
Abstract
PURPOSE Evidence of the influence of family physicians on health care is required to assist managers and policy makers with human resource planning in Africa. The international argument for family physicians derives mainly from research in high-income countries, so this study aimed to evaluate the influence of family physicians on the South African district health system.
METHODS We conducted a cross-sectional observational study in 7 South African provinces, comparing 15 district hospitals and 15 community health centers (primary care facilities) with family physicians and the same numbers without family physicians. Facilities with and without family physicians were matched on factors such as province, setting, and size.
RESULTS Among district hospitals, those with family physicians generally scored better on indicators of health system performance and clinical processes, and they had significantly fewer modifiable factors associated with pediatric mortality (mean, 2.2 vs 4.7, P =.049). In contrast, among community health centers, those with family physicians generally scored more poorly on indicators of health system performance and clinical processes, with significantly poorer mean scores for continuity of care (2.79 vs 3.03; P =.03) and coordination of care (3.05 vs 3.51; P =.02).
CONCLUSIONS In this study, having family physicians on staff was associated with better indicators of performance and processes in district hospitals but not in community health centers. The latter was surprising and is inconsistent with the global literature, suggesting that further research is needed on the influence of family physicians at the primary care level.
- physicians
- family
- primary care physicians
- primary health care
- cross-sectional studies
- public health systems research
- patient care team
INTRODUCTION
The discipline of family medicine must constantly adapt to be relevant within different health systems and national contexts.1–4 The discourse on the roles and competencies of family physicians attempts to define their contribution to strengthening primary health care systems.5–9 International policy documents on family medicine and primary health care rely on data that are mostly derived from high-income countries; African health care leaders are looking for evidence of benefit from their own low- and middle-income country contexts.10–12
Responding to post-apartheid imperatives to provide universal health coverage, the South African government has embarked on a project of primary health care reengineering as the first step in a progression to national health insurance.13,14 Such reforms are aligned with the country’s commitments to universal human rights norms and improvement of health access and equity.15–17
Although South Africa has had informal vocational training in family medicine for almost 35 years, the discipline was only formally registered in 2007, and new family physicians began graduating from the 4-year full-time residency training program only in 2011.2,18,19 Family physicians are trained to fulfill 6 key roles: a competent clinician, a consultant and a capacity builder to the health care team, a leader of clinical governance, a supporter of community-orientated primary care, and a clinical trainer2 (see Supplemental Appendix 1 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1.) A national position paper argues that family physicians should be expert generalists placed throughout the district health system,2 which includes district hospitals, community health centers, and primary health care clinics within subdistricts. Appointment of family physicians to public-sector posts across the country’s 9 provinces has occurred in a heterogeneous fashion, however. The variation in deployment can partly be explained by a lack of local evidence to support family physicians’ contribution and confusion as to the roles of this new “specialist” in the health system.12,20
The aim of this study was to assess the influence of family physicians at primary care facilities and district hospitals. Their influence was evaluated in terms of 2 domains: health system performance and quality of clinical processes across the burden of disease. This article presents the findings from 1 of 4 studies, both published here and elswhere,21,22 and unpublished (K.B.vP, et al, December 2017) that evaluated the early impact of family physicians on the South African health care system.
METHODS
Study Design
We conducted a cross-sectional, observational study to compare community health centers (primary care facilities) and district hospitals with vs without family physicians. Use of family physicians was not randomized as the creation and filling of family physician posts were predetermined by local policy and service requirements. The group of facilities with family physicians had had a family physician in a designated post for a minimum of 2 years. The comparison group consisted of facilities that did not have a family physician post on staff or any other exposure to a family physician. We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement’s checklist23 to guide this research.
