
Abstract
PURPOSE We wanted to determine whether an educational intervention targeting general practitioners reduces the 2-year prevalence of depression and self-harm behavior among their older patients.
METHODS Our study was a cluster randomized controlled trial conducted between July 2005 and June 2008. We recruited 373 Australian general practitioners and 21,762 of their patients aged 60 years or older. The intervention consisted of a practice audit with personalized automated audit feedback, printed educational material, and 6 monthly educational newsletters delivered over a period of 2 years. Control physicians completed a practice audit but did not receive individualized feedback. They also received 6 monthly newsletters describing the progress of the study, but they were not offered access to the educational material about screening, diagnosis and management of depression, and suicide behavior in later life. The primary outcome was a composite measure of clinically significant depression (Patient Health Questionnaire score ≥10) or self-harm behavior (suicide thoughts or attempt during the previous 12 months). Information about the outcomes of interest was collected at the baseline assessment and again after 12 and 24 months. We used logistic regression models to estimate the effect of the intervention in a complete case analysis and intention-to-treat analysis by imputed chain equations (primary analysis).
RESULTS Older adults treated by general practitioners assigned to the intervention experienced a 10% (95% CI, 3%–17%) reduction in the odds of depression or self-harm behavior during follow-up compared with older adults treated by control physicians. Post hoc analyses showed that the relative effect of the intervention on depression was not significant (OR = 0.93; 95% CI, 0.83–1.03), but its impact on self-harm behavior over 24 months was (OR = 0.80; 95% CI, 0.68–0.94). The beneficial effect of the intervention was primarily due to the relative reduction of self-harm behavior among older adults who did not report symptoms at baseline. The intervention had no obvious effect in reducing the 24-month prevalence of depression or self-harm behavior in older adults who had symptoms at baseline.
CONCLUSIONS Practice audit and targeted education of general practitioners reduced the 2-year prevalence of depression and self-harm behavior by 10% compared with control physicians. The intervention had no effect on recovery from depression or self-harm behavior, but it prevented the onset of new cases of self-harm behavior during follow-up. Replication of these results is required before we can confidently recommend the roll-out of such a program into normal clinical practice.
BACKGROUND
Depression is a common and disabling disorder that affects people of all ages1–4 and about 5% to 10% of adults older than 60 years.5,6 Recent attempts to reduce the prevalence of depression in the community have focused on improving the identification of people with depression7–11 and on increasing the efficacy of existing management strategies.12,13 Screening and case finding are the approaches most frequently used to identify people with depression in populations at risk, particularly in general practice settings. A meta-analysis of 16 randomized trials, however, found that the systematic use of screening instruments or case-finding procedures increased the recognition of depression by 27% but had no effect on the adoption of treatments or the outcome of patients.14
The evidence in support of the use of educational interventions targeting general practitioners to reduce the prevalence of depression and suicidal behavior remains inconclusive. Gilbody et al15 suggested that interventions incorporating clinician education, case management, and integration between primary and secondary care have a greater chance of being effective than interventions limited to education.16,17 For example, the Improving Mood—Promoting Access to Collaborative Treatment (IMPACT) trial recruited more than 1,800 older adults with major depression or dysthymia who were randomly assigned to usual care or an intervention that included supervised case management, education, support of antidepressant use, and brief problem solving therapy.18 After 12 months, 45% of patients in the intervention group had improved compared with only 19% of those receiving usual care (OR = 3.4; 95% CI, 2.7–4.4). A similar reduction in suicidal ideation was observed.19 Other trials using collaborative care models to manage older adults with depression treated in primary care settings have reported similarly encouraging results,20–22 although gains were modest and the costs high.23,24 In addition, most published studies to date have had relatively small sample sizes and imprecise effect estimates, uncertain sustainability of the intervention in normal clinical practice, and inability to generalize these findings to the entire population of older adults reviewed in primary care.
