
Abstract
PURPOSE We wanted to review systematically the efficacy, effectiveness, and safety of inhaled corticosteroids with respect to health outcomes in patients with chronic obstructive pulmonary disease (COPD).
METHODS We searched MEDLINE, EMBASE, The Cochrane Library, and the International Pharmaceutical Abstracts to identify relevant articles. We limited evidence to double-blinded randomized controlled trials (RCTs) for efficacy, but we also reviewed observational evidence for safety. Outcomes of interest were overall mortality, exacerbations, quality of life, functional capacity, and respiratory tract symptoms. When possible, we pooled data to estimate summary effects for each outcome.
RESULTS Thirteen double-blinded RCTs determined the efficacy of an inhaled corticosteroid compared with placebo; 11 additional studies assessed the safety of inhaled corticosteroid treatment in patients with asthma or COPD. Overall, COPD patients treated with inhaled corticosteroids experienced significantly fewer exacerbations than patients taking placebo (relative risk [RR] = 0.67; 95% CI, 0.59–0.77). No significant difference could be detected for overall mortality (RR = 0.81; 95% CI, 0.60–1.08). Evidence on quality of life, functional capacity, and respiratory tract symptoms is mixed. Adverse events were generally tolerable; pooled discontinuation rates did not differ significantly between inhaled corticosteroid and placebo treatment groups (RR = 0.92; 95% CI, 0.74–1.14). Observational evidence, however, indicates a dose-related risk of cataract and open-angle glaucoma. Severe adverse events, such as osteoporotic fractures, are rare; the clinical importance of the additional risk is questionable.
CONCLUSIONS Overall, the risk-benefit ratio appears to favor inhaled corticosteroid treatment in patients with moderate to severe COPD. Existing evidence does not indicate a treatment benefit for patients with mild COPD.
- Chronic obstructive pulmonary disease/drug therapy
- corticosteroids
- health outcomes
- systematic review
- meta-analysis
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is among the leading causes of morbidity and mortality worldwide.1 In 2000 COPD accounted for approximately 20.7 million outpatient visits, 3.4 million emergency department visits, 6.3 million hospitalizations, and 116,513 deaths in the United States.2 The World Health Organization estimates that by the year 2020, COPD will be the third-leading cause of death and the fifth-leading cause of disability worldwide.1
COPD is characterized by a progressive, irreversible limitation of airflow associated with an abnormal inflammatory response to noxious particles or gases. It is caused primarily by smoking.3,4
The beneficial effect of inhaled corticosteroid treatment for COPD remains controversial,3,5 in part because only smoking cessation is reliably shown to slow the rate of decline in lung function.4 Although the Food and Drug Administration (FDA) has not approved inhaled corticosteroids as monotherapy for the treatment of COPD, they are frequently prescribed to reduce or alleviate symptoms, increase exercise capacity, reduce the number and severity of exacerbations, and improve health status. The Global Initiative for Chronic Obstructive Lung Disease recommends inhaled corticosteroid treatment for patients with COPD who have a documented spirometric response to inhaled corticosteroids and for patients with moderate to severe COPD (forced expiratory volume in 1 second [FEV1] <50% predicted) who have repeated exacerbations that require treatment with antibiotics or oral corticosteroids.6 Inhaled corticosteroid treatment is, however, associated with rare but potentially serious adverse events, such as osteoporosis, glaucoma, and cataract, that are difficult to identify in efficacy studies.7
Six inhaled corticosteroids are available in the United States: beclomethasone dipropionate (beclomethasone), budesonide, flunisolide, fluticasone propionate (fluticasone), mometasone furoate (mometasone) and triamcinolone acetonide (triamcinolone). Table 1⇓ summarizes their generic names, trade names, manufacturers, dosage form with corresponding devices, strengths, and labeled uses.
Inhaled Corticosteroid Trade Names, Manufacturers, Formulations, and Labeled Uses
Most published studies and systematic reviews8–10 have evaluated the effect of inhaled corticosteroid treatment on FEV1 decline. The rate of FEV1 descent, however, is an imperfect surrogate outcome for clinically important health outcomes, such as health-related quality of life, functional capacity, and exacerbations.11 Only one meta-analysis focused primarily on health outcomes12; none of these systematic reviews took observational evidence for adverse events into consideration. Limiting adverse events assessment to randomized controlled trials (RCTs) risks missing rare but potentially severe adverse events, such as osteoporotic fractures, glaucoma, or cataract, which RCTs cannot reliably assess because of limitations of sample sizes and study durations.
The objective of this review is to determine the risk-benefit ratio of inhaled corticosteroid treatment for COPD by systematically reviewing the evidence on the efficacy, effectiveness, and safety of inhaled corticosteroid treatment in patients with COPD with respect to health outcomes. Contrary to previous systematic reviews, because our review incorporates observational evidence for adverse events, we provide the first comprehensive assessment of the risk-benefit ratio of inhaled corticosteroid treatment for COPD.
METHODS
This study is part of a larger systematic review of the comparative effectiveness and tolerability of inhaled corticosteroids in patients with asthma or COPD conducted for the Oregon Drug Effectiveness Review Project (DERP).13 We limited outcomes of interest a priori to health outcomes to assure clinical applicability of results.
