
Abstract
PURPOSE We wanted to explore how patients’ experiences with preventable problems in primary care have changed their behavioral interactions with the health care system.
METHODS We conducted semistructured interviews with 24 primary care patients, asking them to describe their experiences with self-perceived preventable problems. We analyzed these interviews using the editing method and classified emotional and behavioral responses to experiencing preventable problems.
RESULTS Anger was the most common emotional response, followed by mistrust and resignation. We classified participants’ behavioral responses into 4 categories: avoidance (eg, stop going to the doctor), accommodation (eg, learn to deal with delays), anticipation (eg, attend to details, attend to own emotions, acquire knowledge, actively communicate), and advocacy (eg, get a second opinion).
CONCLUSIONS Understanding how patients react to their experiences with preventable problems can assist health care at both the physician-patient and system levels. We propose an association of mistrust with the behaviors of avoidance and advocacy, and suggest that further research explore the potential impact these patient behaviors have on the provision of health care.
INTRODUCTION
Most medical error research focuses on errors in hospital care,1 although most health care is delivered in the outpatient, primary care setting.2 Exactly what encompasses medical error and patient safety in the outpatient setting has been a matter of some debate.3–5 Dovey and Phillips support a definition that includes “policy, regulation, payment and management as well as medical care delivery.”4 The Institute of Medicine, in their report Patient Safety: Achieving a New Standard of Care, “strongly believes that patient safety is indistinguishable from the delivery of quality care.”6 Studies asking both patients and physicians to report or describe errors have produced responses as diverse as incorrect prescriptions, lost laboratory results, disrespectful physicians, and inability to get timely appointments.7,8
Even using a broad definition of patient safety that encompasses quality and related issues, there is still much we do not know about safety from the patient’s point of view.8–11 Patients do report they experience error in ambulatory care,12,13 and many patients and physicians express the belief that patients have some responsibility for their safety.10 Several agencies and foundations recommend active patient involvement.14–17 Although no research indicates that following these recommendations will change patient outcomes, analogous studies of patient empowerment in disease management show that similar actions taken by patients do affect their outcomes.18–21
Anecdotal reports describe how patients who experience error change their behaviors in interacting with health care clinicians.9,22 Research supporting these reports or documenting the extent and type of these changes, however, has not been done. The purpose of this study was to assess how patients’ experiences with self-perceived preventable problems, including medical error and quality lapses, affected them emotionally and altered their interactions with health care.
METHODS
