
Abstract
PURPOSE A culture of blame and fear of retribution are recognized barriers to reporting patient safety incidents. The extent of blame attribution in safety incident reports, which may reflect the underlying safety culture of health care systems, is unknown. This study set out to explore the nature of blame in family practice safety incident reports.
METHODS We characterized a random sample of family practice patient safety incident reports from the England and Wales National Reporting and Learning System. Reports were analyzed according to prespecified classification systems to describe the incident type, contributory factors, outcomes, and severity of harm. We developed a taxonomy of blame attribution, and we then used descriptive statistical analyses to identify the proportions of blame types and to explore associations between incident characteristics and one type of blame.
RESULTS Health care professionals making family practice incident reports attributed blame to a person in 45% of cases (n = 975 of 2,148; 95% CI, 43%–47%). In 36% of cases, those who reported the incidents attributed fault to another person, whereas 2% of those reporting acknowledged personal responsibility. Blame was commonly associated with incidents where a complaint was anticipated.
CONCLUSIONS The high frequency of blame in these safety, incident reports may reflect a health care culture that leads to blame and retribution, rather than to identifying areas for learning and improvement, and a failure to appreciate the contribution of system factors in others’ behavior. Successful improvement in patient safety through the analysis of incident reports is unlikely without achieving a blame-free culture.
INTRODUCTION
In the international agenda for patient safety, incident reporting systems are critical engines for learning.1,2 For those who report safety incidents, however, fear of blame is a recognized barrier in all safety-critical industries that seek to use the analysis of incidents as a method for improvement.1–7 The extent of blame attribution within incident reports themselves is unknown. Underreporting is the norm, and it has been estimated that reporting systems detect only 10% of adverse events in hospitals.8 Such underreporting represents a major missed opportunity to understand errors and prevent harm.
The patient safety movement is based on the premise that patient safety incidents are largely the result of poorly designed systems.9 Even so, our previous study of primary care incident reports suggests that those who report such incidents focus heavily on describing the shortcomings of the individuals (staff, patients, families, caregivers) involved without considering system failings.10 In a minority of situations, where there is willful misconduct or negligence, it is appropriate that individual accountability should be enforced.11 The political and media climates in many countries, however, too often demand that individuals are held responsible regardless of the reason.1,12,13 Where there is blame and finger-pointing, the opportunity for shedding light on the real explanation for serious incidents is lost. Fear of blame is a major barrier to both participation in incident reporting and to promoting an underlying safety culture in health systems.1,6
Most patient safety studies have been in hospital populations, yet globally, primary care manages up to 90% of all patient contacts.14 Primary care lags behind secondary care in generating learning from incident reports15 and has additional challenges when it comes to reporting patient safety concerns. For example, a report on whistle-blowing in a family practice emphasized how difficult it is to report confidentially or anonymously when working in small clinical teams.16 In addition, a potential immediate employer may be personally involved in the safety incident. Accordingly, we set out to examine a sample of patient safety incidents reported from primary health care settings within a publicly funded health care system. The aim of our study was to identify and classify the types of statements of attributed blame made within the reports and to relate them to the nature of the incidents.
METHODS
Data Source
We analyzed data taken from the National Reporting and Learning System, a database of 14 million patient safety incident reports from England and Wales. A patient safety incident was defined as “any unintended or unexpected incident that could have harmed or did harm a patient during healthcare delivery.”17 Reporting incidents started on a voluntary basis in 2003, but since 2010, reporting has been mandatory for incidents resulting in severe harm or death. Reports contained structured categorical information about care setting, patient demographics, and the perception of severity of harm, as well as free-text descriptions of the incident, apparent causes, and planned actions to prevent recurrence. The database is described in more detail in a study of patient safety-related hospital deaths in England.13
Study Population
We included reports if they related to the provision of primary health care in England and Wales and were not duplicates. In accordance with the National Academy of Medicine definition of primary care, we also included community health care reports, including those from community-based nursing and mental health care services.18 Our study period, which was April 2005 to September 2013 (42,729 reports submitted during this period), was dictated by data availability at the study outset. We combined all reports of severe harm and death (1,199 reports) with a weighted random sample of incident reports of lower harm severity (12,500) to create a sampling frame of 13,699 reports. The weighting gave greater priority to more recent reports. We described the sampling frame in more detail elsewhere.19
Sample Size
In a pilot study of 857 patient safety incident reports, we found blame descriptions in 47% (401). To estimate the true proportion of blame descriptions within these primary care data, with a 95% confidence interval of no greater than 2%, we calculated that a sample size of at least 2,043 incident reports was required. From the sampling frame of 13,699 reports, we drew a randomly selected sample of 2,679 (to accommodate for the frequency of duplicates and reports with insufficient detail to interpret) using a random number generator.