The Depression and Early Prevention of Suicide in General Practice (DEPS-GP) trial was conceived to ascertain the effect of a simple and sustainable clinician-based education intervention and practice audit on the prevalence of depression and self-harm behavior in a large sample of primary care patients aged 60 years or older. Unlike previous trials,18,21 the DEPS-GP intervention targeted general practitioners and collected information on mental health outcomes from a nonselected group of their primary care patients. Our hypothesis was that older adults treated by the physicians in the intervention group would have a lower prevalence of a composite measure consisting of clinically significant depressive symptoms or self-harm behavior than the patients of control physicians.
METHODS
Trial Design
The DEPS-GP project was an open label, parallel, clustere-randomized trial with a 1-to-1 allocation ratio of general practitioners to a targeted and nontargeted educational intervention about depression and self-harm behavior. The Ethics Committees of the University of Western Australia, the University of Melbourne, and the Royal Australian College of General Practitioners approved the study protocol, and all participants provided informed consent. The study was conducted in accordance with the declaration of Helsinki and registered with the Australian New Zealand Clinical Trials Registry under the ACTR number 12605000049673 on July 25, 2005.
Participants
We posted a one-time invitation to take part in the study to 19,046 general practitioners listed on the Australasian Medical Publishing Company Proprietary Limited database and practicing in the Australian states of Western Australia, South Australia, Victoria, New South Wales, and Queensland. The accuracy and completeness of this list are unknown. There were 772 physicians who replied to our invitation, and 373 agreed to recruit adults aged 60 years or older for the study. Details about the recruitment process have been described elsewhere.25 We started recruitment in July 2005 and completed the collection of endpoints in June 2008.
Intervention
Participating physicians were the target of the intervention, which consisted of 3 components: (1) printed educational material about practical aspects of the assessment and management of depression and self-harm behavior in later life, (2) practice audit of 20 active patients with detailed personalized audit feedback that took place within the first 6 months of the study, and (3) newsletters outlining progress of the study. The newsletters were posted to participating physicians 6, 12, and 18 months after randomization.
Physicians participating in the educational activities of the project accrued points for the maintenance of professional standards.
Twenty consecutive patients aged 60 years or older attending the practice during the 4-week audit period were given a self-rating questionnaire by the receptionist at the time of their arrival at clinic. They were asked to record the date of the visit, their date of birth, sex, birthplace, marital status, and educational attainment, and to complete the 9-item Patient Health Questionnaire (PHQ-9) and the and the Depressive Symptom Index Suicidality Subscale (DSI-SS).
We used the PHQ-9 to assess depressive symptoms among the study patients.26 The PHQ-9 consists of 9 questions about how often the respondent has been bothered by depressive symptoms during the past 2 weeks, and each item can be scored 0 (“not at all”), 1 (“several days”), 2 (“a week or more”) or 3 (“nearly every day”). A total score of 10 or more indicates the presence of clinically significant depression.27 The DSI-SS is a 4-item self-report questionnaire designed to identify the frequency and intensity of suicidal ideation and impulses in the previous 2 weeks. Scores for each item of the DSI-SS range from 0 to 3, with higher scores reflecting greater severity of suicidal ideation. Past work has supported the scale’s psychometric properties.28–30 Patients returned the questionnaires to the practice receptionist before their medical appointment.
After each of the 20 consultations reviewed during the audit period, each physician was asked to complete a 1-page summary sheet, which contained the following qustions: “Did you screen for mental health problems during this consultation? (yes/no),” “What is the likelihood that s/he was depressed? (high/medium/low-none),” “Did you ask about suicide risk? (yes/no),” and “What was the suicide risk estimation? (high/medium/low-none).” We also asked the about the proposed management plan after the consultation: physician counseling (yes/no), referral to general hospital (yes/no), psychiatric hospital (yes/no), public mental health service (yes/no), private mental health service (yes/no), involvement of family or relevant others (yes/no), and prescription of antidepressant medication (yes/no), including the name of the antidepressant.