This qualitative study was conducted between November 2002 and October 2003. Because of the exploratory nature of this research, we chose to use a solicitation question that was broad and put the onus of perception on the patient. Our question was similar to questions that have been used in other studies to identify patients who experienced medical error8 and is consistent with a broad definition of patient safety.6
The study was set in 2 large university-affiliated, community-based family practices in the Cincinnati, Ohio, area.
Participant Selection
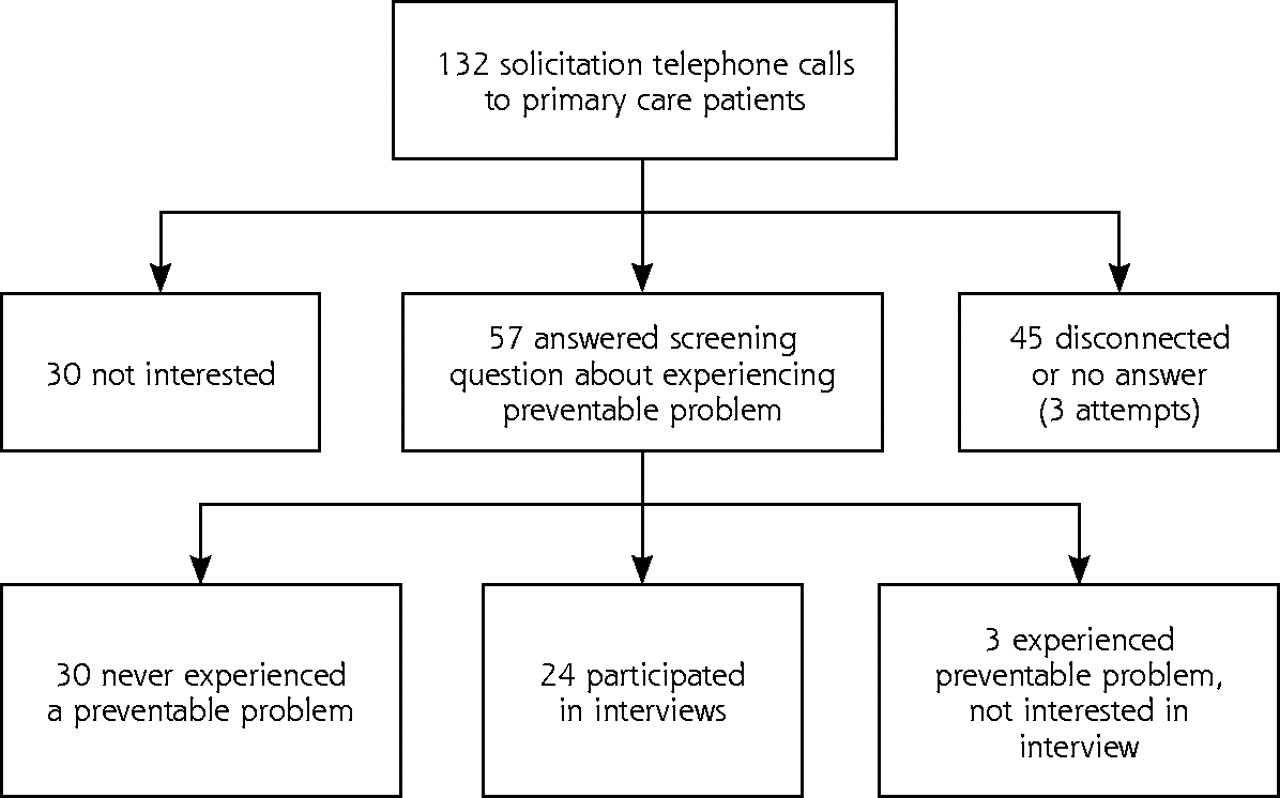
After approval from our institutional review board, we obtained from practice databases a random sample of telephone numbers of patients stratified by age (younger than 18 years, 18 to 65 years, and older than 65 years) and race (white, not white [primarily African American]). We chose maximum variation based on demographic data because there were no existing data on which to otherwise define a selective sample. We began with more than 15,000 patients’ telephone numbers and called patients from each stratified group until a respondent agreed to participate. We asked the person who answered (not necessarily the patient of record), “Have you or your child ever experienced a preventable problem with your primary care? Would you discuss it further with a researcher at a later time?” We continued calling patients, rotating through the stratified groups and soliciting participants, at the same time we were performing the interviews. When it became apparent that women were oversampled, we specifically asked to speak to men to maintain their representation. We assessed for data saturation through ongoing informal review of the interviews by the interviewer (NCE), a research assistant, and a medical anthropologist (CJJ). After 24 interviews, we believed patients were reporting no important new behaviors, and we stopped soliciting participants. To obtain these 24 interviews, we called 132 patients (Figure 1⇓).

Solicitation of local primary care patients to participate in the semistructured interviews.
Data Collection
Participants were interviewed in their homes or workplace by 1 investigator (NCE). She introduced herself as a physician researcher from the university. In the semistructured interviews, she asked participants to tell her (1) their stories of preventable problems, (2) why they thought it happened, (3) what they could have done to prevent it, (4) how they have changed how they interact with health care, and (5) what lessons they learned from the experience(s). The interview was developed from the medical literature8,23 with input from other patient safety researchers for face validity. She then asked for demographic data. The interviews lasted 15 to 45 minutes and were audiotaped and transcribed, with all identifying information removed. Although a brief analysis of the types of problems experienced is reported here for context, this article discusses the emotional and behavioral responses to experiencing these preventable problems.
Data Analysis
We performed our analysis in the editing style24,25 using QSR NVivo 2.0 (QSR International Pty Ltd, Doncaster, Victoria, Aust). In this method, while acknowledging our previous assumptions, we sorted the interview data into coding categories derived from the data, explicitly checking them against other categories and the original data, and then searched for patterns and themes.