Conceptual Framework
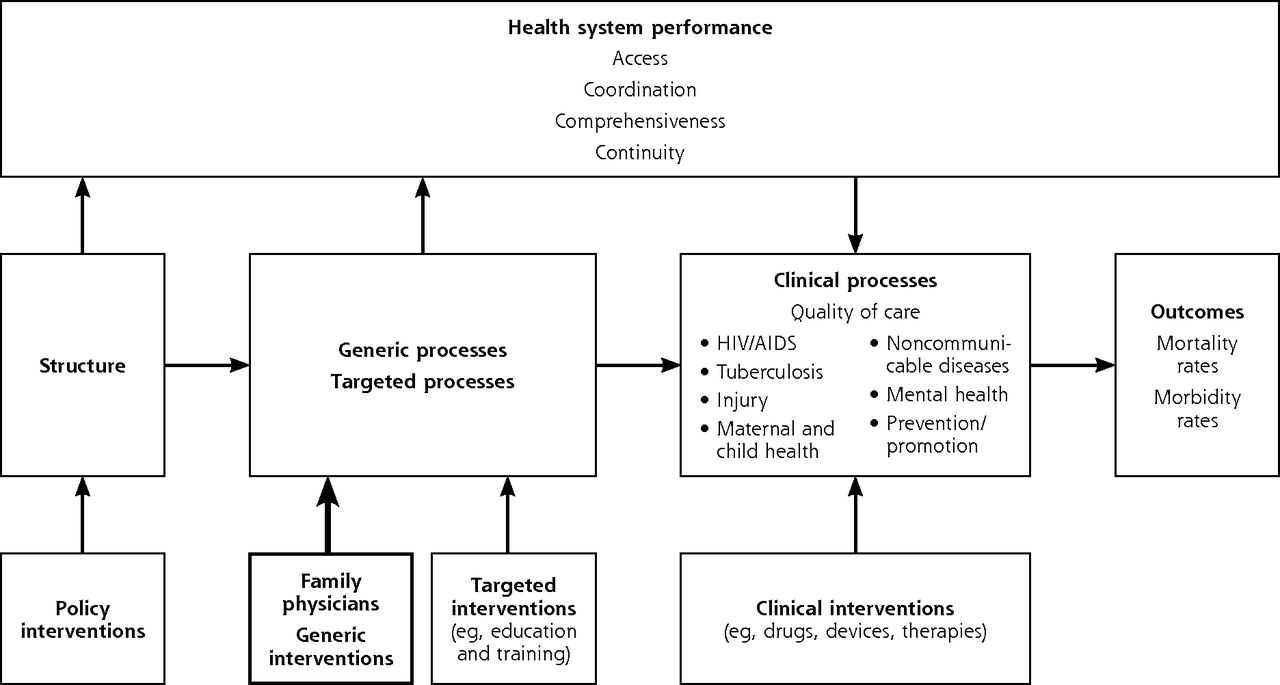
We created a conceptual framework (Figure 1) to inform our approach to designing the study and determining the data collection instruments. In this framework, structure refers to issues of governance and economics that are largely affected by changes in policy. Health service processes are subdivided into generic (cross-cutting organizational processes), targeted (aimed at a specific program or condition), or clinical (services at the level of the patient). Generic and targeted processes can affect health system performance, which also influences the quality of clinical processes that in turn affect clinical outcomes. Family physicians were seen as a generic intervention as they were not limited to a specific program or condition and could have impact broadly on health system performance and clinical processes. We assessed 4 key aspects of primary health system performance: accessibility, coordination, comprehensiveness, and continuity.26 The key clinical processes were drawn from South Africa’s quadruple burden of disease and public health issues: HIV/AIDS and tuberculosis; violence and injury; maternal and child health; and noncommunicable diseases.17

Setting
This study was conducted in the district health system of the South African public sector in 7 of the country’s 9 provinces. (See Supplemental Appendix 2 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1 for a brief description of the South African district health system.)
Sample Size Calculation
We used a clinical process indicator (the diabetes management score) and a health outcome indicator (the facility-based perinatal mortality rate) for calculation of study sample size, given that family physicians are reported to have a positive impact on these indicators, with an earlier study providing standard deviations and estimates of likely effect size.27
A sample size of 14 community health centers in each group gave 80% power to detect an effect size of 10% in the diabetes management score (SD, 13%) with a possible 5% type 1 error.27 A sample size of 14 district hospitals in each arm gave 80% power to detect an effect size of 8.4 perinatal deaths per 1,000 births in perinatal mortality rate (SD, 7.91) with a 5% type 1 error.27
We therefore chose a final sample size of 15 district hospitals and 15 community health centers in each group (with and without family physicians, for 60 facilities in total) to have sufficient power and to allow for some loss of facilities or incomplete data collection.