We searched MEDLINE, EMBASE, The Cochrane Library, and the International Pharmaceutical Abstracts to identify relevant articles. We used either medical subject headings (MeSH or MH) as search terms when available or key words when appropriate. We combined terms for the selected indication (COPD) and adverse events with 6 specific inhaled corticosteroids (beclomethasone, budesonide, flunisolide, fluticasone, mometasone, and triamcinolone). We limited the electronic searches to “human” and “English language”; we searched sources from 1970 to 2005 (April) to capture literature relevant to the scope of our topic.
Two persons independently reviewed abstracts; if both reviewers agreed that the trial did not meet eligibility criteria, it was excluded. We reviewed the full text of all eligible articles. Double-blind RCTs of at least 6 months’ duration and an outpatient study population were eligible for inclusion. Preestablished exclusion criteria concerned study design or duration, patient population, interventions, and outcomes. We excluded open-label studies from the efficacy analysis because empirical evidence indicates that lack of blinding frequently leads to measurement bias and an overestimation of effect sizes.14 For adverse events we included both experimental and observational studies. For observational studies we included those with large sample sizes (>100 patients) that lasted at least 1 year and reported an included outcome. For adverse events we also included evidence from mixed populations with asthma and/or COPD.
We assessed the internal validity (quality) of trials based on predefined criteria from the US Preventive Services Task Force (ratings: good-fair-poor)15 and the National Health Service Centre for Reviews and Dissemination.16 External validity (generalizability) was assessed but did not influence quality ratings. We rated trials with a fatal flaw in one or more categories as poor quality and excluded them from the analysis; we rated trials that met all criteria as good quality. The majority of trials received a quality rating of fair. We accepted the definitions of exacerbation as reported in each study because we did not have access to individual patient data. Although definitions of exacerbation varied across studies, most defined it as an episode requiring oral or parenteral corticosteroids, antibiotics, emergency department visits, or hospitalizations because of increased respiratory tract symptoms.
When possible, we pooled data to obtain summary effect estimates for a given outcome, using relative risks to measure effect sizes. We used fixed-effects models for all meta-analysis because the observed heterogeneity was low (<20%, assessed using the I2 statistic). We assessed publication bias using funnel plots and Kendall’s tests, although the validity of these methods is limited given the small number of component studies. All analyses were conducted using Stats-Direct 2.3.8 (StatsDirect Ltd, Sale, Cheshire, UK).
RESULTS
Overall we identified 880 citations. Figure 1⇓ illustrates the disposition of citations and articles. Thirteen double-blinded RCTs determined the efficacy of an inhaled corticosteroid compared with placebo in patients with COPD. We excluded 1 study for quality reasons because of a high rate of postrandomization exclusions.17 We included 11 additional studies conducted in adult patients with COPD or asthma to assess the risk of adverse events of long-term inhaled corticosteroid use.
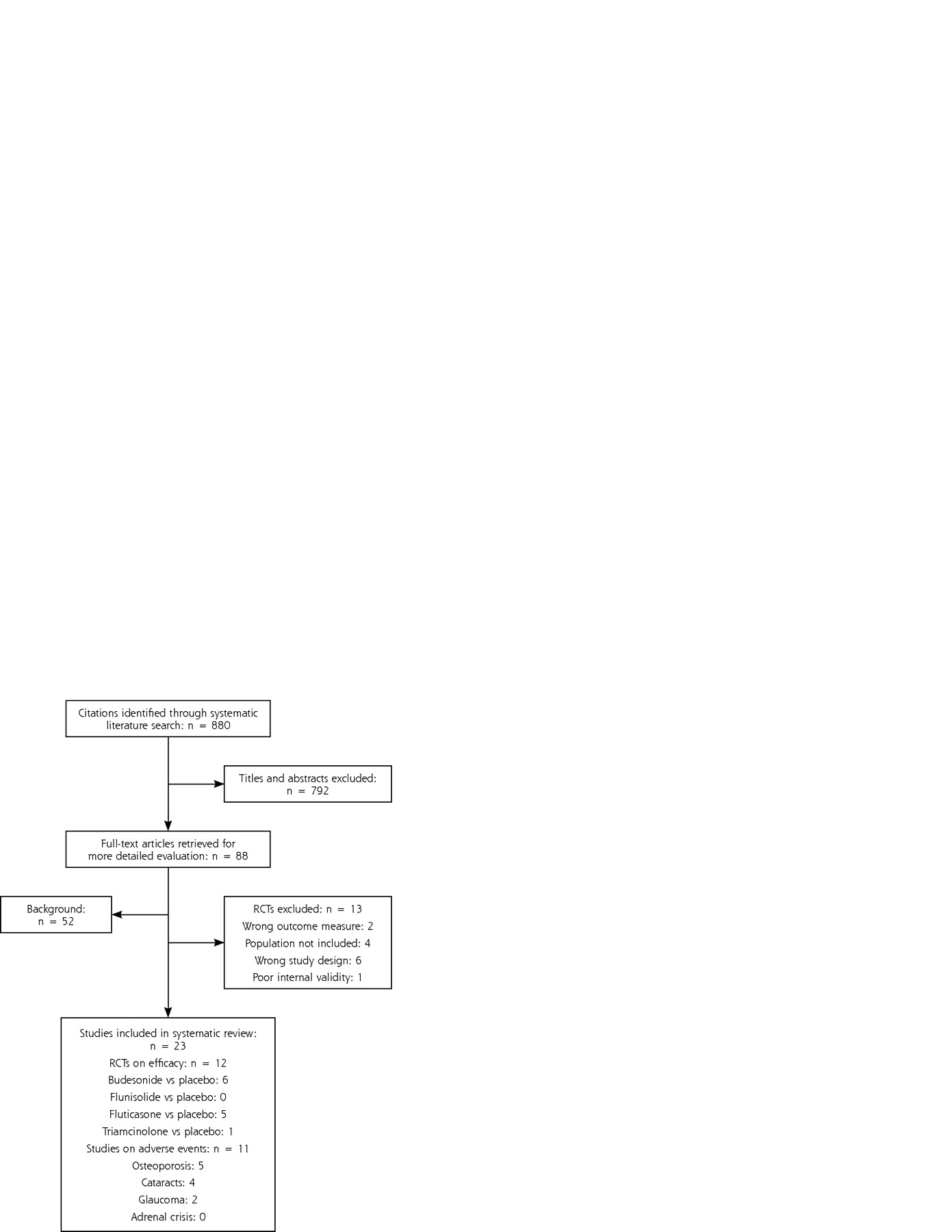
Results of literature search.