Physicians assigned to the educational intervention received detailed written audit feedback, which included a description of the number of patients with depression in their practice audit compared with other participating practices; the number of patients with depression and self-harm ideation (based on the PHQ algorithm developed by Spitzer and colleagues31 and a DSI-SS score of 1 or greater in any of the 4 screening items for self-harm) that they correctly identified compared with control physicians; the sex, date of birth, and specific symptoms of depression reported by each person with depression in their practice audit; and similar information for suicidal ideation. The also received educational material focused on the assessment and diagnosis of depression, identifying and managing suicidal risk in older adults, using antidepressant medication with this age-group, and crisis support contact information. Moreover, audit feedback directed physicians in the intervention group to relevant sections of the educational material.32
The newsletters posted to intervention physicians described the general information presented to the control group, as well as information about the signs and symptoms of depression most frequently found among older adults within the study, screening tips for uncovering depression and suicide risk, and case studies that provided cross-referencing to the educational material posted during the audit.
Physicians randomly assigned to the control group did not receive the printed education material, but they completed a practice audit and were mailed newsletters. In this case, audit feedback was limited to pooled data (ie, number of older adults with depression or suicidal ideation within their practice audit and across all participating physicians, and the proportion correctly identified within their practice and the study in general). Similarly, the newsletters posted to physicians in the control group were limited to general information about the number of physicians and older adults involved in the study, their demographic characteristics, and a snapshot of the interventions employed for treating depression.
Outcomes
The primary outcome of interest of this study was a composite measure of self-harm behavior or clinically significant depression (PHQ-9 ≥10) recorded 12 or 24 months after recruitment.
We asked the study patients, “How often have you attempted suicide or intentionally harmed or injured yourself in the past year?” Possible answers were no, once, or more than once. We also asked them, “Have you thought about or attempted to kill yourself in the past year?” Possible answers were no or yes. We considered that self-harm behavior (ie, suicide ideation or attempt during the past year) was present in the past year if participants did not reply no to both questions.
Other Measures
Patients recorded the dates of assessment and birth, sex, place of birth, marital status, living arrangements, educational achievement, physical activity, smoking status, risky alcohol use, self-reported medical morbidities from a list of common morbidities, and history of physician diagnosis of depression. We used self-reported information on weight and height to calculate the body mass index (kg/m2), and the Duke Social Support Index as a measure of social support.33
We recorded information about the number of audits completed by participating physicians, self-reported use of antidepressants during the preceding 12 months, contact with mental health professionals, and support from family and friends to deal with health problems (nonspecified support) during the preceding 12 months. We retrieved medication data from the list of medications (prescription and nonprescription) provided by physicians at the 24-month assessment.
Possible Factors Mediating the Effect of the Intervention on Outcomes
We asked patients at the 12 and 24-month assessments whether they had received (1) antidepressant treatment during the preceding 12 months; (2) assessment or treatment from a psychiatrist, psychologist, or counselor in the preceding 12 months; and (3) any other form of support for health problems (including anxiety and depression) from non–health professionals (this last question was only asked at the 24-month assessment). In addition, we recorded the number of audits completed by each participating physician and considered that a minimum of 10 audits should have been completed (ie, 50%) to indicate compliance with the study protocol.
Sample Size
At trial registration, we had hoped to power the study to measure the effect of the intervention on suicide attempts over 2 years. As the number of consenting physicians was lower than the required 480, we had to create a new primary outcome measure to achieve sufficient power. This new measure was a composite of clinically significant depressive symptoms (PHQ-9 ≥10) or self-harm behavior. We calculated that we would need to recruit 21,600 older adults (or about 310 physicians; power 80%, α = .05). Assuming a loss to follow-up of about 15% to 20%, we aimed to recruit 372 physicians into the study. We recruited 373.
