
Abstract
PURPOSE Prostate cancer screening guidelines have changed as new evidence showing an equivocal mortality benefit led many organizations to relax recommendations for this screening and instead suggest shared decision making. Presently, it is unknown how successfully these conversations happen. Our objective was to understand men’s communication preferences when they discuss prostate cancer screening.
METHODS In this scoping review, we searched 4 electronic databases (Medline, Embase, PsycINFO, and CINAHL) and the gray literature. Additional studies were obtained from reference lists of included studies and relevant review articles. We included qualitative studies reporting patient perspectives relevant to the research question and published in English. Two independent researchers screened titles and abstracts based on these criteria, conducted a full-text review for final inclusion, evaluated the remaining articles for validity, extracted data, and used thematic analysis to build a thematic framework. A subgroup analysis was performed for Black men as many studies elicited their perspectives.
RESULTS Analyses were based on 29 studies. We identified 4 main themes that men described as critical for successful prostate cancer screening risk discussions with their primary care clinician: using everyday language, receiving a sufficient quantity of information, spending enough time, and having a trusting and respectful relationship. Three additional themes emerged that prohibited men from having any discussions at all: having already decided to pursue prostate cancer screening, being passive in medical encounters, and perceiving threat to one’s well-being. Black men faced racism, which impacted medical interactions.
CONCLUSIONS Our findings point to strategies to support men’s communication preferences and address preconceptions surrounding prostate cancer screening. More studies are needed in certain underrepresented populations given the propensity for disparity in health outcomes.
- prostate cancer
- cancer screening
- communication
- shared decision-making
- risk assessment
- patient-centered care
- patient participation
- physician-patient relations
- primary care
- preventive health services
- professional practice
INTRODUCTION
The Canadian Cancer Society reports that prostate cancer is the number 1 diagnosed malignancy and the third-leading cause of cancer-related death in men.1 Despite these high rankings, the 5-year survival rate is 91% and the overall mortality attributed to prostate cancer has decreased by 50% since 1995.1 The diagnosis is typically made in asymptomatic men after they screen positive for an elevated prostate-specific antigen (PSA) level and undergo a prostate biopsy, which engenders its own risks, namely, serious bleeding and infection.2 The long-term mortality benefit of population-wide prostate cancer screening using PSA has come into question, with 2 large randomized controlled trials showing conflicting results.3,4 Implementing a population-level screening strategy that minimizes unnecessary biopsies but still detects potentially aggressive disease remains challenging. Recognizing this uncertainty, many professional organizations now recommend shared decision making when considering screening with a PSA test starting between ages 45 and 50 years and stopping at age 70 years, with varying screening intervals based on the patient’s baseline risk.5-8
Men eligible for prostate cancer screening face enormous pressure as they rapidly digest complex information to make a decision that can markedly impact their health. Coupled with time constraints during clinical encounters, misunderstanding of the multifaceted concept of risk limits men’s ability to effectively participate in shared decision making. Screening rates have been shown to fall because of persistent confusion over the risks and benefits.9 The decline in screening may be implicated in the rising incidence of advanced prostate cancer.10 Furthermore, Black men in particular face systemic inequity in the form of underrepresentation in primary care roles, lower health literacy, lack of insurance, financial and geographic inaccessibility, and lack of representation in clinical trials, resulting in barriers to accessing the health care system.11 This obviously undermines shared decision making in a group known to experience health disparities in prostate cancer along the spectrum of screening, diagnosis, treatment, and survival.11-13 As shared decision making becomes prevalent in primary care, understanding how men prefer having risk discussions can facilitate these discussions when considering prostate cancer screening.
A metanarrative systematic review studying information-seeking behaviors among men considering cancer screening showed that many were “passive gatherers,” meaning knowledge related to cancer screening usually came from unsolicited sources rather than independent effort.14 Understanding men’s communication preferences can help engage them in becoming active participants in their own health care. Decision aids, such as pictographs representing risk or videos of patient experiences, are available to support patient choice and have been shown to improve patient-clinician communication, health knowledge, and patient engagement.14 Decision aids had a mixed impact on the actual decision to screen, however, and it is unknown to what extent patients themselves were involved in creating these materials.