Tables 2⇓ and 3⇓ describe included studies.18–40 In efficacy studies, patients were generally smokers or former smokers with a clinical diagnosis of COPD. Only the Copenhagen City Lung Study enrolled smokers identified as having mild COPD during a random population survey and subsequent respiratory system screening.23 Severity of COPD varied from mild to severe across studies; inclusion criteria tended to exclude patients with asthma or good bronchodilator responsiveness. Patients with a history of asthma, allergic disease, or sudden onset of breathlessness were excluded from all studies. Further, FEV1 reversibility after bronchodilator use was frequently assessed before enrollment; cutoff criteria were between 10% and 15%. Nine trials (69%) were funded by pharmaceutical companies and 3 (23%) were supported primarily by governmental agencies or independent funds; 1 study (7%) did not report funding source.
Summary of Included Randomized Controlled Trials on Efficacy of Inhaled Corticosteroids in COPD
Summary of Included Studies on Adverse Events of Inhaled Corticosteroids in COPD
Exacerbations
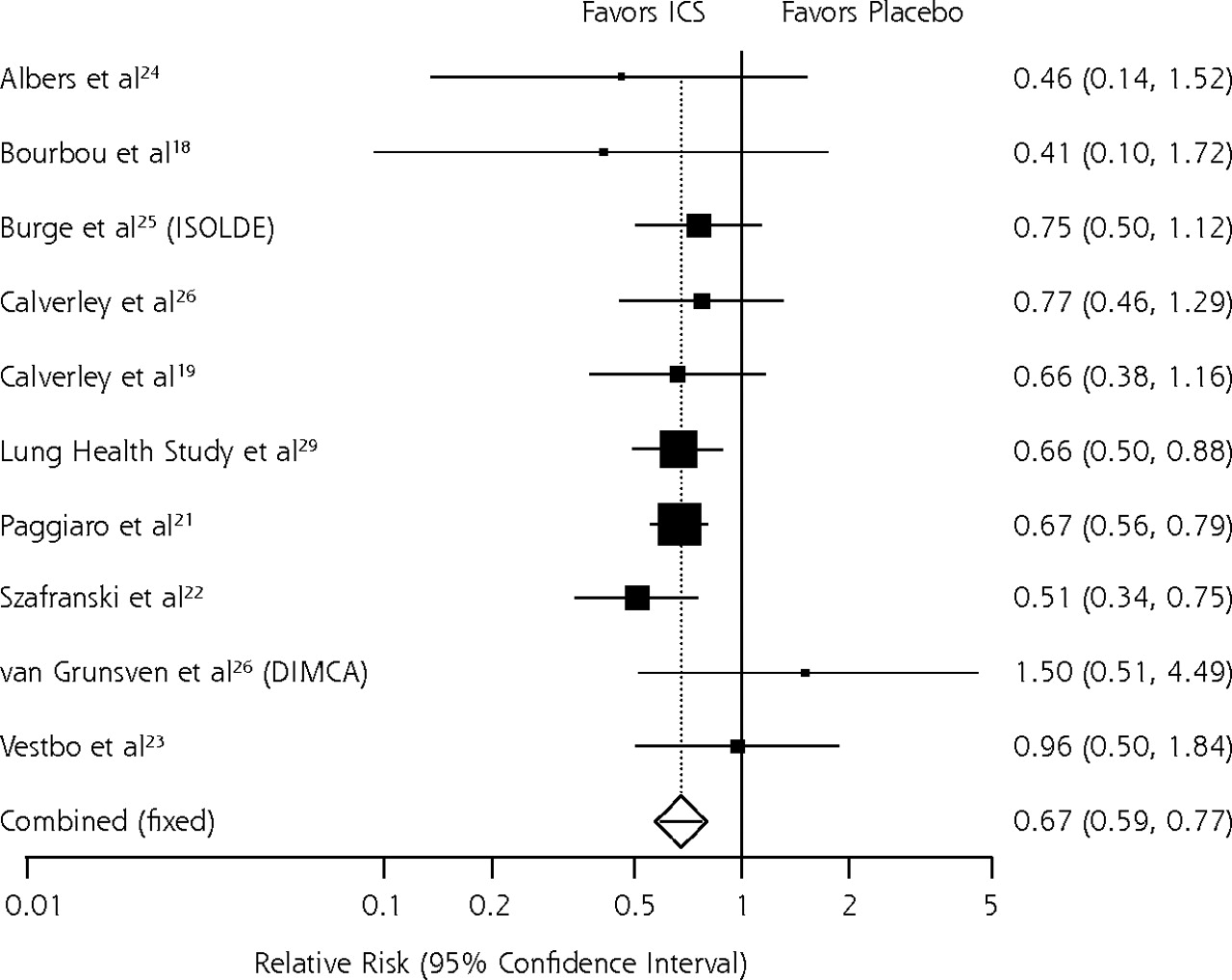
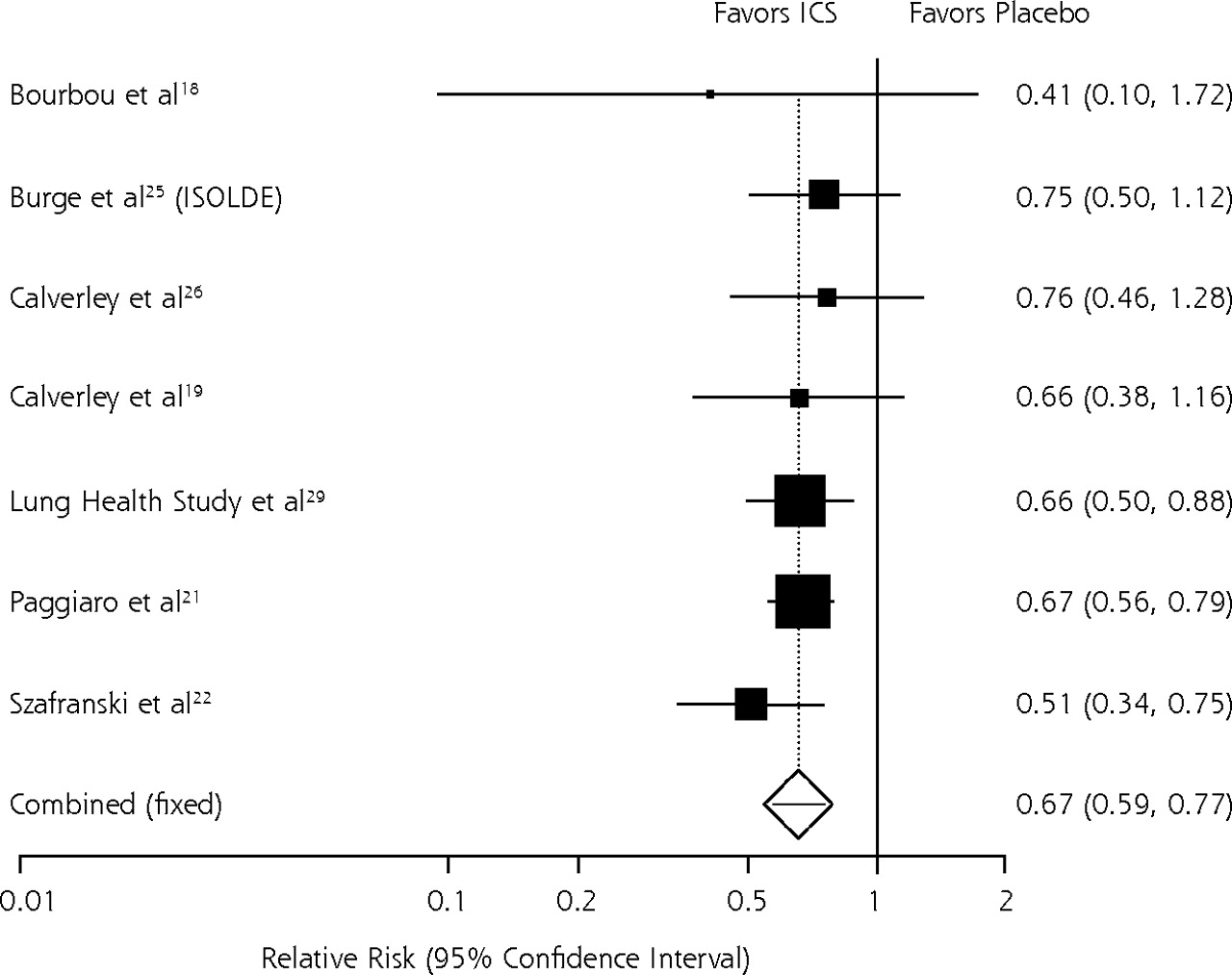
