Long covid—an update for primary care
BMJ 2022; 378 doi: https://doi.org/10.1136/bmj-2022-072117 (Published 22 September 2022) Cite this as: BMJ 2022;378:e072117
- Trisha Greenhalgh, professor of primary care health sciences1,
- Manoj Sivan, associate professor in rehabilitation medicine2,
- Brendan Delaney, professor of medical informatics and decision making3,
- Rachael Evans, associate professor in respiratory medicine, associate professor in respiratory medicine4,
- Ruairidh Milne, person with long covid and, emeritus professor of public health5
- 1Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
- 2Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, UK
- 3Institute of Global Health Innovation, Imperial College London, London, UK
- 4Institute for Lung Health, Department of Respiratory Sciences, University of Leicester, Leicester, UK
- 5School of Healthcare Enterprise and Innovation, University of Southampton, Southampton, UK
- Correspondence to T Greenhalgh trish.greenhalgh{at}phc.ox.ac.uk
What you need to know
Long covid (prolonged symptoms following covid-19 infection) is common
The mainstay of management is supportive, holistic care, symptom control, and detection of treatable complications
Many patients can be supported effectively in primary care by a GP with a special interest
This article updates and extends a previous BMJ Practice Pointer published in August 2020 when almost no peer reviewed research or evidence based guidance on the condition was available.1 In this update we outline how clinicians might respond to the questions that patients ask.
Definition
The term “long covid”2 refers to prolonged symptoms following infection with SARS-CoV-2 that are not explained by an alternative diagnosis. It embraces the National Institute for Health and Care Excellence (NICE)’s terms “ongoing symptomatic covid-19” (symptoms lasting 4-12 weeks) and “post covid-19 syndrome” (symptoms beyond 12 weeks),3 the US Centers for Disease Control and Prevention’s group of “post-covid conditions,”4 and the World Health Organization’s “post covid-19 condition.”5
Epidemiology
In mid-2022, approximately 70% of the UK adult population had been infected with SARS-CoV-2.6 Of these, almost 2 million report covid-19 symptoms persisting for more than four weeks; 807 000 (41% of all people with long covid) for more than a year; and 403 000 (19%) for more than two years.7 Based on workforce data from the British Medical Association,8 a full time equivalent general practitioner with an average list size (approximately 2000) has around 65 patients with long covid, 27 of whom will have been unwell for more than a year, and 12 for more than two years. Most general practices have far fewer patients with a long covid diagnostic code on their electronic health record9 for a combination of reasons, including lack of presentation, lack of recognition, and inadequate coding. These figures do not cover children, who are outside the scope of this article.
