Article Text

Abstract
Study objective: To estimate the impact of the severe acute respiratory syndrome (SARS) outbreak in early 2003 on a tertiary care hospital in Taiwan, ROC.
Methods: The study estimated the utilisation of resources related to infection control, SARS related medical services, and routine medical services, and SARS related medical outcomes at National Cheng Kung University Hospital (NCKUH) from 25 March to 16 June 2003 through a cross sectional survey of hospital records.
Results: A mean of 5100 persons per day (95%CI 4580 to 5610) underwent fever screening at the outpatient and emergency department (ED) entrances to the hospital, of which 35 per day (95% CI 30 to 40) were referred for further evaluation for suspected or probable SARS. ED isolation surge capacity was created via 12 new beds outside the ED: eight for SARS assessment, three for patients awaiting inhospital bed assignment, and one for resuscitation. A total of 382 patients were fully evaluated for suspected or probable SARS outside the ED, of which 27 were admitted. The mean numbers of outpatient clinic patient visits, ED visits, ED trauma patient visits, ED admissions, hospital admissions, and operative procedures decreased during the outbreak. Thirty eight patients were hospitalised with suspected SARS, of which three received the final diagnosis of probable SARS. Two patients with probable SARS died. No cases of nosocomial SARS transmission occurred.
Conclusions: This SARS outbreak was associated with substantial use of hospital and ED resources aimed at infection control, comparatively less use of resources related to the medical care of patients with suspected or probable SARS, and decreased use of routine medical services.
- infection control
- severe acute respiratory syndrome
- SARS, severe acute respiratory syndrome
- ED, emergency department
Statistics from Altmetric.com
On 14 March 2003, an outbreak of severe acute respiratory syndrome (SARS) was recognised in Taiwan, Republic of China, when the first two probable cases of SARS were diagnosed in a recent traveller to Guangdong Province and his wife.1,2 By 22 April, Taiwan experienced only 29 probable SARS cases, four of which resulted from secondary transmission from the index case (one physician and three family contacts).1,3,4 However, by 22 May, the nosocomial spread of SARS in at least nine hospitals catapulted the number of probable cases to 583, including 60 deaths.1,5 When the last probable case of SARS was reported on 15 June, 671 probable cases of SARS had occurred, with 83 deaths, seven of which were in healthcare workers.4,6,7
With its ability to rapidly cross international borders, spread within hospitals, and affect heathcare workers, the recent outbreak of SARS in Taiwan, ROC and other countries posed a new challenge for hospitals worldwide.1,2,8–20 This SARS outbreak also demonstrated many features suggestive of a bioterrorist attack, including the aerosol spread of infection, predominate pulmonary pattern of disease, multiple patients with similar signs and symptoms, simultaneous presentation, multiple simultaneous outbreaks, and no identified natural vector. Lessons learned from this SARS outbreak may not only assist emergency preparedness for future outbreaks of SARS, but also for intentional releases of contagious biological agents. Accordingly, we sought to estimate the impact of the SARS outbreak at a tertiary care medical centre, National Cheng Kung University Hospital (NCKUH), in terms of resource use and SARS related medical outcomes.
METHODS
Study design
We estimated the impact of SARS on NCKUH through a cross sectional survey of hospital records, and when relevant, a case-control comparison of hospital records during the same period in 2002.
Study setting
The study setting was NCKUH, one of 15 tertiary care medical centres in Taiwan, located in the south western city of Tainan (fourth most populous city in the country after Taipei, Kaohsiung, and Taichung). NCKUH serves a population of 1.7 million and has a catchment area of about 2200 km2. The hospital has 1173 beds, 83 ICU beds, and 60 ED beds. The annual ED census is 62 606, with 13 545 admissions per year.
Study period
We defined the study period as the duration of the SARS outbreak at NCKUH beginning on 25 March and ending on 16 June 2003. We designated 25 March as the first day of our study, because on the evening of 24 March NCKUH activated its hospital emergency plan in response to the growing SARS outbreak. On 26 March NCKUH received its first suspected case of SARS. We selected 16 June as the last day of the study, because the following day the World Health Organisation removed its travel advisory for Taiwan.21
Definitions
We used the definitions of suspected and probable SARS recommended by WHO and implemented in Taiwan on 17 March.22 Diarrhoea was also used as a criterion for suspected SARS in Taiwan, because diarrhoea had been reported as a prominent early symptom in Hong Kong and Taipei.1,16 No attempt was made to classify probable patient-cases of SARS in Taiwan into a “confirmed” patient-case category, because no international consensus existed for the case definition of “confirmed SARS” during the study period. We also used the term “possible SARS” to describe those patients undergoing evaluation for suspected or probable SARS.
