Article Text

Abstract
Given the importance of unemployment in health inequalities, re-employment of unemployed persons into paid employment may be a powerful intervention to increase population health. It is suggested that integrated programmes of vocational reintegration with health promotion may improve the likelihood of entering paid employment of long-term unemployed persons with severe mental health problems. However, the current evidence regarding whether entering paid employment of this population will contribute to a reduction in health problems remains unambiguous. This systematic review and meta-analysis aimed to assess the effects of re-employment programmes with regard to health and quality of life. Three electronic databases were searched (up to March 2015). Two reviewers independently selected articles and assessed the risk of bias on prespecified criteria. Measures of effects were pooled and random effect meta-analysis of randomised controlled trials was conducted, where possible. Sixteen studies were included. Nine studies described functioning as an outcome measure. Five studies with six comparisons provided enough information to calculate a pooled effect size of −0.01 (95% CI −0.13 to 0.11). Fifteen studies presented mental health as an outcome measure of which six with comparable psychiatric symptoms resulted in a pooled effect size of 0.20 (95% CI −0.23 to 0.62). Thirteen studies described quality of life as an outcome measure. Seven of these studies, describing eight comparisons, provided enough information to calculate a pooled effect size of 0.28 (95% CI 0.04 to 0.52). Re-employment programmes have a modest positive effect on the quality of life. No evidence was found for any effect of these re-employment programmes on functioning and mental health.
Statistics from Altmetric.com
Introduction
Unemployment is a major cause of socioeconomic health inequalities. Prolonged periods of unemployment are associated with an increased risk of all-cause mortality of 63%,1 an 80% increased risk of fatal and non-fatal cardiovascular events,2 a twofold risk of experiencing a limiting illness,3 and a 3.5% increased prevalence of poor mental health.4 Whether unemployment will also lead to the onset or aggravation of severe mental disorders remains unclear. However, unemployment rates among persons with severe mental disorders, for example, schizophrenia, are high (80–90%).5 Besides, unemployment has been associated with a twofold increased prevalence of smoking6 ,7 and a 1.5 times increased prevalence of excessive alcohol use.7 Thus, unemployment may lead to poor health, which in turn will reduce the probability of re-employment.8–10
Observational studies have provided ample evidence that entering paid employment can improve health. A meta-analysis of 15 longitudinal studies showed significant improvements in mental health (effect size 0.89), life satisfaction (effect size 3.04) and subjective physical health (effect size 0.38) among workers who re-entered paid employment.11 Another systematic review of 33 prospective studies showed that entering paid employment reduced the risk of depression (OR 0.52; 95% CI 0.33 to 0.83) and improved general mental health (OR 3.8 and effect size 0.66).12 A recent systematic review of Luciano et al13 showed that entering paid employment was associated with decreased psychiatric treatment and increased self-esteem. These results from observational studies are reflected in the powerful message of the so-called Black report on the health of Britain's working-age population: ‘Work, matched to one's knowledge and skills and undertaken in a safe, healthy environment, can reverse the harmful effects of prolonged sickness or long term unemployment, and promote health, well-being and prosperity’.14
Re-employment of unemployed persons may be a powerful intervention to reduce health inequalities. Crowther et al15 showed in their meta-analysis of randomised controlled trials (RCTs) that people with severe mental illness who received supported employment were more likely to be in competitive employment than those enrolled in a conventional training-placement programme with 34% versus 12% in paid employment after 1 year, respectively. A recent systematic review reported that those who received supported employment were more likely to be in competitive employment (52–60%) compared to control conditions (23%–30%).16
These systematic reviews show that intervention studies have focused on effectiveness for vocational outcomes, such as entering paid employment, hours of paid work per month and income received. The evidence for effectiveness on health-related outcomes is scarce. Two RCTs have reported positive effects such as 4% higher quality of life score17 and 38% reduced healthcare costs.18 However, another RCT on employment interventions did not find any beneficial effects on health or healthcare costs.15 Hence, the current evidence whether entering paid employment of unemployed persons with severe mental health problems will contribute to a reduction in health problems remains unambiguous. Therefore, our aim was to provide a systematic literature review on the effectiveness of re-employment programmes for health and to estimate in a meta-analysis the magnitude of these health benefits.