Two studies did not provide sufficient data on exacerbation rates and could not be included in the meta-analyses.20,21 Overall, pooled results of 4,300 patients from the 10 remaining trials showed a 33% reduction (95% CI, 23%–41%; RR = 0.67; 95% CI, 0.59–0.77) in COPD exacerbation rates over a mean follow-up period of 20.8 months (Figure 2A⇓). Sensitivity analysis showed that this treatment effect derives largely from studies in populations suffering from moderate to severe COPD (respectively, FEV1 ≥50% to <80% predicted and FEV1 <50% predicted according to American Thoracic Association criteria).41 Limiting the analysis to the 7 trials with populations with moderate to severe COPD (ie, excluding populations with mild COPD) produces an estimated benefit of inhaled corticosteroid treatment almost identical to the results of the overall meta-analysis (RR = 0.66; 95% CI, 0.57–0.75) (Figure 2B⇓). The number needed to treat (NNT) in this population is 12 (95% CI, 9–18); ie, 12 patients with moderate to severe COPD need to be treated with an inhaled corticosteroid for 17.7 months to avoid 1 exacerbation. For the population with mild COPD (FEV1 ≥80% predicted), we pooled results of 3 small studies (n = 191); no benefit of inhaled corticosteroid treatment emerged (RR = 0.92; 95% CI, 0.55–1.53). As noted, the sample size of this analysis is small, and point estimates of both subgroup analyses are within each other’s confidence intervals. Inferences about differences of treatment effects must be made cautiously.