Facility Selection
Seven out of the 9 provinces were included in the study as determined by the educational footprint of the 6 participating universities that train family physicians in South Africa. We obtained a complete list of district hospitals and community health centers from the National Department of Health. With the assistance of the participating universities, this list was split into lists of facilities with and facilities without family physicians, which were then randomly reordered. Starting at the top of the randomly ordered lists, we selected 2 district hospitals and 2 community health centers with family physicians from each province to give 14 district hospitals and 14 community health centers. Each was then matched with a facility without family physicians from the other list using criteria shown in Table 1. One additional facility for each group was selected from the Western Cape Province, where the study was based, to arrive at the intended number of 15 facilities per group. (Supplemental Appendix 3, at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1, shows the facility sampling selection process.)
Matching Criteria by Facility Type
Indicators and Data Collection Instruments/Tools
For study outcomes, we selected a set of indicators that we expected would reflect the influence of the family physician on clinical processes, health system performance, and clinical outcomes (Figure 1). The selection of corresponding data collection instruments/ tools (Table 2)28–35 was dependent on the availability of reliable and valid routinely collected data or existing tools, the feasibility of collecting data, the different scope of practice in district hospitals and community health centers, and an a priori consensus between the researchers in the participating academic departments.
Instruments/Tools Used for Data Collection
Fieldwork and Data Management
We trained 4 teams with a total of 16 fieldworkers (11 health professionals and 5 assistants with previous experience in research data collection) to collect data in the 7 provinces according to a detailed fieldwork protocol (Supplemental Appendix 4 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1). Fieldworkers were interviewed before appointment. Training was facilitated by the lead investigator (K.B.vP.) over 2 to 3 days, and consisted of face-to-face training, role playing, and practical evaluation in the field. Each team was led by a health professional and supervised by an academic family physician attached to a participating university. The teams also interacted remotely with the lead investigator (K.B.vP.) via telephone, e-mail, and a communication application (WhatsApp). Facility-level data were collected between June 2015 and March 2016, and then captured with EpiData version 3.1 (EpiData Software) via a double-entry method and using checks to minimize data entry errors.36
Data Analysis
We then imported the data from EpiData into Microsoft Excel (Microsoft Inc) and used SPSS version 23 (IBM Corp)37 to conduct the analysis in consultation with a biostatistician. Data analysis commenced with descriptive statistics for the facilities. Subsequently, the independent samples t test for equality of means was used to compare means between the groups with and without family physicians (continuous dependent variables, see Table 2 for detail on the data collected). For those means found to be significantly different, we performed regression analysis using a generalized linear model to control for the effect of confounders. Confounding variables for health system performance were levels of staff (professional nurses, junior and senior physicians) and distance from a referral hospital. Confounding variables for clinical processes were the presence of outreach to the district health system facility (from the general specialties at the referral hospitals) and bed utilization rate (as proxy of district hospital inpatient workload).
Ethical Considerations
This study was approved by the Health Research Ethics Committee (Medical), Stellenbosch University (reference S15/01/003) and by each partner institution. The 7 provincial health authorities and research committees also gave permission to access facilities across the study setting (Supplemental Appendix 5 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1).
RESULTS
The contribution of each province to the final facility sample is shown in Supplemental Appendix 6 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1. The distribution of sites across provinces differed from that intended because some provinces did not use any family physicians at community health centers or used them at all of those at the subdistrict level. One province did not have any district hospitals without family physicians.
On average, 26 out of the 30 community health centers (87.5%) and 24 out of the 30 district hospitals (80.7%) had complete data sets (data set completion per tool is available in Supplemental Appendix 7 at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1).
Table 3 compares the characteristics of the facilities with and without family physicians, showing that they were fairly well matched. Table 4 compares the facilities on indicators of health system performance and clinical processes, and should be interpreted in conjunction with the instrument/tool descriptions in Table 2; results of this comparison are discussed below.