Materials and methods
Literature search
This systematic review was conducted according to the PRISMA checklist.19 Comprehensive literature searches were conducted by the first author (RMvR) in Medline, Embase and PsycInfo (to March 2015). The full search strategy is presented in online supplementary appendix I.
On the basis of the title and abstract, two reviewers (RMvR and MS) selected the articles for full-text appraisal and final inclusion. Each article had to fulfil all of the following criteria: (I) participants were unemployed, aged between 18 and 65 years, and had mental health problems, (II) the intervention must consist of a form of job placement (eg, competitive employment, sheltered employment), (III) the study design was a randomised controlled trial, (IV) the outcome measures must be health related (eg, physical health, mental health, health status) and (V) the article was published in a peer-reviewed scientific journal and written in English. A consensus method was used to resolve disagreements. The references of all included studies were checked for other possibly relevant articles.
Assessment of risk of bias in included studies
Two reviewers (RMvR, BEC) independently assessed risk of bias of the included studies using the Cochrane collaboration's tool for assessing risk of bias.20 We added one item (10b) concerning fidelity to the methodology of the intervention (see online supplementary appendix I). Each item was rated as showing low, high or unclear risk of bias. Disagreements were resolved in a consensus meeting.
Data extraction
Relevant information was collected on the characteristics of the study population (eg, age, gender, sample size, health problems), health outcomes (eg, physical health, mental health, health status, etc), intervention content, and proportion of persons in competitive employment within the period of intervention. The core findings in each article were expressed by effect sizes. Where possible, these effect sizes were directly extracted from the original article. For articles in which this information was not presented, effect sizes were calculated using raw data.
Data analysis
The effect size was calculated in Review Manager V.5.3 with the Hedges’ g approach, wherein the mean difference at follow-up is divided by the pooled weighted SD at follow-up.20 Unless otherwise indicated, a positive effect size indicated a beneficial effect of integrated programmes of vocational reintegration with health promotion concerning health outcome. We examined potential publication bias using funnel plots. The I2 statistics were used to determine the percentage of total variation across studies, that is, due to heterogeneity rather than chance.21 Owing to the observed heterogeneity, we conducted random-effects meta-analyses on each independent health outcome (using Review Manager 5.3). The pooled effect sizes were calculated according to the Hedges’ g approach, which takes into account the size of the study and provides a weighted effect size. Finally, a meta-regression analysis was carried out to identify follow-up duration, mean difference of the percentage persons in competitive employment, proportion of male, and proportion of persons diagnosed with schizophrenia as potential determinants of the effect size.
Results
Characteristics of the included studies
Our search of the literature resulted in 2091 potentially relevant articles. After title and abstract screening, 1302 articles were retrieved for full-text appraisal. Finally, 16 articles were included in the study (figure 1). Exclusion of articles was mainly due to a lack of health outcome measures (n=42); the study design was not a randomised controlled trial (n=34) or absence of job placement within the intervention (n=21). Most of the included studies presented more than one outcome measure, which can be classified into: functioning (n=9), mental health (n=15) and quality of life (n=13) (see online supplementary appendix II).

Flow chart of the included studies.
In 12 of 16 studies, the intervention was Individual Placement and Support (IPS). IPS emphasises integration of vocational and healthcare services, rapid job finding, obtaining competitive employment that corresponds to the clients’ preferences and clinical and rehabilitative needs, and follow-along support at the job.22 Some studies used a derivate of IPS like Compensated Work Therapy (CWT),23 Assertive Community Treatment with Individual Placement Support (Act-IPS)24 or integrated supported employment combined with work-related social skills training.25 In all studies, the control group received traditional vocational rehabilitation which consists of pre-employment training and medical care as usual. There is some variation between studies in the traditional vocational rehabilitation offered, but none of these programmes had competitive employment as their immediate goal.