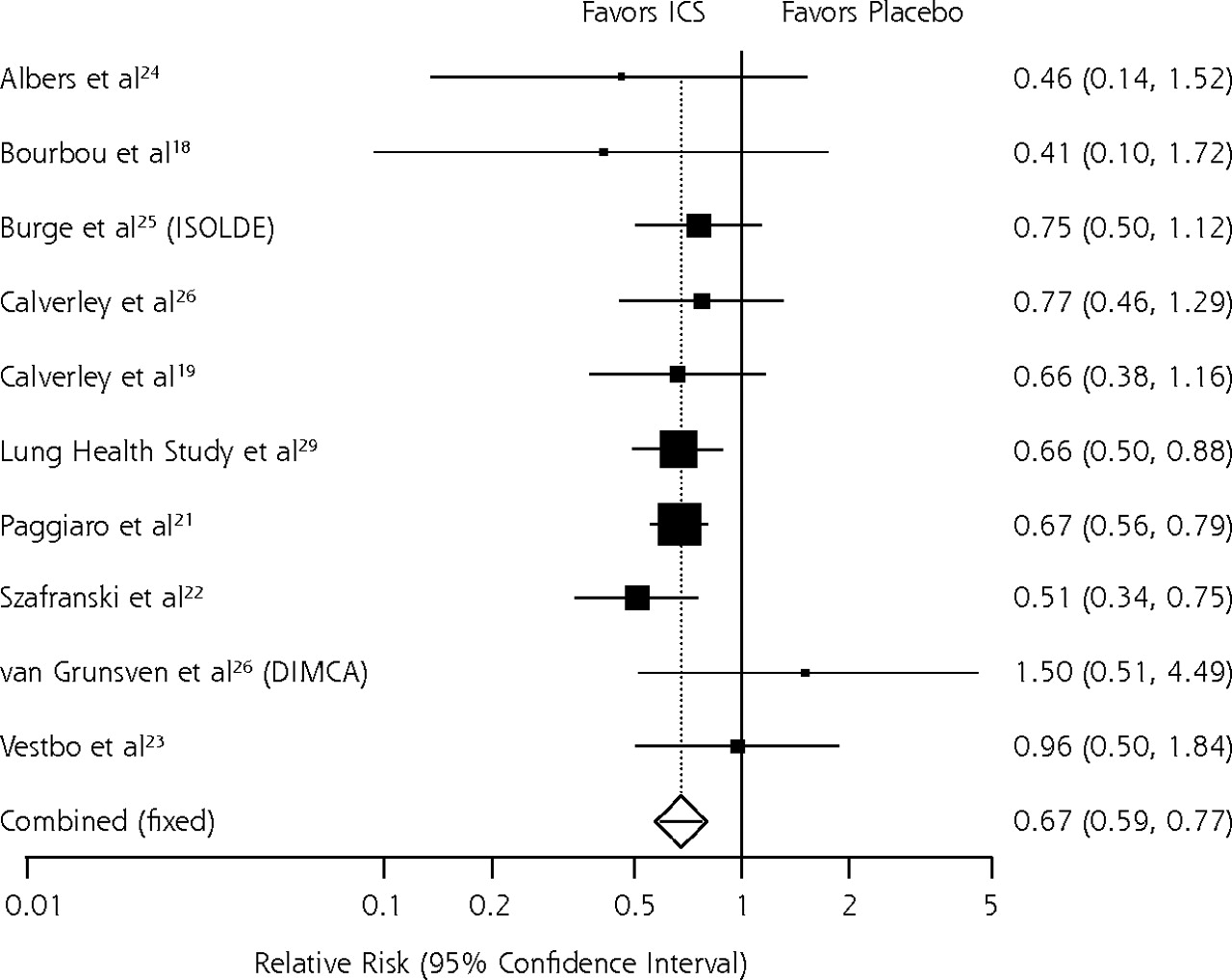

Relative risk meta-analysis of effects of inhaled corticosteroids on exacerbations.
COPD = chronic obstructive pulmonary disease; DPI = dry powder inhaler; MDI = metered dose inhaler.
In sensitivity analyses we compared pooled results of studies of newer inhaled corticosteroids (ie, fluticasone) that have a large degree of first-pass metabolism42,43 with those of older inhaled corticosteroids (ie, beclomethasone, budesonide, flunisolide, and triamcinolone). Relative benefits of both groups were almost identical (newer inhaled corticosteroids: RR = 0.69 [0.59–0.80]; older inhaled corticosteroids: RR = 0.65 [95% CI, 0.53–0.79]).