For these reasons, it is paramount that we better understand men’s communication preferences to optimize shared decision making in primary care, especially given the equivocal evidence of the mortality benefit of population-wide prostate cancer screening and difficulties appreciating the nuances of risk when applied to the individual. The objective of our study was to understand how men prefer discussing the risks and benefits of prostate cancer screening with their primary care clinician.
METHODS
Protocol
We conducted a scoping review to systematically explore men’s communication preferences for shared decision making when considering prostate cancer screening. We developed our protocol following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews Checklist15 and registered the protocol with the Open Science Framework online (https://osf.io/ebwnz/).
Search Strategy
We developed our search strategy in collaboration with a medical science librarian. We searched 4 databases (Medline, Embase, PsycINFO, and CINAHL) from their date of inception to March 2022. The key words and MeSH headings used, and our search strategies, are outlined in the Supplemental Appendix. Additional articles were systematically retrieved from the gray literature by following an extensive checklist prepared by Canada’s Drug and Health Technology Agency (Supplemental Table 1).16 To ensure the completeness of our search, we searched for references from studies that met the inclusion criteria and included relevant citations in the article-screening process.
Eligibility Criteria
Taking a patient-centered approach, we developed inclusion criteria requiring that articles detailed patient preferences for risk communication surrounding prostate cancer screening in English-speaking primary care settings. Specifically, we included peer-reviewed qualitative articles on eligible men who had never received a prostate cancer diagnosis and their perspectives on how prostate cancer screening was discussed with them by their primary care clinician. Articles written in a language other than English were excluded to eliminate heterogeneity owing to nuances in communication between languages. We also excluded articles that evaluated primary care clinicians’ perspectives or were quantitative in nature.
Study Selection
We selected studies using Covidence (Veritas Health Innovation Ltd), a web-based and collaborative software that streamlines literature reviews. Duplicates were removed by Covidence and manual revision. Two independent reviewers (J.F. and D.D.) screened titles and abstracts according to the inclusion and exclusion criteria described previously. We pilot tested the screening process by screening the first 50 electronic database search results. All the included articles from the screened titles and abstracts underwent full-text review for final inclusion. We resolved conflicts through direct discussion between the 2 reviewers, and any remaining unresolved conflicts were mediated by a third party with content expertise (M.V.). Our interrater reliability, measured by the Cohen  , for abstract screening and full-text review was 0.75343 and 0.59972, respectively. We appraised the validity of the included articles with the Critical Appraisals Skills Programme (CASP) Qualitative Studies checklist,17 a 10-item user-friendly and pragmatic questionnaire designed for use in qualitative health research.18 Question 10 in the CASP checklist (“How valuable is the research?”) evaluates the overall contribution of the study to the broader literature. Given that question 10 would not contribute to the quality of the participants’ responses, we chose not to display the results for this question.
, for abstract screening and full-text review was 0.75343 and 0.59972, respectively. We appraised the validity of the included articles with the Critical Appraisals Skills Programme (CASP) Qualitative Studies checklist,17 a 10-item user-friendly and pragmatic questionnaire designed for use in qualitative health research.18 Question 10 in the CASP checklist (“How valuable is the research?”) evaluates the overall contribution of the study to the broader literature. Given that question 10 would not contribute to the quality of the participants’ responses, we chose not to display the results for this question.
Data Extraction and Synthesis
We created a custom data collection form in Covidence using an iterative process with the study team. We pilot tested this abstraction form with 5 articles to ensure the relevancy and consistency of the information captured. We then collected study characteristics (authors, country, source of information, number and demographics of participants, and verbatim text in the Results or Findings section).
Analysis was conducted using thematic synthesis, a technique developed by Thomas and Harden19 that applies the rigorous methodology of a systematic review to combine the results of qualitative studies. We chose this technique as a practical way to summarize viewpoints taken across the various contexts of the included studies. Following their approach,19 we read line by line all text collected verbatim under the Results or Findings sections of our included articles.