Four researchers who had expertise in primary care (2 family physicians [NCE, TZ] in the same department, but in different clinical practices), sociology (LH), and medical anthropology (CJJ) provided a diverse team approach to the data. After all researchers reviewed and discussed 1 transcript, the senior author and 1 researcher read 12 transcripts and devised the initial coding categories, which were modified and then confirmed by all 4 researchers. Each transcript was then read and coded by the senior author and an additional researcher. During coding, categories were added or modified, as needed, as we drew on the original transcripts for meaningful segments of text.24 During dyad meetings each interview was discussed until consensus in coding was reached. Then, in a series of meetings, all the researchers reread and discussed the coding categories and the original data and developed themes and models related to emotional and behavioral responses in the face of experiencing preventable problems and errors.
RESULTS
Participants
Table 1⇓ displays the demographic characteristics of our 24 participants. Most (75%) were women, and their ages ranged from 20 to 81 years. The participants were equally divided between African American and white.
Participant Characteristics
Types of Preventable Problems Experienced
The 24 participants described experiencing 63 different preventable problems and errors, ranging from misdiagnosis to the inability to get a timely appointment (Table 2⇓). Office administration and communication problems were most frequently described. Nine participants reported experiencing 2 problems; 10 participants experienced 3 or more problems.
Preventable Problem Types Reported by Participants
Emotional Responses
The most common emotional response to experiencing preventable problems was anger; we frequently heard such statements as, “I was very, very disturbed,” and “I ain’t never been so mad before.” Mistrust was also commonly expressed, as expressed by, “… it’s hard to have faith anymore” in medicine, and “I am sort of distrustful of new doctors.” A sense of resignation, that “it hasn’t made any difference” or “I just let it go” was also common, but fear was mentioned only rarely.
Behavioral Responses
Participants expressed a number of behavioral responses to the problems they experienced. We classified these into 4 groups: avoidance, accommodation, anticipation and advocacy (Table 3⇓). Individual participants usually used several behaviors, depending on the specific situation. Although many responded with several behaviors within a category, or even from 2 or 3 categories, only rarely did a participant responded with behaviors from every category.
Behavioral Responses to Experiencing Perceived Medical Problems
Avoidance
Avoidance includes both a partial or total avoidance of the system. Responses included the following:
“I don’t interact (with doctors). I haven’t been back since” (44-year-old white man; physician-insurance company communication problem).
“I just don’t like to really be in the presence of doctors. I mean, like if I really don’t have to, I will just try to deal with what I have to deal with outside of them instead of going to the doctor” (27-year-old African American woman; nursing mistake and doctor-patient communication problem).
Others tried to navigate around the parts of the system where the problems occurred, such as avoiding the telephone or the office staff. Some avoided their current doctor, office, or hospital by switching to another one.
Accommodation
Accommodation includes behaviors by participants who simply put up with problems and often changed their own behaviors to adjust to the system. For example, long waits to be seen were dealt with by “bringing things for the kids to do—and lots of snacks, too.” Others believed that simply following the doctor’s advice closely was the best thing to do:
“Follow the doctor’s advice, he has been educated and he knows more about what to do than you do” (72-year-old white woman; procedural problem and doctor-patient communication problem).
Others just tolerated the mistakes: “I think it’s just one of those things that happened” (81-year-old white woman; medication problem).
Anticipation
Anticipation involves foreseeing problems and acting or reacting to them. This category of responses was the largest, and we subdivided it into attend to details, attend to emotions, acquire knowledge, and actively communicate.
Attending to details includes keeping track of and asking for the best appointment times, as well as paying attention to medicines and dosages, keeping a list of medicines and health problems, and even double-checking the prescription at the pharmacy:
“People should always read before they pop a pill in their mouth, they should always make sure it’s what they want” (34-year-old white man; medication problem).
Attending to emotions and paying attention to gut instinct were identified by many as important:
“Until basically somebody can tell you what you believe in your heart to be right, you just have to keep going” (42-year-old white woman; missed diagnosis and doctor-patient communication problem).
Acquiring knowledge includes consulting family, friends, books, and the Internet:
“Personally, things I do, I try to read books to see what is said. The children have computers, so I have them to look up something for me on the computer” (69-year-old African American woman; appointment problem).
Participants also stressed checking out a doctor ahead of time and using intelligent criteria to select a doctor.
