
Abstract
PURPOSE In evaluating complaints suggestive of rhinosinusitis, family physicians have to rely chiefly on the findings of a history, a physical examination, and plain radiographs. Yet, evidence of the value of signs, symptoms, or radiographs in the management of these patients is sparse. We aimed to determine whether clinical signs and symptoms or radiographic findings can predict the duration of the illness, the effect of antibiotic treatment, or both.
METHODS We analyzed data from 300 patients with rhinosinusitis-like complaints participating in a randomized controlled trial comparing amoxicillin with placebo. We used Cox regression analysis to assess the association between the presence at baseline of rhinosinusitis signs and symptoms or an abnormal radiograph and the subsequent course of the illness. We then tested for interactions to assess whether the presence of any of these findings predicted a beneficial effect of antibiotic treatment.
RESULTS Two factors at baseline were independently associated with a prolonged course of the illness: a general feeling of illness (hazard ratio = 0.77, 95% confidence interval, 0.60–0.99) and reduced productivity (hazard ratio = 0.68, 95% confidence interval, 0.53–0.88). Neither typical sinusitis signs and symptoms nor abnormal radiographs had any prognostic value. Prognosis remained unchanged whether or not patients were treated with antibiotics, no matter what symptoms patients had at baseline.
CONCLUSIONS In a large group of average patients with rhinosinusitis, neither the presence of typical signs or symptoms nor an abnormal radiograph provided information with regard to the prognosis or the effect of amoxicillin. The time to recovery was longer in patients who felt ill at baseline or who did not feel able to work, but the course of their illness was not influenced by antibiotic treatment.
- Acute sinusitis
- family practice
- antibiotics
- respiratory tract infections
- prognosis
- signs and symptoms, respiratory
- radiography
- practice-based research
Annals Journal Club selection—see inside back cover or http://www.annfammed.org/AJC/.
INTRODUCTION
Acute rhinosinusitis is a common disease in family practice.1 Most practice guidelines agree that for the vast majority of patients, antibiotics are not necessary. Yet, a number of placebo-controlled randomized trials have demonstrated a (limited) positive effect of antibiotics.2–5 This evidence suggests that in a small minority of patients—generally those described as having acute “bacterial” rhinosinusitis—antibiotics can be beneficial. The problem is how to identify these patients.
Sinus puncture and computed tomography (CT) imaging are considered the reference standards for diagnosing acute bacterial rhinosinusitis.6 These procedures cannot routinely be performed in daily general practice, however, because they are too painful, too elaborate, or too expensive. A better understanding of the correlation between the results of sinus puncture or CT imaging and signs and symptoms would allow clinicians to identify patients who could benefit from antibiotic treatment. Several diagnostic studies have investigated this correlation,7–9 but their results were too divergent to formulate clear-cut practice recommendations.
In this study, we looked at this problem from a pragmatic point of view. For a family physician, it is presumably more important to know the patient’s prognosis and whether the patient might benefit from antibiotics than to know the exact diagnosis. Only a few studies have focused on these questions, however.10–12 The goal of our study was to search for clues to identify patients with suspected rhinosinusitis who are at risk for a prolonged course of illness and who could benefit from antibiotic therapy. We had 2 research questions: (1) In patients with suspected acute rhinosinusitis, can signs, symptoms, or radiographic abnormalities predict a prolonged course of illness? and (2) Can signs, symptoms, or radiographic abnormalities predict a beneficial effect of amoxicillin treatment?
METHODS
Population
We performed a secondary analysis of data from a randomized controlled trial (RCT).13 Between October 1998 and December 1999, 69 family physicians in Flanders, Belgium, enrolled in this trial patients meeting 3 inclusion criteria: aged 12 years or older, a respiratory tract infection as the presenting complaint, and self-reported purulent rhinorrhea. Exclusion criteria were allergy to penicillin or ampicillin; receipt of antibiotic treatment within the previous week; complaints lasting for more than 30 days; abnormality on chest examination; signs of complicated sinusitis (facial edema or cellulitis; orbital, visual, meningeal, or cerebral signs); pregnancy or lactation; comorbidity that might impair immune competence; and inability to follow the protocol because of language or mental problems. Enrolled patients were randomly assigned to receive amoxicillin 500 mg 3 times a day or placebo for 10 days. The 2 groups were comparable in every relevant aspect. More details on the methodology of this study have been published elsewhere.13
We conducted the present analyses in the subgroup of patients who had—in addition to purulent rhinorrhea—at least 1 of the following symptoms indicating acute rhinosinusitis: unilateral facial pain, pain in the upper teeth, visible purulent rhinorrhea, and a biphasic illness history (ie, after initially improving, the condition worsened again). We selected these signs and symptoms because they have been associated with rhinosinusitis in diagnostic trials of high quality.6,8 Our study was approved by the Ethics Committee of Ghent University Hospital.