Randomization
The randomization procedure took place after the recruitment of physicians and their patients was finalized. Those who consented were randomly assigned to the intervention or control condition according to a list of random numbers generated by computer in blocks of 24 physicians, with equal numbers allocated to each study group. To decrease the risk of contamination, physicians working at the same practice received the same randomization number.
Statistical Methods
The data were managed and analyzed with Stata 11.1 (StataCorp). We used cross-tabulations to determine the distribution of covariates according to group assignment (Pearson’s χ2 statistic).
We compared the proportion of patients in the intervention and control groups who met criteria for the primary composite outcome measure at either the 12- or the 24-month assessment; the same analysis was repeated separately for depressive symptoms and self-harm behavior. We used logistic regression (population average estimation) to examine the association between these outcomes and the intervention taking into account the baseline value of each outcome and relevant confounding variables.
We then stratified the analyses according to the presence or absence of depression or self-harm behavior at baseline. The data were organized with older adults at level 1 nested within practices/physicians at level 2. Our initial analyses took into account the effect of clustering by practice and then by physician, but both were later dropped because their impact on the statistical models proved to be negligible (intraclass correlation coefficient ≤0.01).
We applied imputation by chained equations to complete an intention-to-treat (ITT) analysis of the outcomes of interest (primary analysis). Older adults who died during follow-up were not included in the ITT analysis, as they could not possibly meet criteria for an endpoint of interest for the study. All variables available at baseline contributed information to calculate the missing values for the imputation files. We generated 5 imputed data sets to achieve stable estimates and 95% confidence intervals; α was set at .05, and all statistical tests reported are 2-tailed.
RESULTS
Outcomes of Interest
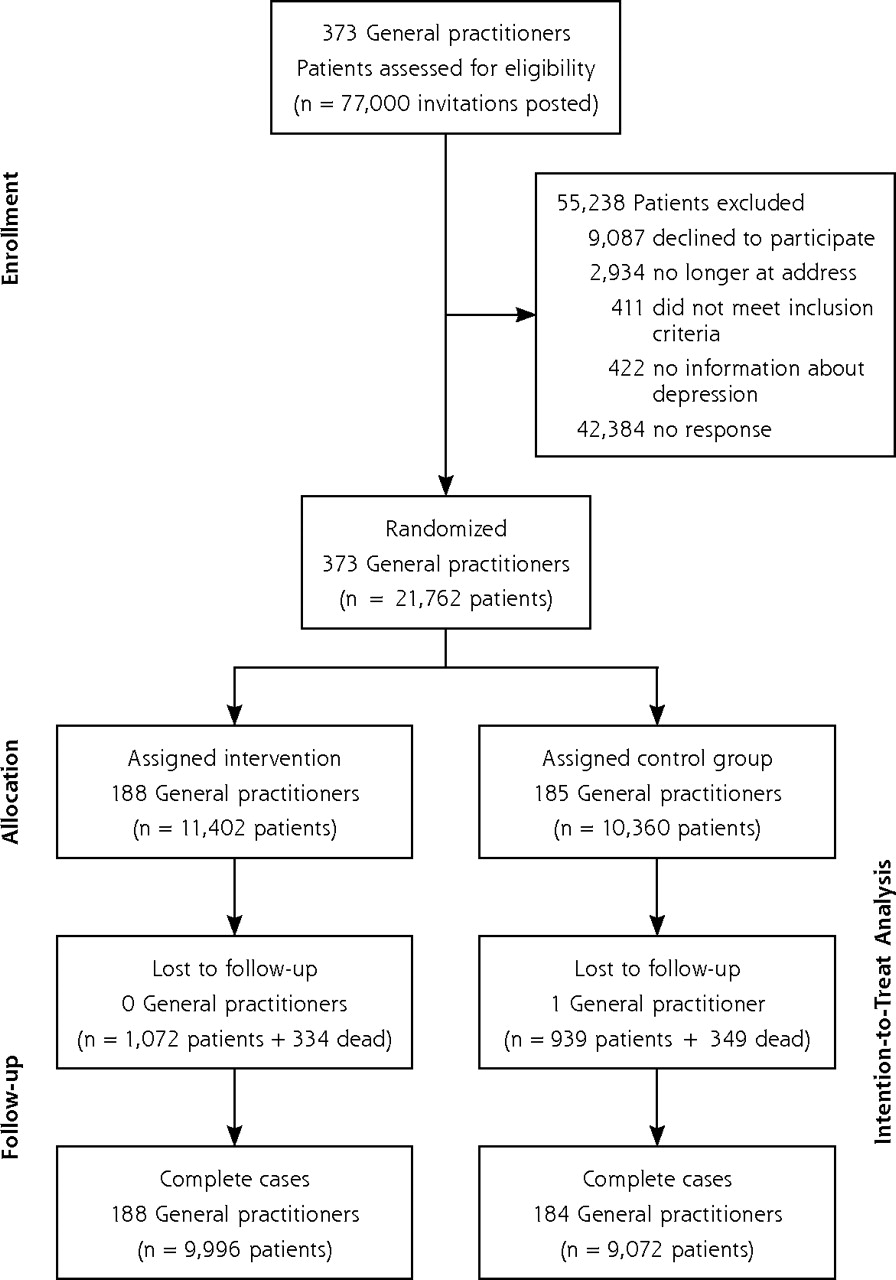
A total of 77,000 invitations, together with a reply-paid envelope, were sent to all patients aged 60 years or older listed in these practices (average of 203 patients per physician): 42,384 did not respond, 9,087 patients declined to participate, 2,934 were returned as “not known at this address,” 411 did not meet the inclusion criteria (aged younger than 60 years or not reported), and 422 patients were excluded because of incomplete information on depressive symptoms and self-harm behavior, leaving a total study sample of 21,762 adults aged 60 years or older. Figure 1 shows the flow of study patients during the trial. The average number of patients recruited per participating physician was 58.5 (median = 44, interquartile range = 21–82, minimum-maximum = 1–300).
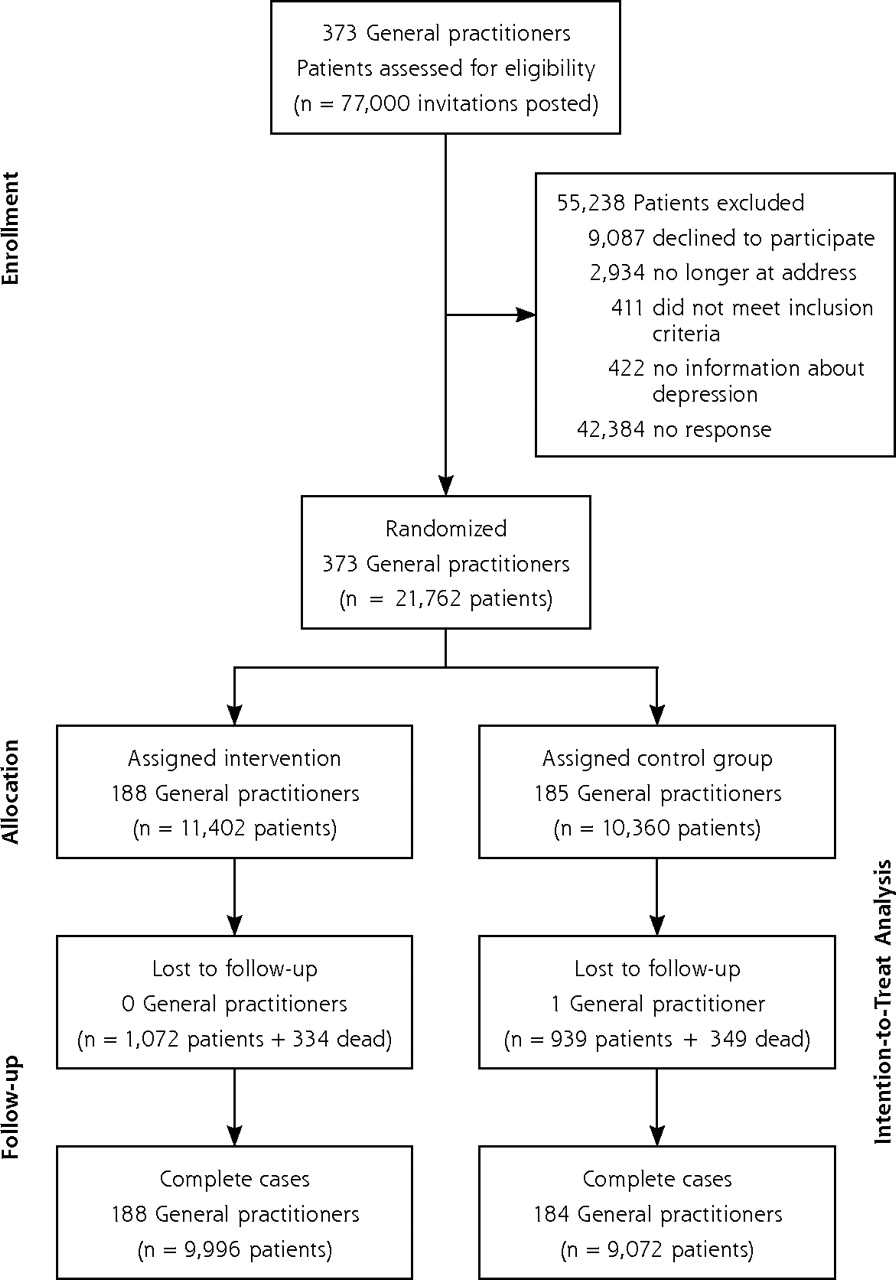
Flow of general practitioners and their patients from enrollment until final collection of trial outcomes after 2 years.
