had differential verification bias and/or incorporation bias (30% and 31%, respectively). The former refers to bias introduced by the use of different reference standards for positive and negative test results. For example, patients with a positive point of care D-dimer test result undergo invasive imaging as reference standard, whereas patients with negative point of care D-dimer tests only receive follow-up or less invasive imaging tests as reference standard. Incorporation bias occurs when the index test is also part of the reference standard. For example, venous thromboembolism is excluded in patients with a low probability ventilation-perfusion scan only if the point of care D-dimer (index test) is negative. Lijmer et al have demonstrated that both forms of bias can affect (often overestimate) the diagnostic performance of an index test.25 However, adding both forms of bias into a covariate analysis did not change the overall sensitivity and specificity of SimpliRED D-dimer and Clearview Simplify D-dimer. A covariate analysis was not possible for Cardiac D-dimer and Triage D-dimer owing to the limited amount of studies available on these tests; however, studies on these tests (notably those on Cardiac D-dimer) did not have differential verification and/or incorporation bias.
Finally, only two studies were performed on Triage D-dimer and only four were performed on Cardiac D-dimer, thus limiting the precision of our results for these tests.
Implications
The laboratory based enzyme linked immunosorbent assay (ELISA) is currently advocated in the literature as the best D-dimer test for excluding venous thromboembolism in a hospital setting. Stein and colleagues report in their meta-analysis that ELISA for D-dimer has an overall sensitivity of 0.96 for DVT and 0.95 for PE.8 We found in our meta-analysis that the quantitative point of care D-dimer tests (Cardiac D-dimer and Triage D-dimer) indeed have similar sensitivity to ELISA for D-dimer. According to Stein and colleagues, the overall sensitivity of laboratory based latex D-dimer tests is 0.85 and 0.89 for DVT and PE, respectively,8 which is equal to the average accuracy of the Clearview Simplify point of care D-dimer test.
Physicians, especially those in primary care, are confronted with a wide spectrum of patients suspected of venous thromboembolism. This spectrum could range from a low risk patient—for example, a 32 year old female on oral contraceptives with minor swelling of the leg—to a high risk patient—such as a 78 year old male with a disseminated malignancy, acute onset of dyspnoea with pain on inspiration, and swelling of the entire leg. However, patients in daily practice are hardly ever “textbook patients.” It is not uncommon for the low risk patient to have DVT and the high risk patient to be diagnosed with another disease, such as heart failure. Hence, it is difficult to make a decision on which patients are to be referred for reference testing (imaging) on the basis of signs and symptoms only. Moreover, this decision often has to be made at the point of care; that is, during the consultation of the patient. One possibility is referring all patients for imaging, but this approach has a poor yield of confirmed cases of venous thromboembolism (the prevalence of venous thromboembolism has even decreased below 10% in recent years26) and thus seems not very cost effective. Physicians in daily practice are, therefore, in need of simple and safe additional tests, such as point of care D-dimer tests, to guide them in their diagnostic decision making.
According to our analysis, using a diagnostic strategy that includes point of care D-dimer testing to rule out venous thromboembolism without the need for imaging could achieve a post-test probability of 2% or less. This probability threshold is generally accepted as safe because the incidence of venous thromboembolism following normal imaging tests, such as compression ultrasonography in patients suspected of DVT, is also around 1-2%.6 Applying this “safety threshold” to our results indicates that all point of care D-dimer tests are sufficiently safe in low risk patients, as they achieved a post-test probability of 0.4-1.1% (table 3 and fig 4). Cardiac D-dimer seems to be the only test with the capacity to exclude DVT in patients with a moderate pre-test probability (up to 27%; fig 4), although only four studies on Cardiac D-dimer were available and thus the 95% confidence interval exceeds 2%.
The decision on which point of care D-dimer test to use depends on the setting. In primary care, the Clearview Simplify D-dimer test has the advantage that it can be performed with capillary blood and thus does not require any other equipment. This makes it possible to have a test result even when making a house call, although at the expense of a lower sensitivity than the quantitative tests. This user friendliness is less important in an emergency department setting, where Cardiac D-dimer and Triage D-dimer may be preferable. These two tests might be a better option not only because of their superior accuracy, but also because other cardiovascular biomarkers—such as brain natriuretic peptide, troponin, and C reactive protein—can be measured with the same instrument.
Conclusions
Both qualitative and quantitative point of care D-dimer tests can safely exclude venous thromboembolism in low risk outpatients. Quantitative tests seem to perform better than qualitative tests, although the quantity of available data is still limited. Also, there are only few studies of these tests in patients suspected of PE. In outpatients suspected of DVT, however, point of care D-dimer tests can contribute important information and guide patient management.
What is already known on this topic
Several meta-analyses have shown that laboratory based D-dimer testing—such as enzyme linked immunosorbent assay—can be used to exclude venous thromboembolism
Excluding venous thromboembolism commonly requires referring a patient to a central laboratory facility
Point of care D-dimer tests are available that could enable exclusion of venous thromboembolism in a near patient situation; however, their diagnostic accuracy is largely unknown
What this paper adds
Point of care D-dimer tests can safely exclude venous thromboembolism in low risk outpatients
Such tests can, therefore, contribute important information at the point of care and guide patient management
Notes
Cite this as: BMJ 2009;339:b2990
Footnotes
Contributors: GJG, KJMJ, and RO participated in study concept and design, acquisition of data, analysis and interpretation of data, and drafting of the manuscript. JBR and LB participated in study concept and design and analysis and interpretation of data, and provided statistical expertise and critical revision of the manuscript. KGMM and AWH participated in study concept and design, analysis and interpretation of data, critical revision of the manuscript, and study supervision.
Funding: Financial support was provided by the Netherlands Heart Foundation (project number 2006B237) and “Zilveren Kruis Achmea” (project number Z195). These organisations had no influence on any aspect of this study.
Competing interests: The authors have conducted previous studies with point of care D-dimer tests and have received Clearview Simplify D-dimer, Cardiac D-dimer, and Triage D-dimer testkits free of charge for study purposes. Manufacturers, however, were in no way involved in the meta-analysis.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.