Methods and measurements
We developed measurements for estimating resource use at the hospital based on methodology described by Ricci and Pretto for assessing hospital emergency response to major disasters.23 In developing these measurements, we considered the major categories of resource use during the outbreak—the implementation of infection control measures to prevent the secondary transmission of SARS, the provision of SARS related medical services to those exposed to or infected with the SARS virus, and the provision of routine medical services to those with ongoing medical needs (tables 1–4).
Infection control measures at NCKUH during the SARS outbreak
We also sought to estimate the major SARS related medical outcomes at the hospital during the outbreak (table 5), including the number of secondary cases of SARS in personnel, patients, and visitors, the number of patients hospitalised with the final diagnosis of suspected or probable SARS, and the number of deaths in patients with the final diagnosis of suspected or probable SARS.
Data collection and processing
The first author collected daily and cumulative data concerning resource utilisation from computer databases or hand written logs maintained by a variety of hospital departments (that is, emergency medicine, family medicine, infection control, materials supply, personnel secretary general, surgery). Data were collected concurrently during the SARS outbreak at NCKUH in 2003 and retrospectively during the same period in 2002.
The first author also collected cumulative data concerning SARS related medical outcomes from computer databases maintained by the hospital infection control office. The hospital infection control officer established the number of cases of nosocomial transmission of SARS at NCKUH via inhospital surveillance and by matching the names of all NCKUH personnel and patients during the SARS outbreak against a national insurance database to discover if any of these people were admitted for suspected or probable SARS at another hospital in Taiwan during the outbreak. We did not attempt to identify spread from asymptomatic carriers, as no methodology existed to identify such individuals during the outbreak. Data were entered in a database, using Windows XP Excel software (Microsoft Corporation, Redmond, WA).
Primary data analysis
Data were described by simple descriptive statistics, using SPSS software (11.5 version, Chicago, IL). As only periodic (not daily) data were available from the materials supply department for the use of N95 and surgical masks, we present daily means without 95% CI. Mean data from the SARS outbreak in 2003 were compared with data from the same period in 2002 using 95% CI. This study was approved by the IRB at NCKUH on 3 May 2003.
RESULTS
Tables 1–4 show resource use at NCKUH during the SARS outbreak. Table 2 shows the isolation surge capacity—numbers, types, and locations of isolation beds—at NCKUH before and after the SARS outbreak. Table 4 compares routine resource use during the SARS outbreak with the same time interval in 2002. Other infection control measures and SARS related medical services shown in tables 1 and 3 did not have correlates in 2002. Not shown in table 4 are the three patients with pulmonary tuberculosis, who were transferred from NCKUH to a local tuberculosis hospital for negative pressure isolation during the outbreak (compared with no patients transferred out of NCKUH during the same period in 2002). Table 5 shows key medical outcomes at NCKUH during the SARS outbreak.
Isolation surge capacity at NCKUH before and after the SARS outbreak
SARS related medical services at NCKUH during the SARS outbreak
Routine medical services at NCKUH during the SARS outbreak compared with the same period in 2002*
SARS related medical outcomes at NCKUH during the SARS outbreak
Limitations
Some data concerning resource use were unavailable, such as the number of healthcare workers wearing personal protective equipment in various units, the number of decontaminations or hand washings performed, or the number of SARS related laboratory specimens processed. We were also unable to estimate the number of patients hospitalised in critical care beds during the SARS outbreak because of an absence of records. Furthermore, the comparison of time periods in 2002 and 2003 may suffer from undetermined confounding variables unrelated to SARS, such as the burden of other diseases or injuries on the hospital or differences in the quality and timeliness of medical care.
We also did not evaluate the adequacy of medical management of the patients with suspected or probable SARS. In addition, determination of the cause of death in patients with suspected or probable SARS was limited by national policy during the outbreak that prohibited necropsy of these decedents in order to rapidly expedite their cremation. Finally, the low incidence of probable SARS at NCKUH may limit the ability to extrapolate the NCKUH experience to other settings.