We used NVivo software (QSR International) to apply codes to relevant verbatim text, which consisted mainly of quotes from men themselves. Common codes were grouped to develop descriptive themes, which were then adapted in relation to the research question and synthesized into an analytic thematic framework (Supplemental Table 2 and Supplemental Table 3). Owing to the large number of studies of Black men meeting inclusion criteria, a post hoc subgroup analysis was performed for this group.
RESULTS
We retrieved 726 articles for title and abstract screening. After the screening process, 29 studies eventually met all inclusion criteria (Figure 1). The characteristics of the included studies are summarized in Supplemental Table 4. Most studies were conducted in the United States (23 studies) and elicited perspectives from Black men (25 studies). Participants’ education levels ranged widely, from primary school to college or university degrees, in the 19 studies reporting this demographic. Ten studies reported socioeconomic status. Only 4 studies had good validity based on the CASP questionnaire (Table 1).20-48 The rationale for the research design was unclear in roughly one-half the studies (12 studies). As well, a sizable share (19 studies) did not comment on how the relationship between interviewer and participants could impact reported results.

PRISMA flow diagram of search results, screening, and full text review.
PRISMA = Preferred Reporting Items for Systematic Review and Meta-Analysis.15
Assessment of the Validity of Included Studies (N = 29)
Main Themes
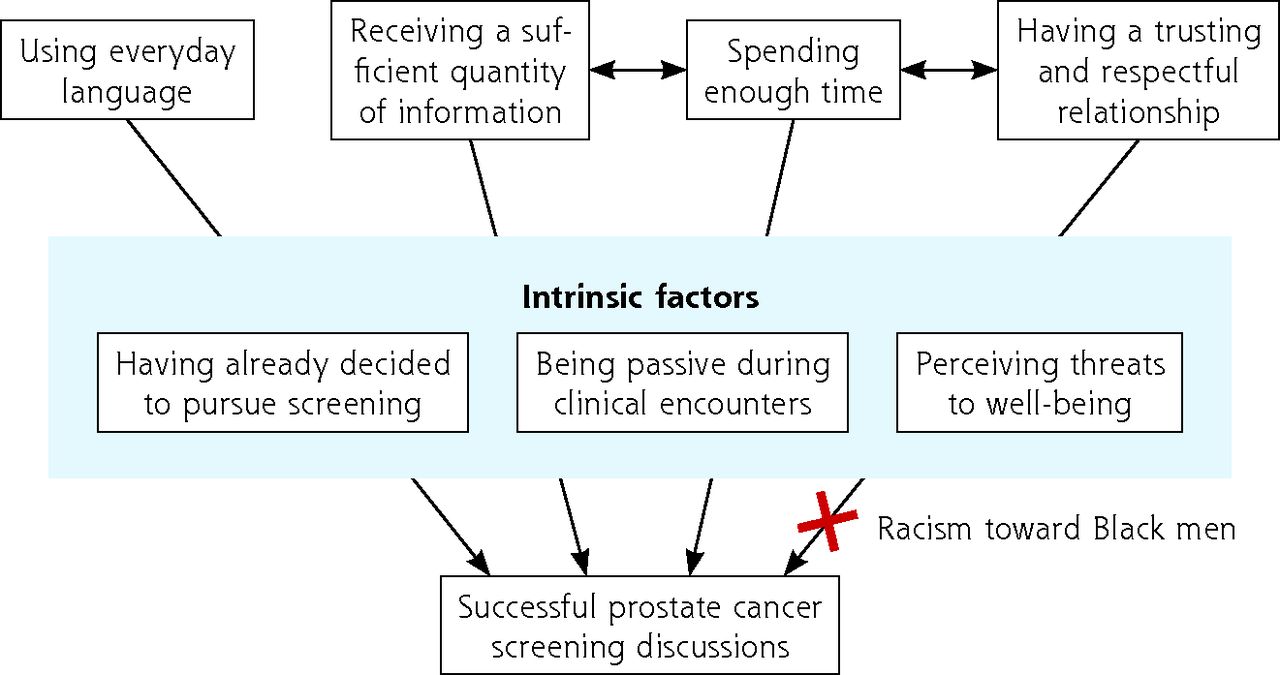
We identified 4 main themes described as critical by men for successful prostate cancer screening risk discussions with their primary care clinician: using everyday language, receiving a sufficient quantity of information, spending enough time, and having a respectful and trusting relationship.
