
Abstract
PURPOSE Little information is available on multimorbidity in primary care in India. Because primary care is the first contact of health care for most of the population and important for coordinating chronic care, we wanted to examine the prevalence and correlates of multimorbidity in India and its association with health care utilization.
METHODS Using a structured multimorbidity assessment protocol, we conducted a cross-sectional study, collecting information on 22 self-reported chronic conditions in a representative sample of 1,649 adult primary care patients in Odisha, India.
RESULTS The overall age- and sex-adjusted prevalence of multimorbidity was 28.3% (95% CI, 24.3–28.6) ranging from 5.8% in patients aged 18 to 29 years to 45% in those aged older than 70 years. Older age, female sex, higher education, and high income were associated with significantly higher odds of multimorbidity. After adjusting for age, sex, socioeconomic status (SES), education, and ethnicity, the addition of each chronic condition, as well as consultation at private hospitals, was associated with significant increase in the number of medicines intake per person per day. Increasing age and higher education status significantly raised the number of hospital visits per person per year for patients with multiple chronic conditions.
CONCLUSION Our findings of higher prevalence of multimorbidity and hospitalizations in higher SES individuals contrast with findings in Western countries, where lower SES is associated with a greater morbidity burden.
INTRODUCTION
Multimorbidity, the co-occurrence of 2 or more (chronic) conditions within the same individual, is linked to higher health care use, higher expenditure, and impaired quality of life.1–3 In the developing countries, little information on multimorbidity is available and is based on secondary data and limited to a only a few chronic conditions and geriatric groups.4–6 With our previous study, for which data were based on the World Health Organization (WHO) Study on Global Aging and Adult Health (SAGE), we reported a 8.9% prevalence of multimorbidity in Indian adults.7 Our systematic review on multimorbidity in South Asia found a lack of uniformity in the definition and assessment of multimorbidity, and no information from primary care in India.8 Given the importance of primary care for delivering coordinated chronic care, and that primary care being the first contact for most populations in India, it is important that we understand the magnitude of multimorbidity in these settings. We therefore undertook this first study to estimate the prevalence of multimorbidity among adult patients attending public and private primary care and to examine the socioeconomic correlates and health care use. The study was exploratory; we restricted it to Odisha, an Indian state (approximate population share of 4% of the total population of India) with average health indicators and comparable health system characteristics.9
METHODS
We conducted a cross-sectional study from October 2013 to March 2014 on 1,670 adult patients from 40 primary health care facilities (20 public and 20 private) by using a multistage, stratified random sampling. Participants were interviewed by 4 trained nurses using a structured multimorbidity assessment protocol (MAP). The 22 included health conditions (Supplemental Appendix at http://www.annfammed.org/content/13/5/446/suppl/DC1) were based on an extensive literature search followed by a chart review of the most frequent chronic conditions encountered in primary care. The 9-item Patient Health Questionnaire (PHQ-9) was used for ascertaining depression (a cutoff score of 10 or more was considered to be positive for depression).10,11 Additionally, we elicited health care use in terms of number of outpatient visits and inpatient admissions in the last 12 months per person per year and count of medications per person per day. The study was approved by the Institutional Ethics Committee of Public Health Foundation of India, New Delhi.
We defined multimorbidity as having 2 or more chronic conditions. We calculated age- and sex-adjusted prevalence across sociodemographic variables and used binary logistic regression analysis to estimate adjusted odds of association of various sociodemographic correlates with multimorbidity. A trend test was performed to investigate whether the probability of having multiple chronic morbid conditions varied across the age-group and by sex. Within multimorbidity, the associated factors for health care use were explored using negative binomial regression analysis and expressed as incidence rate ratio (IRR).