Rates of long covid are lower in people who are triple vaccinated, but prevalence of long covid (persistent symptoms at 12-16 weeks after laboratory confirmed SARS-CoV-2 infection) remains high at 5% for the delta variant and 4.2% for omicron BA.2.10
Symptoms and case definition
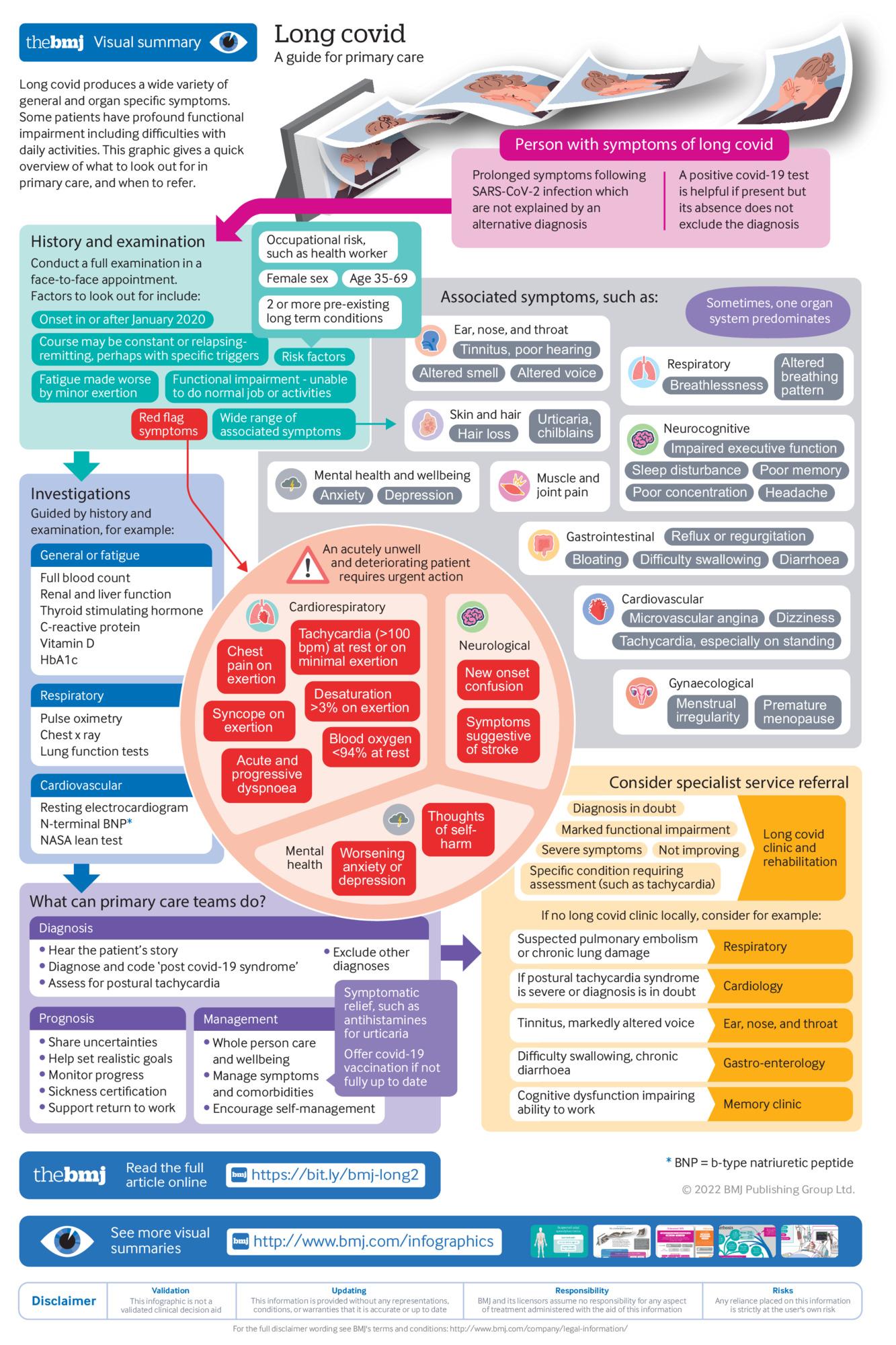
Long covid may be diagnosed late or not at all,111213 so both generalists and specialists should be alert to it as a differential, while also being aware that patients can develop other persistent symptoms following acute covid-19 that are not necessarily caused by covid-19. Long covid is characterised by a constellation of general and organ specific symptoms, the commonest of which are summarised in the infographic. These multiple manifestations lead to difficulties with daily activities such as washing and dressing, low exercise tolerance, and impaired ability to work (either at all or partially), and result in reduced quality of life.5141516171819
Symptoms typically occur across multiple systems concurrently but sometimes one organ system (eg, cardiovascular) dominates. Phenotyping studies have identified several symptom clusters (table 1), with severe cases characterised by greater number and intensity of symptoms and greater functional impairment.333435 Some patients’ long covid follows a fairly constant course, while others experience relapsing and remitting symptoms, sometimes with particular triggers.36
Symptoms, investigation, and management of long covid
Fatigue—described by one patient as “like the most severe jet lag and hangover I’ve ever had”37—is the commonest symptom and may be associated with severe functional impairment; reduced exercise tolerance is also common. Some patients develop post-exertional malaise (PEM) or post-exertional symptom exacerbation (PESE),11 defined as worsening of symptoms following physical or mental exertion, typically 12 to 48 hours after activity and lasting days or (rarely) weeks.38 Long covid has evident (but under-researched) overlaps with chronic fatigue and myalgic encephalomyelitis.39Box 1 gives examples of patients’ accounts.
Patients’ accounts of long covid symptoms and accessing services, from research interviews with people with long covid134041
“I had an odd rash for quite a while; it kept coming and going … very itchy cough ... very mild asthma … I started getting the odd headache again .... Pins and needles, feet going completely numb ... all sorts of odd symptoms, I just kept putting it down to grief until a couple of months in, a friend said, ‘Look, do you think this could be covid?’”
“The fatigue is literally like hitting a wall. I can’t stay awake any more. It’s just like, wow, I have to go to bed.”