Study Design
We took a sequential exploratory approach20 based on first a qualitative analysis and then a quantitative analysis. We conducted a content analysis21 of incident reports, coding the incident characteristics and type of blame attributions, after which we conducted a descriptive statistical analysis of the frequency of blame categories.
Data Coding
Using the Recursive Model of Incident Analysis,22 we coded the free-text descriptions of the incidents using the Primary Care Patient Safety (PISA) Classification System,10 which is aligned with the World Health Organization (WHO) International Classification for Patient Safety (ICPS).23 We coded the primary incident type (eg, administration or discharge planning), primary contributory factor (eg, staffing levels or patient vulnerability), and the severity of the outcome (no, low, moderate, or severe harm or death). This method has been described in more detail elsewhere.10 At the analysis stage, we excluded reports that did not describe a patient safety incident (for example, a patient falling in the clinic parking lot). Reports describing pressure ulcers have been excluded in previous work because they typically describe an outcome rather than an incident type. Pressure ulcers, however, accounted for more than 1 in 8 reports in the database, so we included these as an incident type to ensure the sample reflected the way incident reporting is used.10
We coded for blame according to a framework derived empirically by our team of primary care patient safety experts in conjunction with our lay patient and public involvement team. This framework was tested on a pilot sample of reports and amended as necessary. One of the study team (J.C.) coded the categories, and a random sample of 268 (10%) reports was double-coded. We discussed discordance, rectified discrepancies, and calculated a κ coefficient to determine inter-rater reliability of coding.
Statistical Analysis
We calculated odds ratios and 95% confidence intervals of the odds of blame attribution (vs no blame attribution) and performed χ2 tests to assess the associations between attribution of blame and the following prespecified variables: incident type, the number and nature of contributory factors reported, and severity of harm.10 We integrated the quantitative findings with the emerging insights generated from the coding process.
Ethical Approval
The Aneurin Bevan University Health Board (Wales, United Kingdom) research risk review committee was consulted for ethical approval. As all identifiable details were removed before the submission of reports to the National Reporting and Learning System, ethical approval was waived for analysis of this anonymized data set. To further protect confidentiality, we made minor editorial adjustments to any examples provided, for example, removal of dates, location, and in 1 case, a rare diagnosis.
RESULTS
The 2,679 patient safety incident reports were reviewed against the criteria for inclusion. We excluded reports that did not describe a patient safety incident (n = 134) or did not involve primary health care (n = 397), leaving 2,148 incident reports for analysis. Reports came from a range of primary care settings: 1,405 from family practice, 644 from community nursing services, and the remainder from dentistry, mental health, and pharmacy services.
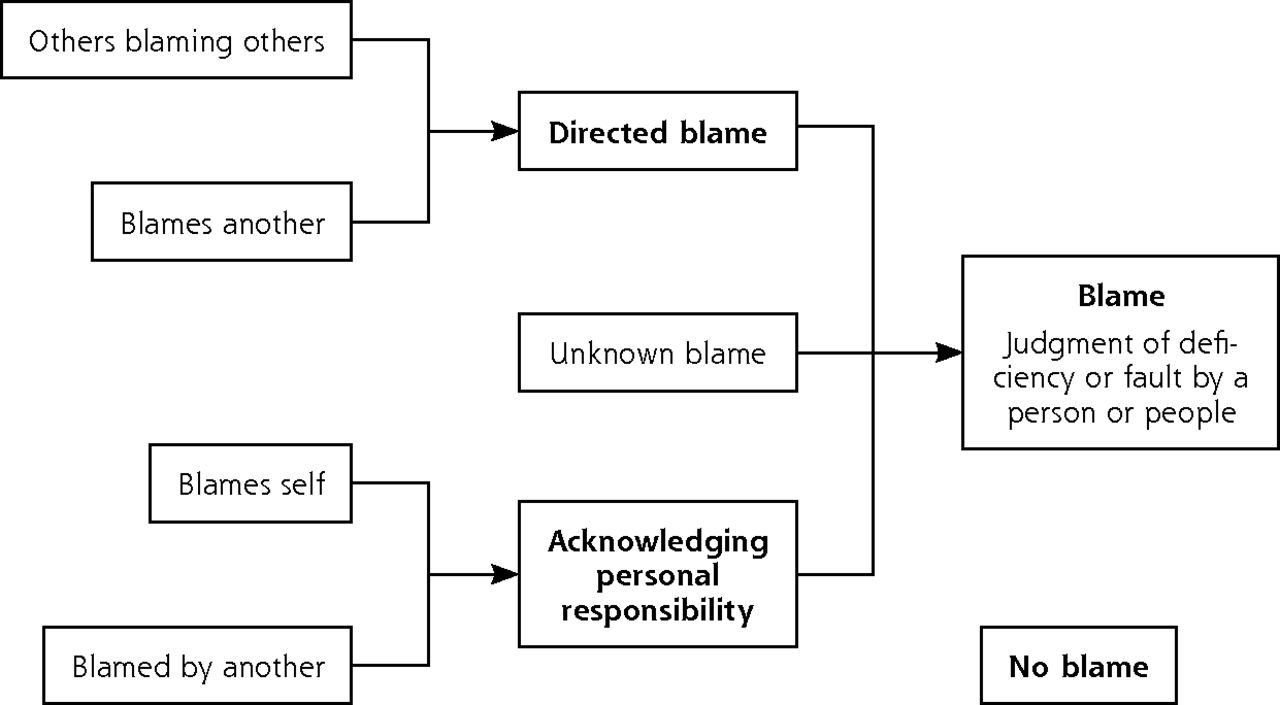
We defined blame as evidence in the free-text of a judgement about a deficiency or fault by a person or people. Described failure of aspects of the system rather than a person was coded as no blame. The remaining incidents described human errors leading to patient safety incidents. We found 5 key categories of blame (Figure 1 and Table 1). Blames self and blamed by another described reports in which the person reporting the incident found fault in his own actions and acknowledged personal responsibility. Blames another and others blaming others, on the other hand, reflect reports that were used to identify others considered worthy of censure: we call this directed blame (Figure 1).