Mortality
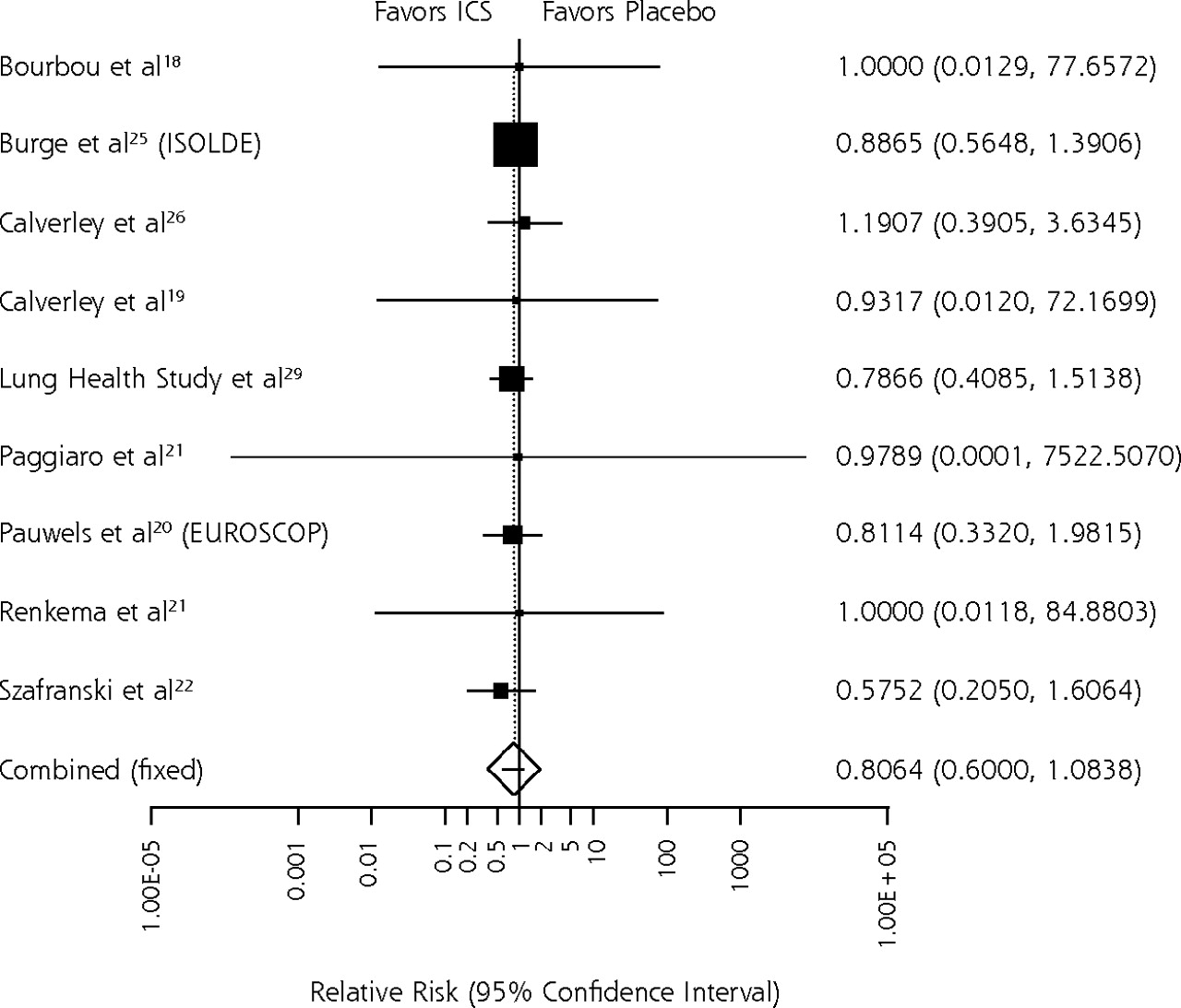
The pooled relative risks (RR = 0.81; 95% CI, 0.60–1.08) for 4,370 patients resulted in no significant difference in all-cause mortality (Figure 3A⇓). Overall, 2.9% of patients on placebo and 2.5% of patients on inhaled corticosteroids died (P = .27) during the mean follow-up period of 22.3 months. Limiting the analysis to studies of moderate to severe COPD (Figure 3B⇓) yielded almost identical results (RR = 0.84; 95% CI, 0.61–1.15). No differences in mortality were apparent between groups taking newer and older inhaled corticosteroids.


Relative risk meta-analysis of effects of inhaled corticosteroids: all-cause mortality.
ICS = inhaled corticosteroid; COPD = chronic obstructive pulmonary disease.
Functional Capacity and Quality of Life
In the few studies that assessed functional capacity or quality of life, outcome measures were too heterogeneous to pool results in a meta-analysis; therefore, we analyzed findings qualitatively.
Five studies examined functional capacity and quality of life in patients with moderate to severe COPD.18,19,22,26,27 Two trials administered a 6-minute walking test after 6 months of inhaled corticosteroid treatment. In one, 6-minute walking distance was significantly greater for patients on fluticasone 1,000 mg/d than for patients on placebo (+27 m vs +9 m; P = .032).27 A smaller Canadian study did not detect any significant difference in walking distances for patients when comparing budesonide 1,600 mg/d with placebo (−15 m vs +13 m; P = NR).18 This trial also reported no significant differences in scores on the Chronic Respiratory Disease Questionnaire. Three studies of patients with severe COPD reported greater improvements in St. George’s Respiratory Questionnaire for patients on budesonide 800 mg/d or fluticasone 1,000 μg/d than for patients on placebo19,22,26; however, the clinical importance of the reported differences (range: −0.8 to −3.0) is uncertain.