RESULTS
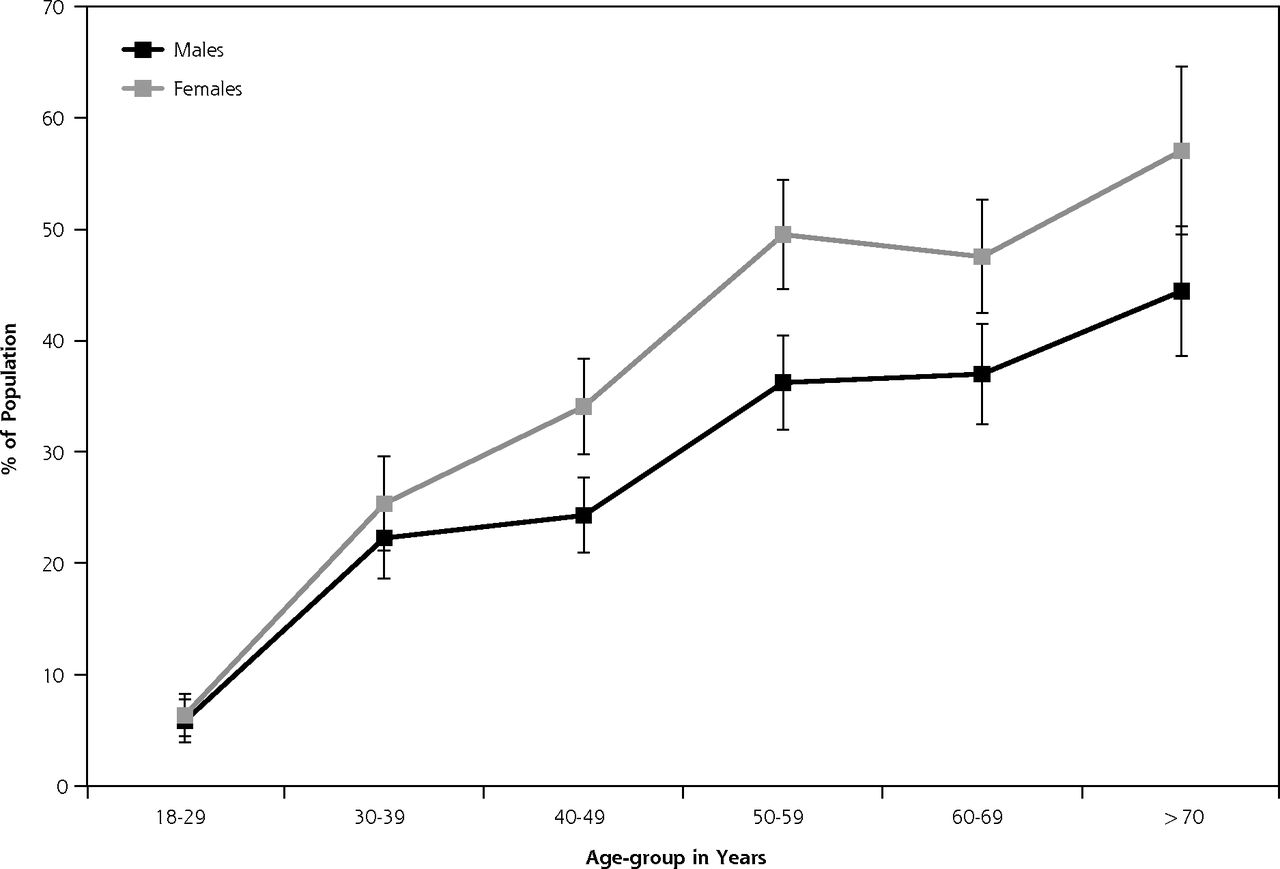
Of 1,649 patients interviewed, more than one-half (54.7%) had at least 1 chronic condition, and 28.3% had more than 1 chronic condition (Table 1). The prevalence of multimorbidity ranged from 5.8% in patients aged 18 to 29 years to 44.4% in patients aged 70 years and more (χ2 for trend = 12.12, P <.001) (Figure 1). Patients had higher odds of having multiple morbidities if they were of older age, female, of higher socioeconomic status, and nonaboriginal; if they had high levels of education; and if they were visiting private health care facilities (Table 1). The mean number of hospital visits per patient per year was 1.62 (95% CI, 1.31–1.93) and 2.81 (95% CI, 2.34–3.28) among patients with single chronic conditions and multimorbidities, respectively. The mean number of medicine used increased from 0.56 (95% CI, 0.50–0.62) among patients with single chronic conditions to 1.17 (95% CI, 1.04–1.29) among patients with multimorbidities. Among patients with multimorbidities, the number of medicines taken was 1.39 times higher among those attending private health care facilities than those visiting public facilities (Table 2). Each additional chromic condition was expected to increase the number of medicines taken by 1.30 times after adjusting for other variables in the model. Increasing age and level of education, however, were significantly associated with higher number of hospital visits (Table 2).