Actively communicating with physicians and staff consists of giving a complete history, asking the doctor questions, and being assertive with the staff:
“I’m not afraid to ask any question about anything … whatever procedure that is going to be done; how it works. I know everything now. I’m not a bit shy anymore” (40-year-old white woman; office staff problems and doctor-insurance company communication problems).
Other participants pointed out the importance of communicating about expectations:
“I would say talk with your doctor and get more information.… I need to get with [my new doctor] and talk more about what is expected of me and how much can I expect from him” (74-year-old African American man; office telephone problems).
Advocacy
Advocacy behaviors involve patients actively seeking better care for themselves and others. Some participants simply spoke up for themselves, insisting on a second opinion, while others had become policy advocates:
“I also belong to an organization; well, we are a little organization … I have written to senators and congressmen” (72- year-old woman; broken equipment and doctor-patient communication problem).
Others focused on fighting for what they believed was right:
“I think first of all, you have to be assertive. I mean, you have to be firm. You can’t go in there being meek. I mean you want to be professional. You want to be kind, but you also want to get your point across” (55-year-old African American woman; office administration problem).
Emotional and Behavioral Relationships
As a qualitative study, our selection criteria for participation emphasized variability to achieve a wide range of responses to self-perceived preventable problems; we cannot quantify the types of responses by sex, age, or race. We did notice, however, that while anger and resignation were expressed by participants who used all types of behavioral responses, loss of trust was expressed most often by those who either avoid health care or use advocacy behaviors. For example, from a participant who generally avoids health care now:
“Sometimes I am kind of leery when I go. I am not as open as I was.… I go in now and just sort of watch them; before I would just go in and start talking” (44-year-old African American woman; doctor-patient communication problem).
And from a participant who now describes himself as a partner in care:
“I guess there was a period of time where I just kind of trusted the doctor to take care of me. Now what I determine is that I need to really become a partner in that process and to pull from his knowledge and stay, as much as I can, aware of what my situation is so that I can ask the right questions” (68-year-old African American man; office staff and doctor-patient communication problem).
DISCUSSION
After experiencing challenges that ranged from seemingly interminable telephone waits for refills or results to rude physicians to serious misdiagnoses, our participants responded to preventable problems primarily with anger, although, not surprisingly, we also heard expressions of both mistrust and resignation. These feelings were translated into a variety of behaviors ranging from avoidance to advocacy. Understanding how patients react to their experiences with preventable problems can assist health care both at the physician-patient and system levels. We believe the 2 most important messages from our study are that (1) experiencing a preventable problem affects trust, resulting in an association of mistrust with health behaviors; and (2) patient behavior in response to these problems has a potential impact on the provision of health care.
It is not surprising the patients respond to medical errors and preventable problems with distrust in physicians and the health care system. In a study of attitudes toward error by patients anticipating brain surgery, the authors note that, “we asked patients about their feelings toward medical error, but by and large, they chose voluntarily to talk about trust.”26 Problems experienced in the ambulatory setting have been strongly related to lower trust in physicians,27 as have poor physician communication and perceived lack of honesty and caring.28,29 Trust has been seen as a mitigator of patients’ level of concern about medical error,26 so it is reasonable that when patients believe they have experienced error or problems that should be preventable, they will lose trust. We noted this lack of trust most often from participants who described avoidance and advocacy response behaviors (Figure 2⇓). The medical literature confirms patients’ use of avoidance behaviors when their trust is low, including voluntarily leaving a practice, reduced rates of care seeking, and less use of medications and treatments.28,30 A lack of trust associated with advocacy behaviors is not mentioned in the medical literature. This association needs to be explored further in future studies, as does a direct causal link between loss of trust and change in behaviors.