Everyday Language
Using everyday language helped men understand their primary care clinician so that effective communication surrounding screening could happen.22,24,27 Men frequently found clinicians’ inadvertent use of medical jargon a barrier to shared decision making.27,37,48 When clinicians neglected to consider men’s educational background during a prostate cancer screening discussion, it not only caused confusion but also made them fearful.27
Sufficient Quantity of Information
The quantity of information was a prominent theme among men who felt risk discussions were most successful when they received balanced and thorough information regarding prostate cancer screening.22,44 Actively disclosing information this way allowed men to consider screening factors they had not considered themselves.27,44 For example, men rarely considered possible downstream consequences if they screened positive.44 Having this information empowered them to fully engage in shared decision making with their primary care clinician.24,26 By contrast, some men were not given information about the risks and benefits of screening, the meaning of test results, or the clinical trial evidence on screening, or an opportunity to discuss personal values before having the PSA test. Instead, they underwent screening solely on the advice of their clinician.26 Even when screening results were negative, men described ongoing health anxiety if not given an adequate explanation of its meaning.21,22,27 The brevity of the clinical interaction was blamed as a major contributor to the lack of information transfer.22,27,41,47 Furthermore, the option of prostate cancer screening was not even discussed with some men, precluding the entire shared decision making process.28,31,38
Enough Time
Men appreciated primary care clinicians spending enough time with them to have all information explained and felt they had a complete understanding as a result.20,22,44 They articulated gender differences in the amount of time spent per visit, noting that female clinicians tended to have longer discussions.27 Having longer discussions was more reassuring to men who were making the decision to participate in prostate cancer screening and had the dual benefit of fostering a therapeutic relationship.22,48
Respectful, Trusting Relationship
Having a respectful and trusting relationship with their primary care clinician positively impacted men’s ability to participate in shared decision making. Men who had trusting relationships with their clinicians said this empowered them to engage in prostate cancer screening discussions.22,36 Patient and clinician demographics played a key role in the therapeutic relationship. For example, gender was again brought up as an important factor. Men were more comfortable discussing matters related to the prostate with male primary care clinicians based on anatomic similarity.25,27,36 Additionally, men viewed younger clinicians critically because of their lack of experience.26
Emergent Themes
During thematic synthesis, 3 emergent themes arose describing intrinsic factors that blocked men from engaging in shared decision making. Though not directly related to communication, they nonetheless had an impact on discussions about prostate cancer screening. These emergent themes were having already decided to pursue screening, being passive during clinical encounters, and perceiving threats to well-being.
Predetermined Decision to Screen
Having already decided to pursue screening before the clinical encounter was commonly reported across studies, and men had many reasons for this resolution. Some believed that screening was the “right thing to do” and viewed preventive health in general with high regard, without acknowledging the risks it would entail.24,29,35,38,41 The perception that preventive health would increase longevity and, thus, capacity to provide for family motivated other men to request prostate cancer screening.21,42,45 Still others were influenced by availability bias, citing prostate diagnoses in those immediately around them as having solidified their decision to undergo screening.24,35,41,44 Finally, there were men who wanted to know what their PSA level was for the sake of knowledge.26,29
Passivity During Clinical Encounters
Being passive during clinical encounters meant the men did not actually make shared decisions when choosing prostate cancer screening. Although a trusting patient-clinician relationship was cited as important to men, some extended this to the point of complete obedience and did not feel the need to discuss recommendations made by their primary care clinician.25,28,30,45-47 Men also described apathy toward shared decision making for prostate cancer screening.26,28,44 Other reasons for passivity during visits were perceived intellectual disparity41 and a power differential.20
Perceived Threats to Well-Being
Perceived threats to well-being were broadly discussed in 2 variations: threats to masculinity and threats to longevity. Aversion to discussing prostate cancer screening was sometimes grounded in the potential negative impact on sexual function.26,29,35,42 As well, discussing health concerns was not considered congruent with masculine identity and so was avoided.31,33,42 Having a good state of health made some men question the worth of an early diagnosis.38 Fear of potentially having prostate cancer and the alleged belief of definite mortality prevented other men from wanting to discuss screening.29,33,34,39,40
Influence of Race
Discussing prostate cancer screening with Black men comes with additional complexity. Many Black men articulated a cultural norm of visiting their primary care clinician only when they felt extremely unwell.23,31,34,39,42,45 They experienced racism during clinical interactions, manifesting mostly as assumptions about their intelligence.29,45,48 Some expressed a desire to interact with Black primary care clinicians so that culturally appropriate care could be provided.20,42 As well, intergenerational trauma from systemic racism in the medical system had an ongoing impact during clinical encounters.40,43,45 Specifically, Black men expected to be mistreated by the medical staff20,43,45,48 and related warily to primary care clinicians who were perceived to be authority figures.20,23,45
Thematic Framework
The overall thematic framework of men’s communication preferences for shared decision making during discussions about prostate cancer screening is illustrated in Figure 2. In Supplemental Table 5, we provide select quotes from included studies about men’s communication preferences when discussing prostate cancer screening, highlighting examples of strengths and areas requiring improvement as it pertains to communication with primary care clinicians.