DISCUSSION
Infection control
The SARS outbreak produced an enormous effort to prevent the nosocomial spread of SARS. A mean of 5100 persons per day underwent fever screening each day at two check points outside the hospital (outpatient and ED entrances) during the outbreak. In addition, the 1500 personnel reporting to work each day had their body temperatures checked twice per eight hour shift.
Thousands of persons wore respiratory personal protective equipment each day. In general, hospital personnel and patients exposed to patients or environments with possible, suspected, or probable SARS wore N95 masks. Personnel in these areas also wore water impermeable gowns, double layered latex gloves, goggles, shoe covers (data not shown). Personnel participating in the resuscitation of patients with possible, suspected, or probable SARS wore powered air purifying respirators with hoods (data not shown). Personnel and patients in non-SARS related areas were also given the option of wearing N95 masks, accounting for mask consumption in low risk areas.
ED isolation surge capacity was generated via the creation of 12 new beds in three temporary shelters outside the ED. Eight beds were created in one tent (deployable rapid assembly shelter or DRASH) for the evaluation of patients for suspected or probable SARS (SARS assessment unit). Two beds were created in another tent for patients with suspected SARS awaiting an inhospital bed assignment. Another bed was established in another tent for patients with probable SARS awaiting an inhospital bed assignment. Still another bed was created in the open air decontamination area outside the ED for the resuscitation of patients with possible SARS (SARS resuscitation subunit). The provision of these beds in shelters outside the ED not only created necessary barriers between various subgroups of patients with possible, suspected, or probable SARS and the normal ED population, but also enabled the hospital to rapidly expand its ED isolation capacity without having to physically modify the existing ED. The generation of ED isolation surge capacity via temporary shelters outside the ED may offer an attractive strategy for EDs faced with long term overcrowding and facilities with fixed capacities.
NCKUH also increased inhospital isolation surge capacity by creating seven new single room isolation beds, 12 new single room NPI beds, and six new single room NPI critical care beds. Surge capacity for hospitalised patients with suspected or probable SARS requiring isolation was produced by transforming the 50 bed pulmonary medicine ward (with its pre-existing 10 NPI beds) into a SARS isolation subunit with 22 single room NPI beds. On average, 12 of these beds were occupied per day during the outbreak.
Isolation surge capacity for critically ill patients with suspected or probable SARS was created by transforming another section of the pulmonary medicine ward into a SARS critical care unit with six new single room NPI critical care beds. In addition, the surgical intensive care unit was closed and its pre-existing four single room NPI critical care beds were transformed into a second area for SARS critical care. This additional capacity was produced at the cost of a reduction in elective surgeries at NCKUH, as surgical ICU patients with non-SARS related conditions were henceforth hospitalised in the limited capacity burn unit. On average, four of these SARS critical care beds were occupied during the outbreak.
Isolation surge capacity for employees requiring inhospital observation for possible SARS was produced by transforming a 50 bed psychiatric ward immediately adjacent to the pulmonary medicine ward into an employee isolation subunit with 25 single room isolation beds. Employees were also given the option of home isolation for three days during the outbreak, but many chose hospital isolation to spare their families from exposure to possible SARS. On average, five of these beds were occupied per day during the outbreak.
These extensive efforts to control infection were necessary, because no other prophylactic or therapeutic interventions were known to be effective against SARS. In particular, the successful containment of SARS at NCKUH seems to have hinged upon the aggressive early identification and isolation of suspected or probable patient-cases at the level of the ED. In the absence of adequate immunoprophylaxis, it is probable that EDs and hospitals facing future outbreaks of SARS will be required to implement similar infection control efforts. It also probable that infection control efforts of this type and magnitude will be required in outbreaks of other highly contagious diseases with respiratory spread to which populations may be susceptible (for example, the intentional release of smallpox against an unimmunised population or a highly virulent influenza pandemic).