Most studies defined competitive employment as a job in the open labour market that anyone could hold with a minimum wage or higher. Some studies used supplementary criteria like that the job was independently held with the participant in continuous employment for at least 30 days18; that fewer than 50% of the participant co-workers had disabilities26; and self-employment was also reckoned as competitive employment.26 The funnel plots in online supplementaryappendix I show that for none of the health outcomes was there an indication of publication bias.
Assessment of risk of bias
Figure 2 shows the overall assessment of risk of bias. The initial agreement of the reviewers on the total assessment of risk of bias was 72% (146 of 204 items). All disagreements were solved in a consensus meeting. A high risk of bias was found with regard to blinding. In eight studies (50%), blinding of participants and personnel and the outcome assessment were lacking. In 14 studies (75%), it was unclear whether cointerventions were avoided, or whether these were similar in the intervention group as well as in the control group.

Assessment of risk of bias.
Functioning
Nine studies described functioning as an outcome measure (see online supplementary appendix II).17 ,18 ,23 ,26–31 Functioning was measured using validated scales like Global Assessment of Functioning (GAF)17 ,18 ,26–31 and Short-Form health survey (SF-36).23 Five studies, describing six comparisons, provided enough information to calculate effect sizes, ranging from −0.12 to 0.09, all not statistically significant (figure 3).17 ,18 ,27 ,29 ,30 The pooled effect size was −0.01 (95% CI −0.13 to 0.11). Within these studies, the percentage of competitive employed ranged from 13% to 55% in the intervention groups compared to 6% to 28% in the control groups. The meta-regression analysis showed no influence of study characteristics on the effect size of functioning.
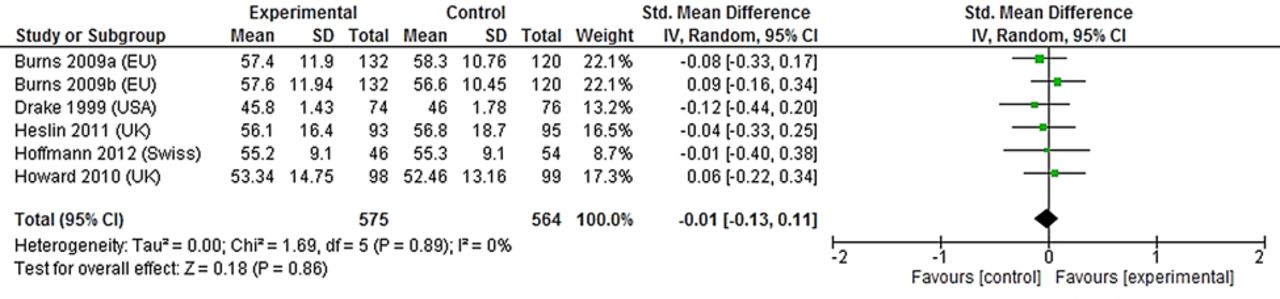
Forest plot of comparison between the intervention group (four studies with Individual Placement and Support, one study with Supported Employment) and control group regarding the outcome measure functioning.
Mental health
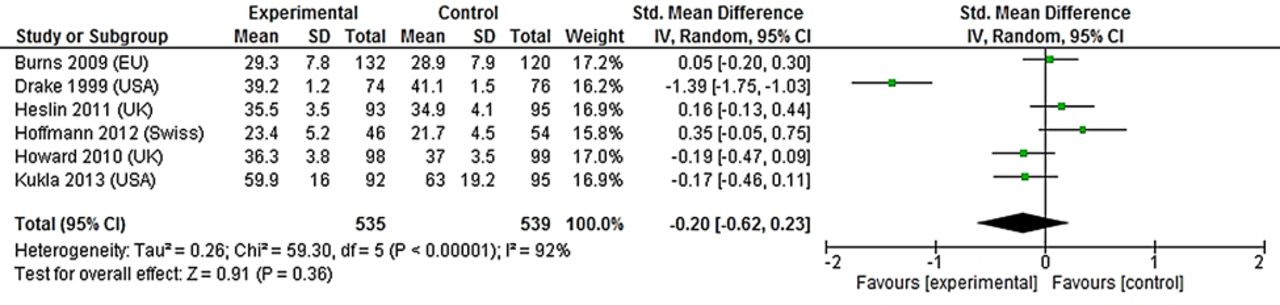
Fifteen studies described mental health as an outcome measure (see online supplementary appendix II).17 ,18 ,23–35 Mental health is the umbrella term for outcomes measured with the Positive and Negative Syndrome Scale (PANSS), Hospital Anxiety and Depression Scale (HADS), Rosenberg self-esteem scale, Brief Psychiatric Rating Scale (BPRS), and Chinese General Self-efficacy Scale (CGSS). One study described a significant difference in self-efficacy in favour of the intervention group.25 Six studies, describing 12 comparisons, provided enough information to calculate effect sizes ranging from −0.58 to 1.39.17 ,18 ,25 ,27 ,30 ,34 Six studies measured psychiatric symptoms and the pooled effect size was 0.20 (95% CI −0.23 to 0.62) (figure 4).17 ,18 ,27 ,29 ,30 ,34 Within these studies, the percentage of competitive employment ranged from 13% to 55% in the intervention groups compared to 2% to 28% in the control groups. The meta-regression analysis showed that studies with over 50% of male participants had a lower effect size of mental health (β −1.43, 95% CI −2.12 to −0.74).