Categories of Blame by Persons Reporting Safety Incidents
Types of blame.
We found an attribution of blame statement in 45% (975) of patient safety incident reports (95% CI, 43%–47%). Cohen’s κ for inter-rater reliability for coding of blame was calculated at κ = 0.81 (95% CI, 0.74–0.88), indicating strong agreement.24 Table 2 shows that where blame was attributed, 92% (894) were cases of directed blame, whereas only 2% (41) acknowledged personal responsibility.
Numbers and Proportions of Blame Attribution (N=2,148 Reports)
We found many cases of directed blame, both from the person reporting the incident and from other reports generated in response to or in anticipation of a complaint (Table 2, example 3: blames another).
Table 3 shows that the 3 types of incidents most likely to be associated with directed blame were those involving discharge planning, communication problems, and referrals. Incident reports involving record keeping and documentation, pressure ulcers, and investigations were significantly less likely to contain directed blame than other incidents.
Likelihood of Directed Blame Attribution With Different Types of Safety Incidents Reported
Where incident reports described 1 or more contributory factors, 50% (433 of 865) attributed directed blame compared with 36% (461 of 1,283) of reports without contributory factors. Table 4 shows the ratios for the odds of blame for each type of primary contributory factor against the odds of blame in the other 3 categories.
Directed Blame and Contributory Factors in Safety Incident Reports
Severity of harm to the patient, ranging from no harm to death, was described in 1,475 incident reports, with 44% (653) of these attributing directed blame (Table 5).
Directed Blame and Severity of Harm in Safety Incident Reports
DISCUSSION
In almost one-half of incident reports, reports containing a judgment featured fault by a person (975 of 2,148), and 42% of reports featured directed blame (894 of 2,148). The proportion showing directed blame varied depending on the incident type, contributory factors involved, and the severity of harm to the patient. Directed blame was less likely in incidents where the patient was harmed (except for the small category of reports about death).
Fear of being held personally accountable is thought to explain much of the reluctance of frontline health care staff to use incident reporting systems to communicate patient safety concerns.2,5,7, 25–27 Although blame is acknowledged to hinder reporting,6 ours is the first study to identify and characterize its use within incident reports themselves.
Health service managers have a responsibility, to motivate reporting within a blame-free culture28,29; further it is difficult to generate learning from reports unless health care is free from an atmosphere of blame.2,12,13 That 42% of reports were used to censure others, however, suggests progress toward a blame-free and supportive culture is slow.
Most safety incidents are caused by a complex interaction of individual actions and system failures, with greater weight given to system factors.9 Reason’s Swiss cheese model describes how, although human error is inevitable, incidents are frequently the result of multiple smaller errors within a failed system: “The important question is not who blundered, but how and why the defenses failed.”9
First, we hypothesize that our results may reflect the outlook and behavior of those working in a culture in which seeking personal accountability for errors is placed ahead of identifying the scope for learning.6,11 Coles et al30 found that hospital clinicians had little confidence managers would deal with reports in a blame-free way. Hospital managers also perceived that incident reports were being used by those making the report to “cover one’s own back” in the event of an incident. Indeed, many directed blame reports were generated in response to or anticipation of a complaint (Table 1, Blames another, example 3).