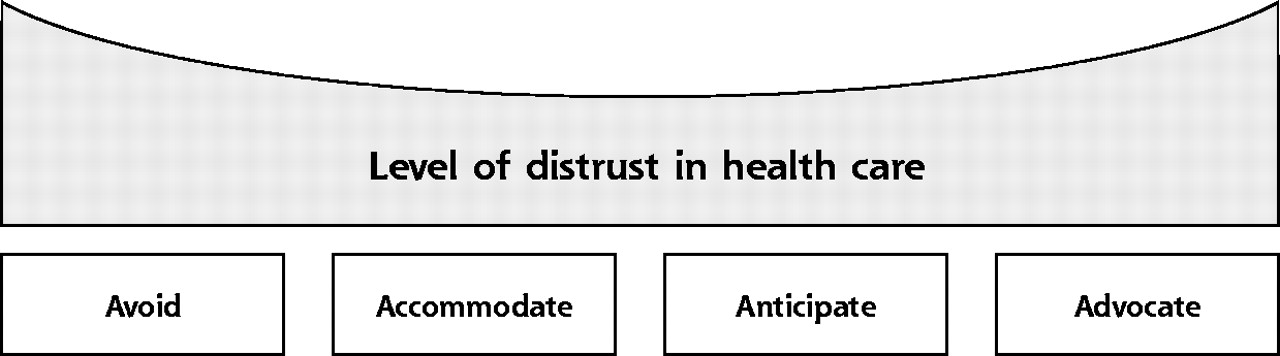
Model of behavioral responses relating to trust.
A proposed model of patients’ behavioral responses relating to trust in the health care system. Those who describe avoidance or advocacy behaviors after experiencing preventable problems were more likely to express loss of trust in aspects of health care.
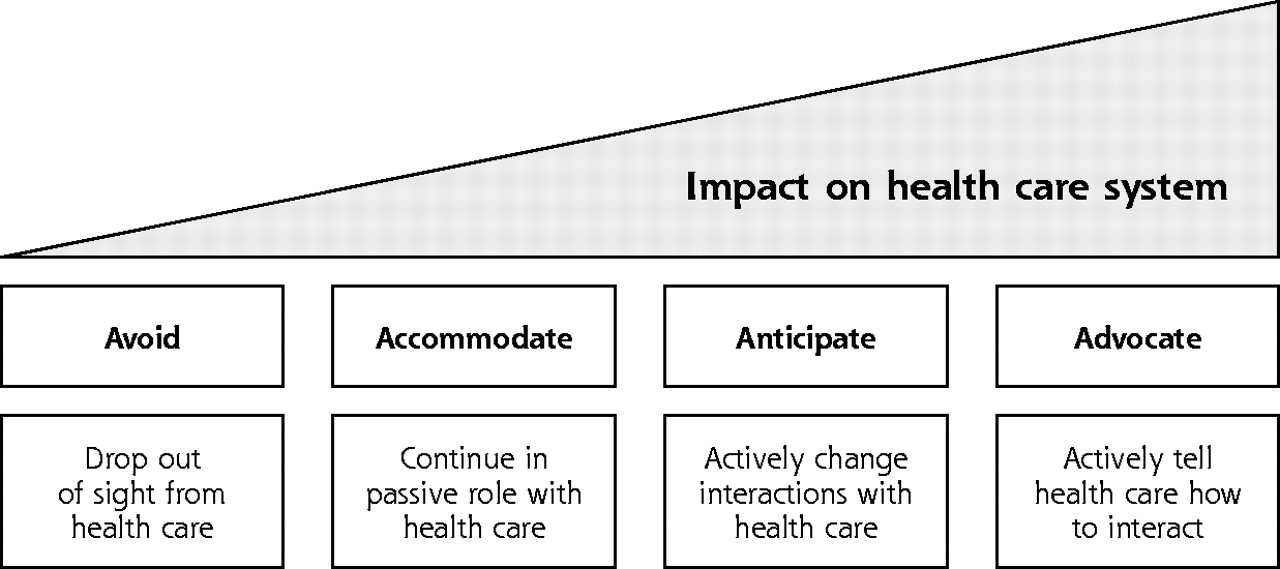
The range of steps made by our participants in the anticipation and advocacy categories echos many of the recommendations made by policy and patient safety experts.14–17 We propose that these behaviors may have a greater impact than avoidance or accommodation behaviors on how health care is provided (Figure 3⇓). Whereas both avoidance or accommodation are active—leaving a practice permanently is a big step for a patient—they may have little impact on a practice when done with no explanation. On the other hand, the behaviors of those who advocate for themselves or who have actively embraced self-education and communication may affect physicians and their practices. There is little in the medical literature on this topic. Organizational change is a complex process, and many models of change exist.31 Inherent to most of them, however, is the importance of having a tension for change, the belief that problems exist with current processes. Also important for change is an understanding of customers’ (or in this case, patients’) needs and concerns.31 Patients who actively advocate, educate, and communicate may be more likely to instill that tension and understanding in a practice or health care system. None of the current literature, however, appears to relate patient behaviors directly to changes in the practice of medicine. This possible connection needs to be better studied.