Forest plot of comparison between the intervention group (five studies with Individual Placement and Support, one study with Supported Employment) and control group regarding the outcome measure mental health. A negative effect size means reduced symptoms.
Quality of life
Thirteen studies described quality of life as an outcome measure.17 ,18 ,24–28 ,31–34 ,36 ,37 Quality of life was measured using validated scales like the Manchester Short Assessment of Quality of Life (MANSA),18 ,32 ,35 the Lancashire Quality of Life Profile,27 Lehman's Quality of life interview,17 ,24 ,28 ,31 ,34 the Wisconsin Quality of Life Index26 ,36 or the WHO Quality of Life Measure. 33 Seven studies, describing eight comparisons, provided enough information to calculate effect sizes, ranging from 0.00 to 0.9917 ,18 ,25 ,27 ,32 ,34 ,36 with a pooled effect size of 0.28 (95% CI 0.04 to 0.52) (figure 5). Within these studies, the percentage of competitive employment ranged from 13% to 74% in the intervention groups compared to 2% to 68% in the control groups. The meta-regression analysis showed no influence of the study characteristics on the effect size of quality of life.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of comparison between the intervention group (six studies with Individual Placement and Support, one study with Supported Employment) and control group regarding the outcome measure quality of life.
Discussion
This systematic review showed some indications that re-employment programmes based on the place-then-train model had a positive effect on quality of life with a pooled effect size of 0.28 (95% CI 0.04 to 0.52). However, there is no evidence for benefits concerning mental health and functioning.
These results seem to partly contradict observational studies that have provided evidence that entering paid employment can improve health9 and decrease psychiatric treatment.13 Mueser et al37 as well as Bond et al38 showed in their RCTs that after 18 months follow-up participants with severe mental illness who obtained competitive employment tended to have less psychiatric symptoms, better overall functioning and higher self-esteem.
In the current systematic review, we could not demonstrate that entering paid employment of unemployed persons with severe mental health problems had a substantial impact on health status. The estimated pooled effect sizes were small and reflect modest clinically important differences. A few explanations can be discussed for the contrasting results between experimental and observational studies. First of all, observational studies present their effects between the group which became employed and the group which stayed unemployed. In an RCT setting, this would imply a comparison between 100% work resumption in the intervention group compared to 0% work resumption in the control group. However, in the studies in this review, the percentage of participants in competitive employment ranged from 13% to 74% in the intervention group compared with 2% to 68% in the control group. In our secondary analysis, a larger difference in the proportion of participants who gained paid employment between the intervention and control groups was not associated with higher effect size, although the number of studies available for this analysis was limited.