The mean age of patients was 71.8 years (range = 60–101 years), and those under the care of physicians in the intervention group were 0.5 years younger than those treated by physicians in the control group (P <.001). There were more women than men in the sample (58.8%), and a larger proportion were under the care of control physicians. Table 1 summarizes the demographic, lifestyle, and clinical characteristics of participating patients at the baseline assessment according to the allocation group of their physicians.
Baseline Demographic, Lifestyle, and Clinical Characteristics of Older Adults, by General Practitioner Study Group
Older adults treated by physicians assigned to the intervention group were 10% (95% CI, 3%–17%) less likely than assigned to the control group to experience the composite primary outcome (ITT, Table 2). The effect of intervention on depression (PHQ-9 ≥10) was not significant (OR = 0.93; 95% CI, 0.83–1.03), but its impact on suicide ideation/attempt over 24 months was significant (OR = 0.80; 95% CI, 0.68–0.94).
Patients With Clinically Significant Depression, Self-Harm Behavior, or Both (Composite) During Follow-up (12 or 24 Months), by General Practitioner Control (n = 10,360) and Intervention (n = 11,402) Study Group
We then completed a series of post hoc analyses to clarify whether the intervention had a measurable effect on the onset of depression and self-harm behavior among those who were free of these symptoms at baseline (Table 3). Older adults treated by intervention physicians had lower odds of reporting self-harm behavior during follow-up than those treated by control physicians (adjusted OR = 0.80; 95% CI, 0.66–0.96), although the effect was not significant for depressive symptoms (adjusted OR = 0.90; 95% CI, 0.79–1.03). The intervention had no effect on 24-month recovery from depression or self-harm behavior in older adults who displayed these symptoms at baseline (Table 3).