SARS related medical services
The demand for SARS related medical services was comparatively less. Although 382 patients underwent evaluation for suspected or probable SARS in the SARS assessment unit outside the ED (including physician examination, chest radiograph, and selected laboratory tests), only three patients required resuscitation in this area. A total of 38 cases of suspected SARS were admitted to the hospital (27 from the SARS assessment unit and 11 as transfers from other hospitals). No cases of suspected or probable SARS were transferred out, suggesting that NCKUH retained the capacity to provide SARS related medical care during the entire outbreak. Altogether NCKUH provided medical care to three patients with probable SARS (compared with 671 probable patient-cases of SARS in Taiwan during the study period).6 Two patients with probable SARS underwent unsuccessful resuscitation attempts in the SARS critical care unit. A third death occurred in a patient with suspected SARS in the SARS isolation unit, who was not resuscitated pursuant to a “do not resuscitate” order. No other patients with suspected or probable SARS required resuscitation during the outbreak. These three deaths also indicate that the outbreak had a comparatively low impact on SARS related morgue services at NCKUH.
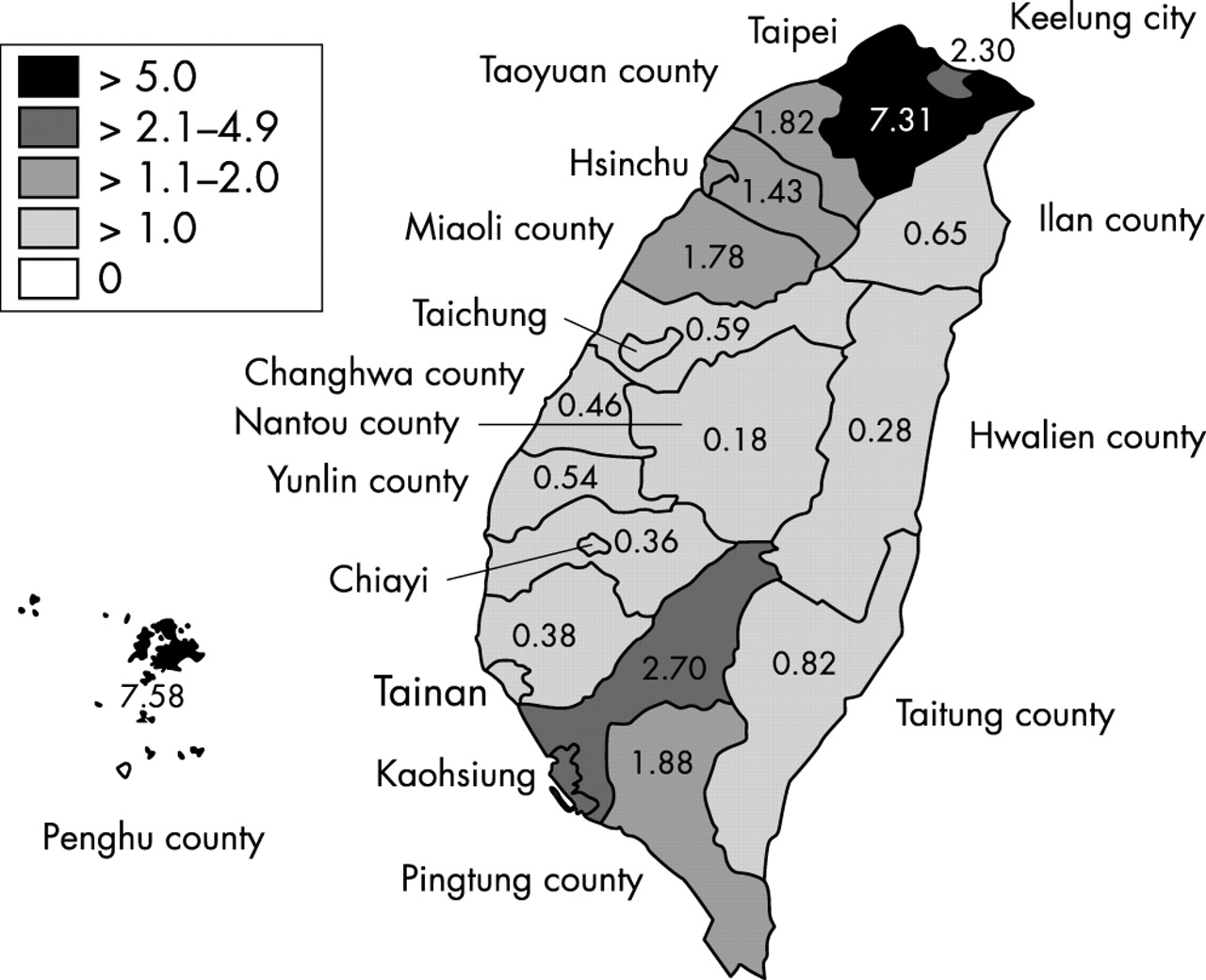
The low impact of this outbreak on SARS related medical services is likely to have been influenced by the successful containment of SARS at NCKUH and elsewhere in Tainan county as the outbreak continued. Ultimately, Tainan county experienced the third lowest incidence of probable SARS in the country, suggesting that efforts to control the nosocomial spread of SARS in this area was an important factor (fig 1).