Two Dutch studies originating from the DIMCA (Detection, Intervention, and Monitoring of COPD and Asthma) program, which recruited patients with mild COPD through population screening, did not find any differences in functional capacity for patients on fluticasone 500 mg/d and those on placebo after 2 years of treatment.24,28
Respiratory Symptoms
Most studies assessed respiratory system symptom scores, but the reported data were mixed and insufficient for meta-analysis. Four studies reported no significant differences in respiratory system symptoms when comparing inhaled corticosteroid with placebo.18,23,26,28 Three studies detected no overall differences in respiratory systems symptoms but did detect significant improvements in subscales, such as daily cough scores, sputum volume,27 night time awakenings,19 and dyspnea.29 In comparisons with placebo, 1 trial reported significantly lower symptom scores in patients during 2 years’ treatment with budesonide 1,600 mg/d21 and another during 3 years’ treatment with fluticasone 1,000mg/d.25
Adverse Events
Efficacy trials commonly reported rhinitis, oral candidiasis, sore throat, bruising, hoarseness, headache, cough, bronchitis, and upper respiratory infection. In most studies, incidence was below 10%. Pooled discontinuation rates because of adverse events did not differ significantly between inhaled corticosteroids and placebo (RR = 0.92; 95% CI, 0.74–1.14). Most studies combined patient-reported adverse events with a regular clinical examination by an investigator. Short study durations and small sample sizes limited the validity of adverse events assessment in many trials. Many studies excluded eligible participants that did not tolerate treatment during the run-in period, limiting the generalizability of adverse events assessment.
To take the limitations of RCTs into consideration and to assess rare but potentially serious adverse events, we also reviewed observational studies (Table 3⇑). Specifically, we were interested in osteoporosis, posterior subcapsular cataracts, ocular hypertension, and open-angle glaucoma.
Bone Density and Osteoporotic Fractures
Overall, the evidence of an association between inhaled corticosteroid products and osteoporosis is mixed. A meta-analysis of randomized trials found no evidence of increased risk of loss of bone mineral density (BMD) or fractures,30 which is consistent with findings from an RCT not included in that meta-analysis.20,33
The strongest observational evidence comes from 2 case-control studies that measured fractures31,34; both reported a slight increase in the risk of fracture for inhaled corticosteroid-treated patients. In 1 study, only current high-dose users (≥700 μg/d) had an increased risk of nonvertebral fractures (OR = 1.68; 95% CI, 1.10–2.57).34 In the other, the risk of hip fracture was significantly higher in patients using an inhaled corticosteroid (OR = 1.19; 95% CI, 1.10–1.28). Additionally, evidence of an inhaled corticosteroid-associated reduction in BMD comes from a prospective cohort study in 109 premenopausal women32: an estimated bone loss of 0.00044 g/cm2 per puff per year of treatment. We view BMD as an intermediate outcome measure of osteoporosis; although a causal relationship exists between loss of BMD and risk of fractures from osteoporosis, the clinical importance of modest changes in BMD is often questionable.
Cataracts
The association between systemic corticosteroids and cataracts, especially at high doses administered for extended periods, is well documented in both children44 and adults.45 Systemic corticosteroid-induced cataracts typically are located on the posterior side of the lens and are referred to as posterior subcapsular cataracts.
Four observational studies evaluated the risk of adult patients developing cataracts, comparing nonspecific inhaled corticosteroid use with no inhaled corticosteroid use.35–38
A British case-control study of 15,479 patients with cataracts detected a modest but significant increase in risk for the overall use of inhaled corticosteroids (adjusted OR = 1.10; 95% CI, 1.00–1.20).38 A subgroup analysis of COPD patients, however, showed no significant increase in risk (adjusted OR = 1.03; 95% CI, 0.94–1.13). These results suggest a cumulative risk of inhaled corticosteroid use for the development of cataracts, because patients with asthma are generally exposed to inhaled corticosteroids for longer periods of their lives than are patients with COPD.
These findings are consistent with other observational evidence in patients with asthma or COPD. A retrospective cohort study with a nested case-control study,37 a case-control study,36 and a cross-sectional study35 reported increased dose- and duration-dependent risks of inhaled corticosteroids use for posterior cataract. These studies do not report on COPD patients alone.
Ocular Hypertension and Open-Angle Glaucoma
In 1 case-control study of 48,118 Canadians aged 66 years and older39 and 1 cross-sectional population-based eye study of 3,654 Australians aged 49 to 97 years,40 the risk of increased intraocular pressure or open-angle glaucoma was compared in patients using inhaled corticosteroids and patients not using inhaled corticosteroids. Both studies adjusted for age, sex, oral steroid use, history of diabetes, and history of hypertension but did not stratify by COPD patients. Both reported a dose-related increase in the risk of open-angle glaucoma for inhaled corticosteroid-treated patients compared with patients who had not used an inhaled corticosteroid.39,40 The case-control study observed this relationship only among current users of high doses of inhaled corticosteroids prescribed regularly for 3 or more months (adjusted OR = 1.44; 95% CI, 1.01–2.06)39; patients on low to medium doses did not have an increased risk (adjusted OR = 0.95; 95% CI, 0.77–1.19). In the cross-sectional study the association between ever using inhaled corticosteroids and elevated intraocular pressure or glaucoma occurred only in patients with a family history of glaucoma (OR = 2.8; 95% CI, 1.2–6.8).40
DISCUSSION
Our meta-analysis suggests that COPD patients treated with inhaled corticosteroids experience significantly fewer exacerbations than patients on placebo. The relative risk reduction is 33%; the NNT to prevent 1 exacerbation during 20.8 months is 12. This treatment effect is apparently stronger in patients with moderate to severe COPD. Pooled estimates for patients with mild COPD did not suggest a reduction of exacerbations. Sample sizes are too small, however, for clear inferences about the efficacy of inhaled corticosteroid treatment in patients with mild COPD.