Facility Characteristics
Comparison of Indicators of Health System Performance and Clinical Processes Between Facilities With and Without Family Physicians
District Hospitals
In the district hospitals, the availability of essential services across the clinical domains was higher in the group of facilities with family physicians, with the availability of key pediatric services differing significantly (mean, 85.0% vs 69.2%; P = .02) (Table 4). The score for Domain 2 of the National Core Standards (which measures aspects of patient safety, clinical governance, and clinical care) was higher for the group with family physicians, but not significantly so; however, only 19 out of 30 district hospital facilities had completed this tool. The child health findings (specifically, the number of modifiable factors identified per audited in-hospital child death) from the child death audit tool (Child Problem Identification Program) was significantly more favorable in this group (mean, 2.2 vs 4.7, P =.049). Findings from the Perinatal Problem Identification Program (which focuses on perinatal, stillbirth, and neonatal mortality rates) favored the facilities with family physicians too, albeit not significantly.
After we adjusted for the influence of confounders on the key pediatric services, presence of senior physicians had a significant influence (β coefficient = 1.317; P = .01), but presence of family physicians was no longer significant (β coefficient = −0.782; P = .88). The significant favorable influence of the family physician on the number of modifiable factors per child death persisted, however (β coefficient=−5.732; P <.001).
Community Health Centers
In the community health centers, however, the findings from the primary care assessment tool (as perceived by users of primary care, Table 4) favored the group of facilities without family physicians, reaching statistical significance in 2 domains: continuity of care (2.79 vs 3.03; P = .03) and coordination of care (3.05 vs 3.51; P = .02). The generalized linear model for the continuity domain was a poor fit and therefore not suited for testing for confounders. The generalized linear model for the coordination domain still favored the facilities without family physicians on staff after adjusting for the confounders (β coefficient for presence of family physician=−0.476; P =.02; intercept β coefficient=3.552). These findings for continuity of care were also affirmed by the managers of primary care (mean difference, 0.25; 95% CI of 0.03–0.50; P = .027). The other domains as measured by the provider and manager components of the primary care assessment tool did not differ significantly between groups. Similarly, there were no significant differences in indicators measured by the chronic disease management audit tool.
DISCUSSION
In this study of South African facilities, data from district hospitals showed that facilities with family physicians generally had higher scores for measures of health system performance and clinical care, and significantly fewer modifiable factors associated with in-hospital pediatric mortality. Senior physicians also contributed to increased access to pediatric life-saving procedures and equipment. A number of initiatives over the last decade have targeted obstetric and neonatal care in district hospitals.28,32,38,39 These findings echo the previously reported child and neonatal health benefits associated with an increased supply of primary care physicians.40
On the other hand, data from community health centers, which deliver primary care, showed that facilities with family physicians generally had lower scores for measures of health system performance and clinical care, as well as significantly lower scores for measures of continuity and coordination of care. These unexpected findings appear inconsistent with the international literature that reports the family physician as being ideally placed to improve primary health care generally and to enhance continuity and coordination of care specifically.9,41–44 It is possible that family physicians were deployed where the need was greatest, as suggested by data showing that facilities with family physicians have a higher average workload (Table 3), and are predisposed to perform more poorly. In addition the family physician’s influence is primarily through the health care team,45 and their influence on the district hospital team (primarily led by doctors) may have been greater than that on the primary health care team (primarily led by nurses), bearing in mind the recognized professional boundaries and hierarchies.46 The family physician is also not formally positioned within the organization’s management structure, and he/she will need to exert a systemic influence through other managers. It is again possible that their influence was greater within the district hospital management structure than in primary health care.47 Another possibility is that the training of family physicians prepared them better for the district hospital as opposed to the primary health care context, as many training programs are still dominated by hospital-based exposure.48,49 In South Africa, the need for and deployment of family physicians in district hospitals has been more clearly conceptualized and operationalized than their role and placement in the primary health care team.2,14,49,50
This study had several limitations. Having family physicians on staff was not randomized, and there may therefore be additional confounders not accounted for or measured. The variability in how family physicians were deployed within the different provinces made it difficult to fully match the facilities between groups. The minimum duration of 2 years of family physicians on staff might have been too short to allow for some aspects of their impact to be measurable. There was no baseline measurement of the outcome indicators at these facilities, before their deployment, which would have enabled correction for significant differences and measurement of change over time. Finally, we did not factor into analysis the type of training the family physician received or the length of time practicing in the field.