“I’d had 11 days of feeling great. And after [a particular] weekend I crashed again. And again it seemed to last for weeks of having these waves of symptoms: shortness of breath, diarrhoea, muscle aches, complete fatigue.”
“I think it [consultation with general practitioner] was a really positive experience and I felt really listened to, and she was able to be honest at that point and said I don’t really know what I can do to help you but you can phone me or email me at any point.”
“My last interaction with my GP was in June. I asked about my lungs, and he said, ‘What do you want me to do about it? You tell me. I have no idea.’ It felt very dismissive […]. ‘Nothing’s got any evidence so, yeah sorry, I can’t help.’ I went back to work after five weeks still very unwell because nobody believed in long covid in May, they just didn’t believe it.”
RETURN TO TEXTQuestions patients ask
Why did I get long covid, and what caused it?
Symptoms (especially fatigue) may persist after many infectious illnesses, including other coronaviruses such as SARS and MERS.42 But no clear explanation exists for why a particular individual develops long covid while another recovers quickly.
Long covid is more common in those who had more severe acute disease43 but may occur after mild or even asymptomatic disease.3444 It is more common in people who were hospitalised, aged 35 to 69, female, living in deprived areas, working in healthcare, social care, or education, with high body mass index, and with more than one pre-existing, activity limiting health condition.734444546
The underlying cause of long covid is not fully known, but several interacting mechanisms likely contribute.474849 A chronic, low grade inflammatory response is correlated with the severity of ongoing symptoms in patients who were hospitalised.33 Some patients have evidence of multi-organ microvascular disease characterised by immunothrombosis and endothelial dysfunction,4748 and some show an autoimmune response, where the body starts to recognise its own tissues and organs as foreign.50 Some patients have covid induced neurological damage, particularly to the autonomic nervous system, which controls involuntary functions like heart rate.354651 Being chronically ill and with unpredictable relapses may lead to loss of work, income, and social interaction, which in turn can lead to poor mental health.14 Structural inequalities such as poverty, overcrowding, poor working conditions, and inability to access services are important in the development and course of covid-19 and may form an important context for long covid.525354
What can my primary care team do for me?
Patients with long covid greatly value input from their primary care clinician. Notwithstanding prevailing uncertainties and the lack of definitive curative therapies, generalist clinicians can help patients considerably by
Hearing the patient’s story and validating their experience
Making the diagnosis of long covid (which does not have to be by exclusion) and excluding alternative diagnoses
Providing holistic, relationship based care through continuity of care with a sympathetic clinician who knows the patient
Conducting a full examination in a face-to-face appointment
Encouraging self-management and directing to resources (box, Resources for patients)
Managing specific symptoms (table 1)
Detecting and actioning “red flag” symptoms (infographic)
Managing comorbidities (especially diabetes and cardiovascular disease and risk factors)
Sharing the uncertainties of prognosis
Helping set realistic goals for recovery (including pacing to avoid PESE)
Considering referral to other members of the primary care team (eg, pharmacist, advanced clinical practitioner, community physiotherapist) or social support services as appropriate
Monitoring progress
Assessing mental wellbeing and managing depression and anxiety as needed
Providing sickness certification
Supporting self-advocacy (eg, with employer when returning to work)
Entering the correct code for long covid on the electronic patient record.55
All this takes time, and several consultations may be needed.
What investigations should I have?
Long covid affects patients in different ways and to different degrees. Because a key component of care is investigating and managing risk factors and comorbidities, no standard protocol exists for assessment. Ideally, every patient should have an in-person consultation including a full history, clinical examination, and review of comorbidities and social circumstances.
Initial investigations are guided by the predominant symptoms (table 1) and are primarily directed at excluding serious alternative diagnoses. Patients may have heard about tests for immunological and clotting function; such tests are the subject of intense research currently, but they do not yet have an established role in clinical practice.
What treatments are available?
As with investigations, no standard protocol exists for treating long covid. Recovery programmes have been designed and implemented with the aim of improving physical health and mental wellbeing.56 The optimal content, delivery method, and duration of these programmes is currently unknown, but under investigation (see EPPIcentre resource, box, Resources for healthcare professionals). Programmes to date have been modelled on successful examples such as pulmonary and cardiac rehabilitation, but with substantial modification for adults with long covid who are particularly managing fatigue and PESE.57
Much current medication is directed at symptom control (paracetamol or non-steroidal anti-inflammatory drugs for fever and pains, antihistamines for allergic symptoms). Table 1 lists other specific medications for different symptom clusters. Covid vaccines may help long covid symptoms and should be discussed with all those without contraindications who are not already fully vaccinated; they should be told that improvement may be modest and not all patients benefit (indeed, some may experience worsening of symptoms).335859
How will I know if I’m getting better?