{kind=link}
Number of patient-cases of probable SARS per 100 000 population in counties in Taiwan, ROC during the SARS outbreak.
Routine medical services
Reductions in the provision of several routine hospital services occurred during the SARS outbreak when compared with the same period in 2002, including the mean daily number of ED patient visits (18% decrease), ED trauma patient visits (13% decrease), ED admissions (17% decrease), outpatient clinic visits (25% decrease), hospital admissions (17% decrease), patients hospitalised (18% decrease), and operative procedures performed (23% decrease). Similar decreases were reported at Prince of Wales Hospital in Hong Kong during its SARS outbreak in which ED visits declined an estimated 20%–30% and major surgery was curtailed.8
The reasons for these decreases are likely to be complex, relating to reductions in both the demand for services and their availability. A major contributing factor was probably that some patients avoided hospitals, because hospitals were perceived as places where SARS might be acquired. Another factor contributing to the decline in ED and outpatient clinic visits was probably the public appeal by the TCDC on 22 May for patients with minor illnesses to stay away from hospitals.24 The extensive fever screening at NCKUH may have been another deterrent, as febrile patients were subject to further assessment (or quarantine at a local military camp if they refused to comply). It is also conceivable that the decrease in ED trauma patient visits was related to the widely reported avoidance of public places during the outbreak, which may have reduced the incidence of alcohol related or interpersonal injury.25–28
Reductions were probably also influenced by the decreased availability of hospital services at NCKUH. For example, the ED was periodically close to saturation and EMS traffic was diverted to other facilities, the outpatient clinics refilled medications by mail to keep patients away, and the department of surgery cancelled numerous elective operations. On the other hand, only three patients with pulmonary tuberculosis were transferred out of NCKUH during the study period (to a local tuberculosis hospital), suggesting that the outbreak had only a minor impact on the ability of NCKUH to provide NPI for non-SARS related medical conditions.
Despite the potential risk of acquiring SARS (that is, 27% of all probable cases in Taiwan reportedly occurred in healthcare workers) or even being quarantined if found to be febrile, the proportion of personnel not reporting to work per day during the SARS outbreak (relative to the number reporting to work) decreased in comparison with 2002.29 Although we did not investigate the reasons why healthcare workers continued to report to work during the SARS outbreak at NCKUH, the extensive efforts to control infection at the hospital coupled with lack of nosocomial spread may have been factors.
Medical outcomes
No cases of the nosocomial transmission of SARS occurred during the outbreak. Underlying factors are likely to include the extensive hospital wide infection control measures implemented by the hospital during the outbreak as well as the low incidence of probable SARS in the NCKUH patient population (which in turn was probably affected by the lack of nosocomial transmission). Of the 38 patients admitted with suspected SARS, only three received the final diagnosis of probable SARS. Two of these patients died during the SARS outbreak. The factors influencing death in patients with SARS are probably complex, including factors related to the virus, host, and medical care. Although no studies have shown the benefit of one particular medical regimen over another for SARS, it is conceivable that delays in ventilatory support played a part in these two deaths, as their resuscitations were characterised by delays for responding staff to first put on powered air purifying respirators with hoods.30 A third death occurred in a patient with the final diagnosis of suspected SARS and terminal lung cancer, who was not resuscitated pursuant to a “do not resuscitate” order.
In conclusion, this SARS outbreak was associated with substantial use of resources related to infection control, comparatively less use of resources related to the medical care of patients with suspected or probable SARS, and decreased use of routine medical services compared with the same time interval during the previous year.
REFERENCES
Footnotes
-
Funding: none.
-
Conflicts of interest: none declared.