We could not detect a significant benefit of inhaled corticosteroid treatment with respect to overall mortality, which in part may be attributable to short study durations (maximum 3 years) relative to the long natural course of disease and to the lack of power to detect such an outcome. We chose overall mortality as an outcome measure rather than COPD mortality, as it does not depend on a subjective judgment by outcome assessors and is therefore less prone to bias. The body of evidence concerning quality of life and functional capacity is mixed and yields no basis for clear conclusions. Empirical evidence suggests, however, that patient quality of life is related to the frequency of COPD exacerbation.46,47 Thus, fewer exacerbations resulting from inhaled corticosteroid treatment can provide indirect evidence for improved quality of life. In addition, inhaled corticosteroid treatment will spare some patients from dealing with systemic corticosteroids.
Efficacy data indicate that adverse events are usually mild and do not lead to significantly higher discontinuation rates for inhaled corticosteroid-treated than for placebo-treated patients. Osteoporotic fractures are rare; the clinical importance of the additional risk is questionable. Evidence from large observational studies consistently indicates a modest risk of cataracts and open-angle glaucoma; it is attributable largely to high dosage and long duration of inhaled corticosteroid use.
Our findings are partly consistent with earlier meta-analyses that assessed exacerbation rates.9,12 Van Grunsven et al9 reported no significant differences in exacerbation rates between the group on inhaled corticosteroids and the group on placebo. Results of a meta-analysis by Sin et al12 are consistent with our findings. Point estimates from our analyses, however, are more precise because of the greater number of component studies. Furthermore, neither of the 2 previous reviews included observational evidence for adverse events to assess the risk-benefit ratio of inhaled corticosteroid treatment. Results of long-term observational studies with respect to exacerbations and mortality are mixed.48–53 The COPE study, a double-blind discontinuation study of fluticasone (1,000 μg/d), reported that patients who discontinued inhaled corticosteroid therapy had a significantly higher recurrence risk of exacerbations than patients who remained on fluticasone treatment.49
We note several limitations in this literature and our work. Durations of efficacy studies are usually too short and sample sizes too small to assess reliably the effects on rare long-term outcomes (eg, mortality) and on rare but severe adverse events. Observational studies posed methodological concerns that precluded meta-analysis.
Because we did not have access to individual patient data, we assumed that definitions of exacerbations did not differ substantially across trials. Although this assumption could lead to some imprecision with respect to efficacy, it might also increase external validity because it synthesizes various definitions of exacerbation used in clinical practice. Moreover, we reviewed inhaled corticosteroids as a class, not taking differences in potency, delivery device, systemic exposure, and dosing into consideration. No treatment regimen appeared to be underdosed; however, because we could not conduct quantitative analyses on adverse events, we were unable to assess whether inhaled corticosteroids with low systemic absorption lead to fewer adverse events than inhaled corticosteroids with high systemic absorption. Our pooled efficacy results might underestimate treatment effects for patients with severe COPD who usually receive high-dose treatments. Differential loss to follow-up might also dilute treatment effects. Placebo groups consistently had a higher dropout rate than inhaled corticosteroid groups. The frequency of exacerbations and mortality might therefore be underestimated for placebo treatment.
None of the included studies can be viewed as an effectiveness trial with a high degree of generalizability. The patient populations often were highly selected and included exclusively current or former smokers. Patients with FEV1 reversibility of more than 10% to 15% were typically excluded. These factors further limit the generalizability of results for non-smoking patients with asthma who have chronic airways obstruction. Even so, good evidence exists from multiple trials that inhaled corticosteroid treatment is efficacious in patients with asthmatic features.13
Finally, we could not include unpublished studies; their absence may lead to an overestimation of treatment effects.
Additional large studies are needed that have the necessary power to address such health outcomes as mortality and quality of life. Results of the ongoing TORCH (Towards a Revolution in COPD Health) survival study may provide answers to some remaining questions.54 This 3-year, multicenter trial is randomizing approximately 6,200 patients with moderate to severe COPD to placebo, fluticasone, fluticasone/salmeterol, or salmeterol; it will end in 2006.
Acknowledgments
We would like to thank Timothy Carey, MD, MPH, who provided insightful comments on various drafts of this paper.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: Funding for this research was provided to the Cecil G. Sheps Center for Health Services Research through a subcontract with the Center for Evidence-Based Policy; Oregon Health & Science University.
- Received for publication June 9, 2005.
- Revision received September 27, 2005.
- Accepted for publication October 27, 2005.
- © 2006 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Inhalation devices and inhaled corticosteroids particle size influence on severe pneumonia in patients with chronic obstructive pulmonary disease: a nationwide cohort study
- Inhaled corticosteroids and the risk of lung cancer in COPD: a population-based cohort study
- Where current pharmacological therapies fall short in COPD: symptom control is not enough
- Statin use is associated with reduced mortality in COPD
- On TRACK: Medical Research Must Consider Context and Complexity
- In This Issue: Communication in the Era of 'Personalized' Medicine