Multimorbidity Prevalence and Its Association With Different Sociodemographic Characteristics: Results From Univariate and Multivariate Analyses (N = 1,649)
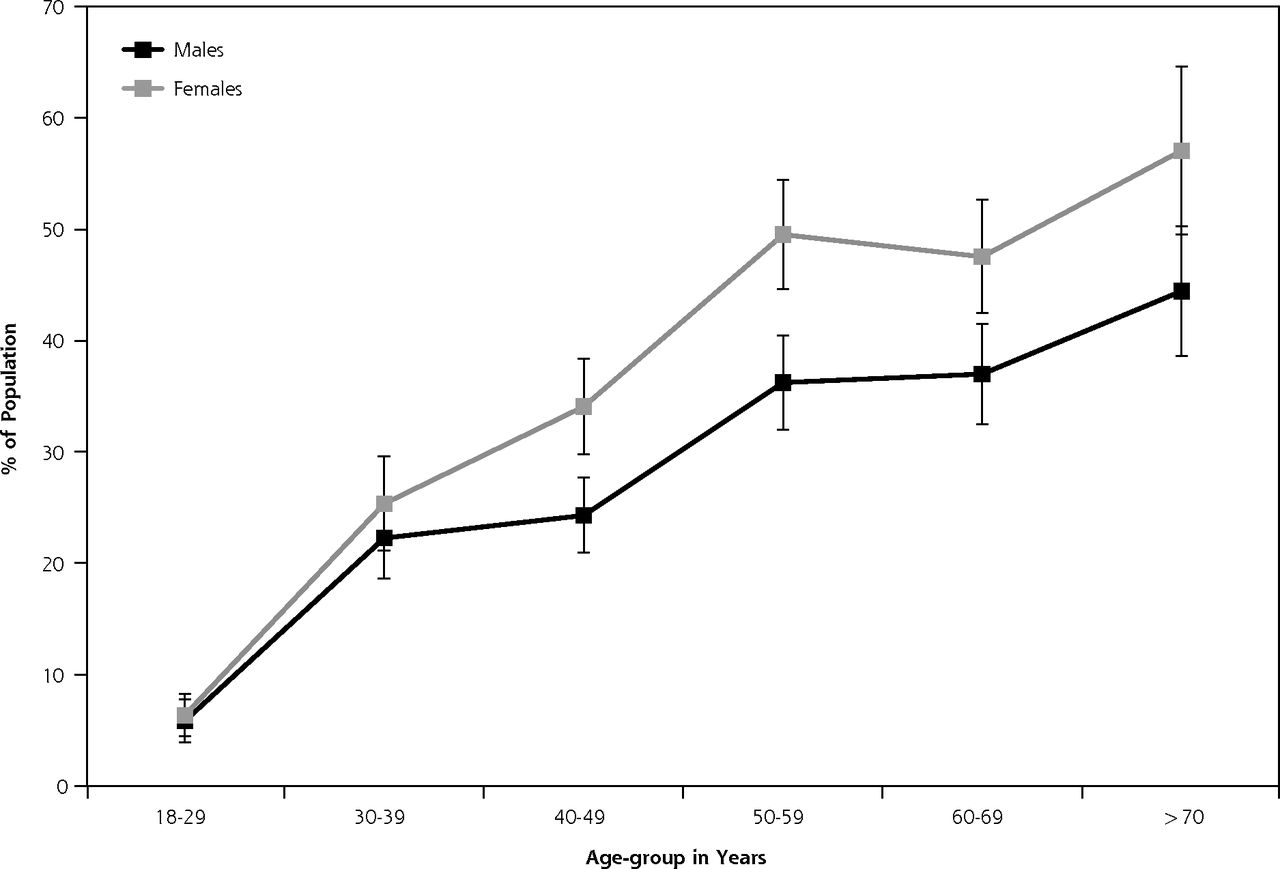
Percentage of population with more than 1 chronic condition, by age and sex.