Thematic framework of men’s communication preferences for shared decision making during prostate cancer screening discussions.
DISCUSSION
As shared decision making in prostate cancer screening becomes more prevalent, understanding what makes this process successful invites opportunities for optimization. Our scoping review identified 29 articles documenting men’s communication preferences when discussing the risks and benefits of prostate cancer screening with their primary care clinicians. We found that men wanted their clinicians to use plain language so they can better appreciate nuances when choosing to pursue screening. They also preferred clinicians who proactively offered balanced and thorough explanations of what evidence exists for risks and benefits, and the downstream implications of resulting PSA levels. Spending enough time to have these complex discussions was considered essential for men. Finally, men voiced their desire to have these conversations with trusted primary care clinicians in a respectful environment.
Several intrinsic factors emerged during our review that hindered men from having open conversations. Before visiting their primary care clinician, some men had already decided they wanted prostate cancer screening and would not allow space for other considerations. Others consistently took a passive approach during clinical interactions and followed recommendations without having any further discussion. Lastly, perceived threats to their well-being deterred some men from wanting to have conversations at all.
Strategies to Improve Shared Decision Making
Much of what men prefer regarding prostate cancer screening discussions is best provided in primary care, where patient-physician relationships are more likely to be established and where preventive health care is practiced routinely. On the foundation of a deep relationship, which has numerous advantages,49 primary care clinicians are poised to disseminate comprehensive information with the aid of decision-making tools. One evidence-based and practical tool, developed by Vickers et al,50 gives practical patient-centered discussion points during prostate cancer screening discussions. Other decision tools of varying complexity and format exist and were shown to increase patient knowledge and decrease decisional conflict in a meta-analysis by Ivlev et al.51 Educating men is beneficial in that it directly addresses concerns they raise about the natural history of prostate cancer and the complications of screening. In the same meta-analysis,51 visual aids specifically were most effective for reducing fervor in men who viewed prostate cancer screening positively, which by extension could be helpful in those who have already decided to undergo screening as seen in our review, although the quality of the evidence was low and overall intention to screen at 1 year was not affected. Using absolute risk reduction with an added bar graph or icon array is preferable as patients more accurately appreciate risk differences when presented this way.52
Patient passivity has been shown to be modifiable through a feasible office intervention.53 During this “activation” process, patients were guided to generate a prioritized list of questions to ask their primary care clinicians in advance of their visit that would inform decision making.53 When “activated” patients had prostate cancer screening discussions, it positively influenced primary care clinicians, who were then more likely to engage in shared decision making with other patients and make neutral recommendations.54
Time limitations were described as a major issue in our review. In addition to directing patients toward decision-making tools for review on their own, primary care clinicians could consider having discussions over multiple appointments or booking dedicated visits for discussions. Alternately, conversations could be spread among members of an interprofessional team, which could include family members and a decisional coach.55 A randomized controlled trial is already under way to investigate the effect of decision coaches on decision quality and patient perception of care quality.56
Our findings show the critical impact of using everyday language and having a therapeutic patient-physician relationship on shared decision making in the realm of prostate cancer screening, and this impact is aligned with the literature. An updated systematic review by Edwards et al57 demonstrates this effect by showing that tailored health messages increased measures of shared decision making for breast and colon cancer screening. In another narrative review of risk communication in general, the importance of using plain language and tailoring communication is again emphasized.58 Themes of predetermined decisions to screen and threats to well-being discovered in our study agree with results in another qualitative review of men’s perspectives on prostate cancer screening by James et al.59