Second, as Reason explains, humans are susceptible to the fundamental attribution error in that they tend to appreciate systems factors in understanding one’s own actions but tend focus on others’ personal behaviors rather than the wider context influencing them.9 The blames-another example of directed blame (Table 1, Blames another, example 1) lists numerous failures of the physician involved but provides no insights into whether the department was busy or the physician had the appropriate training or supervision.
Those reporting incidents acknowledged personal responsibility for their actions in only 2% of their reports, compared with the 42% of reports directing blame at others. Although the exact proportions may not be generalizable for all incidents or routine practice (because of selection biases in the reporting system), this difference is substantial and suggests key differences and missed learning. We may be missing key insights and soft intelligence that individuals closest to these incidents might have offered.31,32 Soft intelligence is insight from experiences of frontline staff about the reality of the system, which can thrive only where staff feel valued and respected.31,32 Historically, despite its potential, analyses of incident reporting have failed to provide this soft intelligence or support this ethic.
It is unsurprising that persons reporting incidents who identified staff factors contributing to the incident were more likely to apportion directed blame than where equipment or patient factors were considered to be causative. Reports describing organizational contributory factors, however, also had higher odds of containing directed blame. It is possible that those reporting incidents may still make fundamental attribution errors despite recognizing system factors.
Directed blame was more likely in situations of discharge planning, communication, referrals and diagnosis, and assessment. These types of incidents involved clinical judgment and interactions with patients, their relatives, and other health care professionals. Perhaps the more emotive nature and context of these incidents resulted in more frequent directed blame. Furthermore, recognizing a diagnostic error may require judgment by the person reporting the incident, whereas a pressure ulcer or documentation error is a matter of fact and more easily reported as such. Many decisions and judgments in primary care are made by individual clinicians in practices where there are no checks and balances that a larger team provides, as in hospital care. Primary care professionals may therefore be more individually vulnerable to directed blame than their hospital colleagues when an error is made.16
Strengths and Limitations
We used a well-established coding method10 with a high level of coding agreement (κ= 0.81) to ensure methodological rigor. Our study examined associations with blame attribution, and we offer new insights into the way incident reports are used. Generalizations from our study should be made cautiously: selection bias in reporting is important,33 rendering this analysis essentially inductive rather than deductive; the quality of incident report analysis relies heavily on the use of subjective interpretation of events during reporting and the depth of information provided by the those reporting the incidents.34 Also, persons reporting incidents may not necessarily have all the information at the time of writing. Further research should explore how persons reporting incidents are affected by social and cultural influences, as well as by their the motivations and understanding of the potential impact of blame. Such explorations, as well as a comparative analysis of blame in secondary care incident reporting, would enable the effective targeting of interventions to improve the learning from these reports.
Leaders and managers of health care systems and health organizations are frequently urged to develop and promote a climate of learning from things that go wrong. It seems that their current approach, however, may drive their staff to point the finger at their colleagues. This amplification of the process of seeking someone to blame is neither in the interests of patients, nor staff, nor of making health care safer.
Acknowledgments
We gratefully acknowledge Dr Rhiannon Watson for double coding, Sophie Banerjee in double coding the pilot sample, and Dr Huw Prosser Evans for design and development of the analysis software. We also gratefully recognize the contribution of Antony Chuter, chair of the patient and public involvement team, whose contributions were integral to the development of the coding frameworks and definitions of blame.
Footnotes
Conflicts of interest: L.D. was the Chairman of the National Patient Safety Agency (NPSA) (2010–2012) and is currently the World Health Organization’s Patient Safety Envoy. P.H. has undertaken paid consultancy with Power Health Solutions (PHS), St Vincent’s Health Australia and for the Australian Commission on Safety and Quality in Health Care, all regarding incident reporting. A.B. obtained a Cardiff University Research Opportunities (CUROP) scholarship to undertake this work. There are no other conflicts of interest.
Funding support: All coauthors contributed to a project funded by the National Institute for Health Research Health Services and Delivery Research program (project number 12/64/118). https://www.journalslibrary.nihr.ac.uk/.
Disclaimer: The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
- Received for publication December 19, 2016.
- Revision received March 23, 2017.
- Accepted for publication April 30, 2017.
- © 2017 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- What became of the 'eyes and the ears?: exploring the challenges to reporting poor quality of care among trainee medical staff
- Patient and caregiver factors in ambulatory incident reports: a mixed-methods analysis
- Mixed-methods study protocol: do national reporting and learning system medication incidents in palliative care reflect patient and carer concerns about medication management and safety?
- Nature and type of patient-reported safety incidents in primary care: cross-sectional survey of patients from Australia and England
- In This Issue: Tools to Help Focus on What is Valuable