Negative Binomial Regression Showing Factors Influencing Health Care Use Within Patients With Multiple Morbidities
DISCUSSION
Using a broad nosological spectrum, we found the prevalence of multimorbidity to be 28.3%, similar to that reported for other high- and middle-income countries.12–14 This rate is higher than our previous findings,7 which could be due to a difference in the number of conditions included to define multimorbidity.15 The higher likelihood of multimorbidity among older adults, women, and those with higher income level is congruent with findings from studies from South Asia.4,6 The observed inverse correlation between socioeconomic status and multimorbidity, though, contrasts with that of Western countries, but it is consistent with previous findings from India.7,16 Such a strong correlation of higher SES with increased multimorbidity could be attributed to apparently contrasting socioeconomic patterns of risk factors for noncommunicable diseases in India, as well as in other developing countries,17 compared with developed countries. Low health care–seeking behavior and probability of underdiagnosis among low-income populations could be one possible explanation.18
As with our previous findings, we observed an increase in the number of medicines taken with the increasing number of chronic conditions.2 The significant association between older age and higher education with a higher number of hospital visits could be attributed to increased health literacy among the patients.19
Overall, our observations indicate multimorbidity to be a prevalent phenomenon among Indian primary care patients and provide novel epidemiological evidence of its magnitude and impact on health care use for one Indian state. These observations have not previously been explored in such detail. Because of the methodology used, our prevalence estimates, even though from a single province, reflect closely the multimorbidity in Indian primary care. Our finding suggests redesigning the current national health programs that focus on single diseases to address multimorbidity more effectively, with particular attention to primary care strengthening and developing contextualized health care protocols.
Acknowledgments
We sincerely thank the Department of Health and Family Welfare, Government of Odisha, for their valuable support. We are also thankful to Indian Medical Association, Odisha branch, and all medical officers and private practitioners for facilitating data collection. We are grateful to all study participants for providing valuable information and sharing their experiences.
Footnotes
Conflicts of interest: authors report none.
Previous presentation: Presented at WONCA South Asia Conference-2014; August 16–17, 2014; Chennai, India.
Funding support: This work was supported by a Wellcome Trust Capacity Strengthening Strategic Award to the Public Health Foundation of India and a consortium of UK universities.
Disclaimer: The sponsors of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/5/446/supplDC1/
- Revision received July 12, 2015.
- Accepted for publication November 21, 2014.
- Accepted for publication July 21, 2015.
- © 2015 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Sex differences in non-communicable disease multimorbidity among adults aged 45 years or older in India
- Household and area determinants of emergency department attendance and hospitalisation in people with multimorbidity: a systematic review
- Community prevalence and dyad disease pattern of multimorbidity in China and India: a systematic review
- Identifying non-communicable disease multimorbidity patterns and associated factors: a latent class analysis approach
- Magnitude, pattern and correlates of multimorbidity among patients attending chronic outpatient medical care in Bahir Dar, northwest Ethiopia: the application of latent class analysis model
- Prevalence of non-communicable chronic conditions, multimorbidity and its correlates among older adults in rural Nepal: a cross-sectional study
- Physical multimorbidity patterns and depressive symptoms: a nationwide cross-sectional study in Japan
- Prevalence and correlates of cardiometabolic multimorbidity among hypertensive individuals: a cross-sectional study in rural South Asia--Bangladesh, Pakistan and Sri Lanka
- Contextual and individual inequalities of multimorbidity in Brazilian adults: a cross-sectional national-based study
- Pattern, correlates and implications of non-communicable disease multimorbidity among older adults in selected Indian states: a cross-sectional study
- Multimorbidity prevalence and pattern in Indonesian adults: an exploratory study using national survey data
- In This Issue: Generalist Care Around the World