Our findings support the need for further research to understand the effects of family physicians on primary health care. District manager interviews and coworker assessments of family physicians (using the 360-degree evaluation tool) in primary health care settings suggest that they are having a beneficial impact, however (unpublished K.B.vP, et al, December 2017,21,51). Our findings may reflect a need to strengthen the family physician’s role in primary health care and to integrate them more fully into the team, as well as to ensure that training programs focus sufficiently on the primary health care setting.
Application of the family medicine and primary health care models from higher-income countries to low- or middle-income health systems (such as those in Sub-Saharan Africa) was reviewed previously in terms of exportability and relevance.45,52–54 A Delphi study among African family medicine leaders demonstrated consensus and commitment toward realizing the principles of primary health care and core values of family medicine, such as person-centeredness, continuity, and coordination of care.55 The application of these principles may differ, however, in African health systems where family physicians do not usually provide first-contact care and must acquire contextually defined competencies, such as the extended range of procedural skills required for working at the district hospital.2,45 African countries that are committed to achieving the Sustainable Development Goals should invest more in training family physicians to scale as well as contextualizing their roles within their primary health care teams, in keeping with the team-based models used in other low- and middle-income countries such as Brazil and Cuba, and supported by the World Health Organization (WHO).12,56–58
This study additionally contributes to the task of refining the methods, indicators, and tools used to measure the influence of South African family physicians. More research will similarly help to understand the facilitators and constraints within the local context that may influence the ability of family physicians to exercise their full potential.9 Such research will guide the ongoing efforts to implement the principles of family medicine within the district health system.18,49,53,59
Acknowledgments
The authors wish to thank the managers, staff, and patients for welcoming the fieldwork teams into their facilities. The authors would also like to acknowledge the following persons regarding the use of the data collecting instruments: Ms U. van Vuuren from the Western Cape Government Department of Health for the use of the chronic disease management audit tool; Dr C. Marshall from the National Department of Health for the use of the National Core Standards tool; Prof R. Pattinson from the Medical Research Council of South Africa for his guidance around using the signal functions tool; Dr G. Bresick from the Department of Family Medicine, University of Cape Town (South Africa) for the guidance and training around using the PCAT; Dr L. Campbell from the University of Kwa-Zulu Natal (South Africa) for coordinating the data collection in the Kwa-Zulu Natal province; and Dr M. Patrick for his help in facilitating access to the Child PIP data. The authors also wish to thank the 16 members of the research teams for their help in collecting and capturing the data: Sr D. Cairncross, Mr L. Chinhoyi, Mr A. Geiger, Sr J. Mokaya, and Mr D. September (Stellenbosch University); Mr D. Greeves and Mr B. Mashaba (Sefako Makgatho Health Sciences University); Ms Z. Gumede and Sr S. Mkhize (University of KwaZulu-Natal); Sr G. Mathebula and Dr P. van Niekerk (University of Pretoria); Mr J. Botes, Mr T. Mokhobo, and Sr M. Els (University of the Free State); and, Ms T. Rwafa and Dr O. Femi (University of the Witwatersrand). In addition, the authors would also like to thank Ms S. Munshi (University of the Witwatersrand) for her help during the initial planning phase of the study.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was conducted with the financial assistance of the European Union. Additional funding was received from the Discovery Foundation (South Africa) and the Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa.
Disclaimer: The contents of this article are the sole responsibility of the authors and can under no circumstances be regarded as reflecting the position of the European Union.
Prior presentations: National conference of the South African Academy of Family Physicians in Cape Town, South Africa, August 12–14, 2016; Annual Research Day of the Faculty of Medicine and Health Sciences, Stellenbosch University in Cape Town, South Africa, on August 11, 2016.
Supplemental materials: Available at http://www.AnnFamMed.org/content/16/1/28/suppl/DC1/.
- Received for publication January 25, 2017.
- Revision received June 3, 2017.
- Accepted for publication June 22, 2017.
- © 2018 Annals of Family Medicine, Inc.




{kind=link}