Model of behavioral responses relating to potential impact.
A proposed model of patients’ behavioral responses relating to their potential impact on health care practice. Those who described anticipation or advocacy behaviors after experiencing a preventable medical problem may be more likely to impact the practice of health care.
The only other published data on patients’ behavior changes in response to experiencing error, a 1997 survey commissioned by the National Patient Safety Foundation, found that the 3 most common safety precautions these patients now take are asking questions; researching the hospital, physician, or treatment; and getting a second opinion.12 These responses are consistent with those reported by our participants. Participants in our study went beyond these recommendations and noted the importance of dealing with the office system—from choosing the best times for appointments to dealing with difficult staff. These areas are often overlooked by policy experts and are important in primary care. Research is needed, however, to know whether patients who use these behaviors will have safer or higher quality of care. Many of our participants expressed a belief that their new way of acting has changed the quality of their care, but corroborating research is sketchy. There is evidence that patients can learn to be more active participants in their health care. Experience in chronic disease management,21,32,33 treatment adherence,19,34 health promotion,35 and communication skills training36,37 suggests that patients can change their behaviors in specific areas. At times these changed behaviors have been shown to improve outcomes.18,21,36 Advancing from these specific areas to improvement in patient safety is a common assumption, but especially in the complex world of primary care, more empiric research is needed.38
Although this study offers a qualitative glimpse into how patients respond to preventable problems in their primary care, there are limitations. Our participants were self-selected, and their experiences might not be generalizable to other primary care populations. Participants included a greater proportion of women than men despite our active recruitment of men. We may have missed some behaviors that men were more likely to adopt. Participants were asked to discuss any preventable problems in their primary care, so their stories are likely to be recent or memorable incidents, not necessarily all incidents that they may have experienced. Interviews were semistructured, but not limited by any time restraints. While this one-time approach to each participant limited our ability to probe deeply into some issues, such as the relative importance of the problem experience, other medical experiences, and media publicity of medical errors in shaping emotional response and behavioral change, we did allow participants sufficient time to tell their story, probing for areas the literature suggested possibly important in response to error.
We elected to use a broad definition of patient safety, allowing patients to self-determine preventable problems, and we elicited stories and experiences that others may believe fall outside the realm of safety and errors. We believe this broad definition is consistent with the medical literature6–8,23 and allowed us to obtain a complete picture of how patients responded to all types of preventable problems. To paraphrase Kuzel and colleagues,8 whether the label of errors applies may be less important than recognizing the emotional and behavioral responses to preventable problems associated with primary health care.
Participants shared their responses to a variety of self-perceived preventable problems. Although anger was present, and trust was lost in physicians and health care, many participants still developed proactive behaviors to help them avoid or minimize preventable problems in the future. Future research is necessary to identify which behaviors commonly performed by patients really improve their safety, and whether patients can learn to adopt these behaviors before they ever experience problematic care.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: Grant number R03 HS1345201 from the US Agency for Healthcare Research and Quality.
This work was a distinguished research presentation at the Annual Meeting of the Society for Teachers of Family Medicine, May, 2004.
- Received for publication January 20, 2005.
- Revision received April 25, 2005.
- Accepted for publication May 16, 2005.
- © 2005 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Effect of Three Key Administrative Errors on Patient Trust in Physicians: Prescription Errors, Confidentiality Breaches, and Appointment Errors
- Association of patients past misdiagnosis experiences with trust in their current physician: the TRUMP2-Net study
- Laboratory testing in general practice: a patient safety blind spot
- The Psychological Impact of a Colorectal Cancer Diagnosis Following a Negative Fecal Occult Blood Test Result
- Do older patients' perceptions of safety highlight barriers that could make their care safer during organisational care transfers?
- Rural Community Members' Perceptions of Harm from Medical Mistakes: A High Plains Research Network (HPRN) Study
- In This Issue: Trade-Offs, Time Use, Depression Care