The best guide to whether a patient is getting better is whether they feel better (and if they do, whether this reflects permanent recovery or temporary remission). A patient reported outcome measure that measures symptom severity across 10 domains as well as functional disability and overall health state, known as the Covid-19 Yorkshire Rehabilitation Scale (C19YRS), has been developed and validated (see multimedia appendix).6061 This instrument, which is less burdensome for patient and clinician than multiple condition specific scales, is available in document format (see bmj.com) and as a smartphone app for the patient linked to a web portal for the clinician (https://c19-yrs.com/).60 It can be completed at intervals over time to chart the patient’s recovery (or lack of it).
When will I get better?
The time course of recovery is extremely variable. Approximately two thirds of patients who have persisting symptoms at four weeks can expect to be recovered by 12 weeks.43 Those still unwell at 12 weeks may benefit from specialist multidisciplinary care. They may still improve, albeit at a slower rate, but many patients appear to plateau and their illness course may fluctuate with exacerbations triggered by physical or mental stress.73362 It is currently not possible to predict which patients will recover within weeks and which will develop a long term condition.
Do I need to see a specialist?
Many people with long covid can be managed effectively in primary care, but “red flag” symptoms (infographic) require urgent referral and action. Additionally, some patients—those with multiple severe symptoms (especially if both physical and mental health are affected), symptoms persisting after a severe acute illness (eg, a period in intensive care), atypical symptoms, profound functional impairment (eg, unable to work or attend college), and those needing confirmation that self-management or supported rehabilitation is safe and appropriate—benefit from specialist referral.63 Ideally, this should occur in a dedicated “single point of entry” long covid clinic. These integrated clinics spanning primary and secondary care give patients access to additional investigations and other specialists (typically including respiratory medicine, cardiology, neurology, rehabilitation medicine, therapists, and psychologists). Not all localities have such services, and in their absence, a thorough history and clinical assessment should enable a referral to be made to the most appropriate secondary care service. Table 1 and the infographic provide some indicators.
Because health services in many areas are currently very stretched, some patients may experience considerable delays even when their referral meets local criteria. Supportive care and symptom control from the primary care team may be helpful in the interim.
What if I’m not getting better?
Early research on management of post-acute covid-19 assumed (explicitly or implicitly) that patients would recover, albeit slowly. Long covid specialist services in the UK were designed around this assumption and focused on assessment, rehabilitation, occupational therapy, and psychological support. Thirty months into the pandemic, it is clear that this approach helps many but not all patients, and that for a substantial minority, “recovery” currently means developing the ability to manage limited energy, continuing pain, cognitive limitations, and ongoing flare ups in what has become a long term condition.36 In addition to research to characterise persisting forms of long covid and test targeted therapies, models of integrated ongoing care more akin to those for other long term conditions such as diabetes, heart failure, or chronic pain are needed, including evaluating and costing the contribution of primary care to any such service. Community based interdisciplinary services and adequate support and training for healthcare professionals are needed to rapidly improve care and services for the growing numbers of people living with long covid.
Resources for patients
Books
The Long Covid Self Help Guide37—written by specialists at a long covid clinic offering lay explanations and self-management strategies for the different symptom clusters of long covid
Support for rehabilitation: self-management after COVID-19 related illness—a World Health Organization guide for patients20
Long Covid Rehabilitation Booklet from NHS Hertfordshire. https://www.hct.nhs.uk/media/4529/long-covid-rehabilitation-booklet-july-2021.pdf.
Websites
Your Covid Recovery (https://www.yourcovidrecovery.nhs.uk/)—an NHS England funded website with public facing resources (Phase I resources). These offer helpful advice for specific symptoms, eg, dizziness (https://www.yourcovidrecovery.nhs.uk/covid-in-the-last-4-weeks/effects-on-your-body/dizziness/). Phase II Your Covid Recovery is a web based covid-19 rehabilitation programme with healthcare professional support for those referred into the scheme (usually by a rehabilitation professional)
Physiotherapy for Breathing Pattern Disorders (https://www.physiotherapyforbpd.org.uk)—a patient facing site designed and run by specialist physiotherapists
Long Covid Work (https://longcovidwork.co.uk/)—a site for people returning to work after long covid.