Outcomes for Older Adults Treated by General Practitioners in Control and Intervention Groups, by Depression or Self-Harm Behavior at Study Entry
Secondary Analyses
We investigated a number of factors that could have mediated the effect of the intervention on the outcomes of interest. Table 4 summarizes these results. A larger proportion of intervention compared with control physicians completed a minimum of 10 audits (OR = 1.34; 95% CI, 1.25–1.43). Patients in the intervention group did not report greater use of antidepressant medications or contact with mental health professionals than older adults treated by control physicians. Likewise, there was no difference between the groups regarding the proportion of patients receiving other types of support (Table 4).
Patients Who Engaged in Activities That Could Have Modified Symptoms of Depression or Suicide Ideation or Behavior at Follow-up, by General Practitioner Study Group
DISCUSSION
The results of this trial show that an educational intervention targeting general practitioners reduced the prevalence of a composite measure of clinically significant depression or self-harm behavior. The effect of the intervention was modest (3% to 17% reduction in the odds of having these symptoms at 24 months).
Our findings were derived from a clustered randomized trial that kept loss to follow-up during the 2 years within acceptable limits (15.6% of patients) and recruited a sample size that was sufficiently large to detect small but meaningful clinical effects associated with the intervention. Although we used well-validated instruments and procedures to collect information about outcomes of interest,31 we acknowledge that our definition of depression was not based on a structured clinical interview, and that self-reported data about the 12-month diagnosis of depression and self-harm behavior were not externally validated. This type of error would not have biased the results of the trial (because error would have been randomly distributed), but it might have affected the measured effect-size of the intervention. In addition, because both groups of physicians participated in audit and feedback, which are activities that can change professional practice,37 we cannot dismiss a possible intervention effect in control physicians. As the process measures did not show any obvious change in the behavior of participating physicians regarding, for example, the prescription of antidepressants, it seems improbable that our results would have been affected in this way. Another limitation of our study design is that participating physicians were motivated volunteers rather than a random sample of practicing physicians, which creates some uncertainty as to whether the program would have been equally successful for the patients of physicians who chose not to participate in this trial. Because physicians with limited interest in mental health may benefit the most from this type of educational program,38 one would hope that the effect of the intervention would have been even greater in a nonselected sample of general practitioners.
We also acknowledge that our follow-up of patients was limited to 24 months, and it is unclear whether the modest effect of the intervention could have been sustained for a longer period. Furthermore, the patients of the 2 groups of physicians were not well balanced for some important variables associated with depression and self-harm behavior, such as age, sex, and living arrangements. We attempted to minimize the impact of such imbalance by forcing these variables into our statistical models, although residual error could have persisted and led to an inflation of our effect estimates.
Finally, we did not validate the self-reported information provided by participants regarding the number of consultations with their physicians and their use of health services during the 12 months leading up to the final assessment.
Previous studies investigating the effect of educational interventions that target general practitioners with the aim of reducing the prevalence of depression among their patients have produced mostly negative results. Data from the Hampshire Depression Project showed that, compared with control physicians, training to assess and manage depression did not improve detection or the outcome of patients with depression after 6 weeks and 6 months (n = 4,192).16 A similar Dutch study reported that the 3-month outcome of 498 patients with depression treated by intervention general practitioners was better than the outcome of patients treated by control general practitioners, but the small differences between the groups were no longer apparent after 12 months.17 These 2 studies focused on the outcome of primary care adult patients who were displaying clinically significant symptoms of depression, and their negative results are entirely consistent with our own. Together, these findings confirm that the depressed patients of general practitioners who participate in educational activities about depression do not have a better medium- to long-term outcome than the patients of general practitioners who do not take part in such activities.