Further, previous literature shows how medical communication is affected by gender and race. In terms of gender differences, female primary care clinicians were found to spend more time with patients and were more likely to engage their patients in shared decision making.60 Patients racially discordant with their primary care clinicians felt less participatory, and this was especially true for Black men.61
Many studies in our review assessed Black men’s perspectives. We found that cultural differences exist in how these men use health care services and that experiences of racism have eroded trust in the health care system, leaving a lasting impact on how this group interacts with their primary care clinicians. These factors should be considered when attempting shared decision making for prostate cancer screening. Although prostate cancer mortality has decreased overall, a wide gap remains between Black men and their non-Black peers.12 Various solutions have been proposed at different levels of the medical system, and it remains to be seen if this gap closes.11,13 Our study suggests actions primary care clinicians can take at an individual level, namely, being sensitive to cultural differences during interactions to facilitate communication and acknowledging the role of ongoing systemic racism to build trust.
Limitations
Limitations of our review include underrepresentation of Latine men and Asian or Pacific Islander men, 2 groups who may have been excluded because of language criteria but who make up an appreciable percentage of the population in the countries studied. Caution is advised when applying the themes revealed in this review to prostate cancer screening conversations with these ethnicities. Decontextualization and reinterpretation of our collected data are a subject of concern for qualitative synthesis methodology as a whole, as the true meaning behind provided quotes may be lost.62 We hope, however, that these generalizations serve busy clinicians well at their next clinical encounter and spark new areas of research in this domain.
Implications for Research
Future research could study the communication preferences of underrepresented ethnicities, which would allow for more tailored discussions for these groups. Another diverse group in which there is a paucity of research is the lesbian, gay, bisexual, transgender, and queer/questioning (LGBTQ) community. Screening rates and perceptions of informed decision making among gay and bisexual men are higher than those among their heterosexual peers,63,64 although it is unknown how they prefer having these conversations, especially in the context of ongoing inequity.65 Transgender populations present unique challenges when discussing prostate cancer screening, as such conversations can be distressing because of the gendered implication of having a prostate gland. Indeed, their prostate cancer screening rates are lower than those of cisgender men.63 Measures to evaluate the effectiveness of risk communication exist, but they were primarily developed in White populations.66 Results from this review may inform the development of a success measure that scores prostate cancer screening discussions for underrepresented groups, such as Black and transgender populations, given their disparities in prostate cancer care.
Conclusions
Our review reveals men’s communication preferences during prostate cancer screening conversations with their primary care clinician. Men want their clinician to use everyday language, to give thorough and balanced information, to spend enough time during these discussions, and to have a therapeutic relationship. Three emergent themes arose that precluded men from engaging in conversations: having already decided to get screened, being passive during visits, and feeling that their well-being was threatened. Many studies elicited Black men’s perspectives; a subgroup analysis revealed themes of racism and cultural differences.
Primary care remains the ideal place to have prostate cancer screening discussions, although attention must be paid to holding evidence-based conversations and removing barriers to the needed changes. Using decision aids, “activating” patients, and involving decision coaches are feasible approaches to incorporating men’s communication preferences in a busy primary care office. Future directions include conducting more qualitative studies on underrepresented groups and creating a culturally sensitive outcome measure to evaluate the success of prostate cancer screening discussions in Black men.
Acknowledgments
The authors would like to acknowledge Karine Fournier, a health sciences librarian at the University of Ottawa, for her help in developing the initial search strategy and suggesting software used in this review.
Footnotes
Conflicts of interest: authors report none.
- Received for publication January 16, 2023.
- Revision received May 11, 2023.
- Accepted for publication May 31, 2023.
- © 2023 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.