Support groups
Long Covid SOS (https://www.longcovidsos.org) and Long Covid Support (https://www.longcovid.org). Examples of resource and networking sites set up by and for people with long covid.
Resources for healthcare professionals
Guidelines
Covid-19 rapid guideline: managing the long term effects of covid-19 (by NICE, Royal College of GPs, and Scottish Intercollegiate Guidelines Network)3
Faculty of Occupational Medicine guidance for health professional on return to work for patients with post-covid syndrome. https://www.fom.ac.uk/wp-content/uploads/FOM-Guidance-post-COVID_healthcare-professionals.pdf
Society of Occupational Medicine’s covid-19 return to work guide for recovering workers. https://www.som.org.uk/COVID-19_return_to_work_guide_for_recovering_workers.pdf
NICE guideline on chronic pain.
E-learning courses
Long term effects of covid-19 and post-covid-19 syndrome: an e-learning resource from the UK Royal College of General Practitioners. https://elearning.rcgp.org.uk/course/view.php?id=492
Health Education England long covid e-learning modules for health professionals. https://www.e-lfh.org.uk/programmes/long-covid/
Online resources
Living maps of covid-19 evidence, created by the UCL EPPI-centre, with long covid segment. http://eppi.ioe.ac.uk/cms/Projects/DepartmentofHealthandSocialCare/Publishedreviews/COVID-19Livingsystematicmapoftheevidence/tabid/3765/Default.aspx
Living systematic review of long covid, which will be updated as new evidence emerges64
Long covid physio: a resource site intended mainly for physiotherapists and their patients, set up by physiotherapists who have (had) long covid. https://longcovid.physio
How patients were involved in the creation of this article
Patients who were members of the LOCOMOTION quality improvement collaborative (see protocol paper for details65) contributed the comments in box 1. RM has lived experience of long covid and co-chairs the patient advisory group for LOCOMOTION. The paper was read by three additional patients with long covid and modified in response to their feedback.
We considered patient led and professionally led research on their merits, aware that many high quality studies on this condition were conceptualised and undertaken by patient communities (who included scientists, social scientists and clinicians, who brought relevant research skills as well as lived experience of long covid).
How this article was created
This paper draws on three sources. The first was a literature search of PubMed using the terms “post-acute covid-19 syndrome (MeSH)”, and “long covid (title and abstract)” and including basic science studies and reviews,11474850 narrative reviews, and conceptual papers considering mechanisms,142426364549526466 clinical trials (of which none had reported at the time of writing), observational studies and reviews of these,15161733344344466267686970 systematic reviews of rehabilitation programmes,71 studies on outcome measures,356061727374 social science studies of long covid in vulnerable groups and underserved communities,525354 surveys121875 and a Delphi study76 of patient priorities, and qualitative studies of the patient experience.213404177 Secondly, the paper drew on group discussions with front line clinicians and patient partners (the LOCOMOTION consortium65) who are members of a national quality improvement collaborative for long covid clinics in the UK (these discussions prompted us to undertake further literature searches where needed). Thirdly, we drew on “grey literature” including service specifications,7879 Office of National Statistics publications,6780 guidelines, and policy documents from the UK and internationally,3556576381 and patient facing self-help literature.2037
{kind=link}
Footnotes
Contributorship and guarantor: The paper draws on the clinical experiences and wisdom of the LOCOMOTION consortium. All authors contributed to the literature search and synthesis of key findings from these. TG wrote the first draft, which was extensively amended by other authors. All authors offered feedback on the infographic. All authors read and approved the final manuscript.
The authors thank patient research participants for the descriptions in box 1, as well as Matthew Knight, Patient Advisory Group members Clare Rayner, Ian Tucker-Bell, and Nikki Smith, and five reviewers (two patients and three clinicians) for helpful comments on an earlier draft.
Competing interests: TG is a member of Independent SAGE. MS is WHO Europe adviser on covid rehabilitation policy and led the development of the C19-YRS (Yorkshire Rehabilitation Scale) outcome measure for long covid. RE and TG are members of the NHS England Task Force for long covid.
Provenance and peer review: commissioned; externally peer reviewed.
This article is made freely available for personal use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usage