We offered our intervention physicians education about screening, diagnosing, and managing depression as well as self-harm behavior. We found no evidence that participation in such activities decreased the prevalence of depression in a nonselected sample of patients, but we did find that older adults treated by intervention physicians were less likely to display self-harm behavior than their counterparts treated by control physicians. These results could not be adequately explained by more frequent use of antidepressants or contact with mental health professionals. It is possible that they were the product of chance (type I error), although other unmeasured factors could potentially explain these findings. For example, there is some evidence that patients of general practitioners randomly assigned to similar educational activities have a more positive view of their physicians, with at least one study showing that these physicians were perceived as having greater understanding of patients’ feelings and emotions.39 Interestingly, the study by Gask and colleagues39 also found that the patients of intervention general practitioners had better health perception and less role limitation caused by mental distress after 12 months than did the patients of control general practitioners, even though the groups showed no obvious difference on depression scores. These results suggest that education about depression and its treatment may improve the attitude of physicians toward mental health issues, which may lead to nonspecific better health outcomes for patients. The results of the Gotland educational program are consistent with such an interpretation.
In the early 1980s the Swedish Committee for Prevention and Treatment of Depression implemented an educational package about the diagnosis and treatment of depression for all general practitioners working on the island of Gotland.40 There is no published evidence that the program reduced the prevalence of depression in Gotland, but the rates of completed suicide dropped dramatically during the subsequent 2 years: from 22 in 100,000 per year to 14.3 and 7.1 in 100,000 per year, respectively (the Gotland study was nonrandomized and without a contemporaneous control group).40 Because suicide behavior is closely associated with depression in later life,41,42 we had anticipated that changes in suicide ideation or behavior would be due to better treatment of depression in this population. Our results show that such is not the case and suggest that other factors (eg, a physician’s empathy and willingness to discuss the emotional concerns of patients) may play a more important role than depression in reducing self-harm ideation in this age-group. In fact, there is evidence that the relationship between patients and their primary care physicians has therapeutic value and, like social interventions, improves outcomes in a way that is different from formal treatments (such as medications).43,44
It is important to note that our intervention did not decrease the prevalence of depression or self-harm behavior. Instead, the prevalence of self-harm behavior increased slightly, but disproportionally, in control group patients, which seems to have been the main reason for the observed difference between the groups. It is unclear what might have caused these changes, but they were either due to unmeasured factors (eg, increased exposure to stress)45 or to the repeated questioning that allowed participants to feel progressively more comfortable to disclose their suicidal ideation. Another possibility is that asking about suicide intent increases the frequency of thoughts of self-harm, although existing data are not consistent with such interpretation.46 It is also possible that at study entry all participating physicians had a similar state of alertness to the need of screening and managing self-harm ideation, and that the activities of the project contributed to maintain or heighten such a state among intervention and control physicians during the follow-up period. Nonetheless, we concede that type I error could plausibly explain our findings, so that replication of these results is required before we can confidently recommend the roll out of such a program into normal clinical practice.
Acknowledgments
The investigators thank participants and research staff for their generous contributions.
Footnotes
-
Conflicts of interest: none reported.
-
Funding support: The study was supported by the project grant number 353569 from the National Health and Medical Research Council of Australia (NHMRC) to Almeida, Pfaff, Kerse, Pirkis, Goldney, and Snowdon, and by an infrastructure grant from beyondblue Australia.
-
Disclaimer: The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
- Received for publication June 16, 2011.
- Revision received October 17, 2011.
- Accepted for publication November 2, 2011.
- © 2012 Annals of Family Medicine, Inc.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- Improving the management of self-harm in primary care
- Discussing suicidality with depressed patients: an observational study in Dutch sentinel general practices
- RAndomised controlled trial to imProve depressIon and the quality of life of people with Dementia using cognitive bias modification: RAPID study protocol
- Targeted education for general practitioners reduces risk of depression or suicide ideation or attempts in older primary care patients
- Factors associated with suicidal thoughts in a large community study of older adults
- Targeted education for general practitioners reduces risk of depression or suicide ideation or attempts in older primary care patients
- In This Issue: An Abundance of Interventions and Observations to Improve Care