Second, RCTs were generally conducted in small study populations typically varying from 37 to 132 persons per study arm, whereas observational studies investigated much larger populations. The modest sample size makes it difficult to demonstrate differences between groups, especially with regard to health outcomes. In addition, participants were followed up for a relatively short term (range 12–24 months) with few measurements compared to observational studies (range 1–15 years), which makes it difficult to determine the influence of work resumption on sustainability of (possible) health effects. In many RCTs, health outcomes were frequently presented as secondary outcomes, or were absent. Therefore, the studies were not primarily designed for demonstrating differences concerning health outcomes. Besides, in some studies, health was measured by the presence and severity of (chronic) health problems. During follow-up, the presence of (chronic) health problems will not change in many cases, whereas the individual’s resilience and capacity to cope with and to adapt according to health problems may change. Consequently, within vocational rehabilitation, outcome measures of health should reflect ‘health, as the ability to adapt and to self-manage’.39 Last, observational studies are susceptible to selection bias, whereas randomisation in RCTs ensures that prognostic factors are equally distributed across intervention and control groups. In observational studies, the healthy worker effect may have occurred, whereby healthier persons are more likely to enter paid employment and remain employed than persons with health problems. As a result, the findings of observational studies may be overestimated.
In addition to these methodological issues, the year of conducting studies and policies on a national level concerning social protection may influence the association between employment and health. A prospective study of Martikainen and Valkonen40, for example, found that the association between unemployment and mortality weakened in periods with increasing unemployment rates. Furthermore, in countries with policies securing a high level of social protection, the impact of job loss on workers’ health was less compared to countries with limited social protection. McLeod et al41 determined that the unemployment-mortality association was much stronger in the USA (low level of social protection) than in Germany (high level of social protection).
There is considerable evidence that there is a fundamental link between health and socioeconomic indicators such as educational qualifications, job status and income. As a result, health inequalities often go hand in hand with other socioeconomic inequalities.14 For example, unemployed persons have a higher mortality rate and more often experience diseases with functional limitations.8 ,42 Inclusion of unemployed persons in the workforce through re-employment programmes is therefore an important strategy to reduce socioeconomic inequalities. The effect sizes found in this systematic review are comparable to those found in many preventive interventions on improvement of unhealthy behaviour. For example, a recent meta-analysis of 18 studies on the effectiveness of workplace health promotion programmes showed an effect for self-perceived health with an effect size of 0.23 (95% CI 0.13 to 0.33).43 Fortunately, the awareness about the importance of employment for health is certainly increasing, as reflected in the rapidly growing amount of research on this topic and by the policies developed in different countries to integrate health services with employment services. However, one of the challenges is to improve the health-related and work-related knowledge of the primary care workforce, as they are the gatekeepers to specialist medical care and key actors in preventing labour market exclusion.44
Shortcomings in the risk of bias assessment were found with regard to blinding of participants, personnel and the outcome assessment and indistinctness whether cointerventions were avoided or not. Knowledge of group assignment by participants and outcome assessors can affect the subjective health-related outcomes reported in most studies. Participants who know that they are allocated to the intervention group may be more inclined to report a positive effect. Besides, if personnel are not blinded, their attitudes in favour of or against the intervention can be transferred to the participant.20 ,45 Furthermore, the lack of information on cointerventions makes it difficult to establish whether the effects reported are the result of the evaluated intervention or not.
This systematic review shows indications that re-employment programmes based on the place-than-train model have some effect on the quality of life of participants, but the effect size is modest. The current systematic review highlights two important challenges for the future. First, policymakers and healthcare providers must be aware that paid employment can be seen as a therapeutic intervention and can contribute to reducing socioeconomic health inequalities. That is why the knowledge of professionals on this topic needs to be improved. Second, research should focus on establishing the effectiveness of re-employment programmes based on the place-and-train model with regard to health by conducting RCTs with a larger sample size, with health outcomes as their primary outcome measure, and with longer follow-up periods.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors RMvR executed the systematic review, conducted the literature search, selected relevant articles for inclusion, performed the data extraction, analysed the data and wrote the manuscript. He is the guarantor. BEC helped conduct the literature search, selected relevant articles for inclusion and contributed to the content of the manuscript. MS selected relevant articles for inclusion and contributed to the content of the manuscript. AB initiated the study and contributed to the content of the article. All four authors made a substantial contribution to the information and material submitted and have read and approved the final version.
Funding This work was supported by the Netherlands Organisation for Health Research and Development (ZonMW, grant 200210005).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.