Baseline Measurements and Follow-up
On the day of enrollment, patients completed a questionnaire, were physically examined by their family physician, and were offered an optional radiographic examination of their maxillary sinuses. On the questionnaires, they rated the severity of individual symptoms on a 6-point scale ranging from 0 (“absent”) to 5 (“worst that it can be”). During the 10 days of treatment, they recorded daily their general feeling of illness using a 4-point scale (good, a little ill, ill, very ill). Patients who had recovered on day 10 stopped filling out the diary. Patients who had not recovered on day 10 were asked to continue keeping the diary until day 15. The prognostic influence of the following variables was studied during the 15 days after enrollment: patient characteristics (sex and age); signs of sinusitis (visible purulent rhinorrhea, postnasal drip, elevated body temperature [≥37.5°C measured and recorded by the patient or family physician]); symptoms of sinusitis (pain on bending, unilateral facial pain, pain in the upper teeth, biphasic illness history, complaints lasting 7 days or more); general symptoms (fatigue, general feeling of illness, reduced productivity); an abnormal radiograph; treatment (amoxicillin); and a summary score of clinical findings (described below).
Data Analysis
We considered a symptom to be present if a patient gave it a score of 3 or higher on the 6-point severity scale, which meant that the patient subjectively perceived the symptom as “moderately severe,” “severe,” or “worst that it can be.” Patients had a general feeling of illness if they stated on the day of enrollment that they felt ill or very ill. Radiographs were considered abnormal if they showed mucosal thickening of at least 6 mm, an air-fluid level, or total opacity. To calculate the clinical sum score, each sign or symptom was attributed 1 point when present, and all points were added for each patient. Possible sum scores therefore ranged from 0 to 8 points.
We used SPSS-11 (Statistical Package for the Social Sciences, ver 11; SPSS Inc, Chicago, Ill) to perform Cox proportional hazards regression analysis.14 The outcome measure of this analysis is the hazard ratio: the ratio between the instantaneous event rate in patients with and without the studied prognostic variable. We defined the event as recovery (ie, the patient indicated in his or her diary feeling generally “well” again. Recovery time was the number of sequential days between the first contact with the family physician and the day of recovery. In this analysis, if a variable is associated with a hazard ratio of less than 1, the course of the illness is prolonged when that variable is present.
We performed 3 analyses. First, we conducted bivariate analyses to estimate the crude hazard ratios, with 95% confidence intervals (CIs), for each variable separately. Second, we included predictive factors with a P value of less than .2 in the bivariate analysis in a stepwise (backward and forward) multivariate Cox regression model to determine which variables were independent predictors of the speed of recovery. Third, we tested for an interaction between each variable and the treatment group by using a multivariate model (variable + treatment + variable × treatment). An interaction between 2 variables indicates that the influence on the prognosis of 1 variable depends on the value of the other variable. In our case, a significant interaction would mean that the impact of antibiotic treatment on the duration of the illness depends on the presence of a prognostic variable (eg, antibiotics shorten illness duration more in patients with prognostic symptom x).
The number of events was sufficiently large to detect a difference in recovery rate of at least 15% for any variable (α = .05, power 1 − β = .80). In the multivariate analysis, there were 49 events per included variable. For variables independently influencing the course of illness, we tested the Cox proportional hazard assumptions graphically by the complementary log transformation plot, and these assumptions were sufficiently met.14
RESULTS
RTC Population
A total of 416 patients were enrolled in the original RCT.13 To ascertain the representativeness of the included population, we checked for possible recruitment bias caused by noninclusion in 3 ways. First, we determined that the characteristics and symptom severity of patients enrolled by family physicians recruiting fewer patients (for whom more selection can be expected) did not differ from those of patients enrolled by family physicians recruiting more patients. Second, we analyzed data from questionnaires (sex, age, body temperature, severity of nasal discharge and pain, reason for nonrecruitment) for all eligible patients who were not included during the 6-week period and found that included and excluded patients were very much alike. The included patients were slightly more likely to report pain than the 332 eligible patents who were excluded (58% vs 50%; relative risk = 1.2, 95% CI, 1.0–1.42; P = .03). The most frequent reasons for exclusion were the presence of an exclusion criterion (22%), the patient’s refusal to participate (16%), the patient’s request for antibiotic treatment (14%), and lack of time by the family physician (10%). Third, we compared the findings on plain radiographs of the maxillary sinuses with the imaging results for other family practice populations with clinically suspected sinusitis and found good correspondence.
Study Population
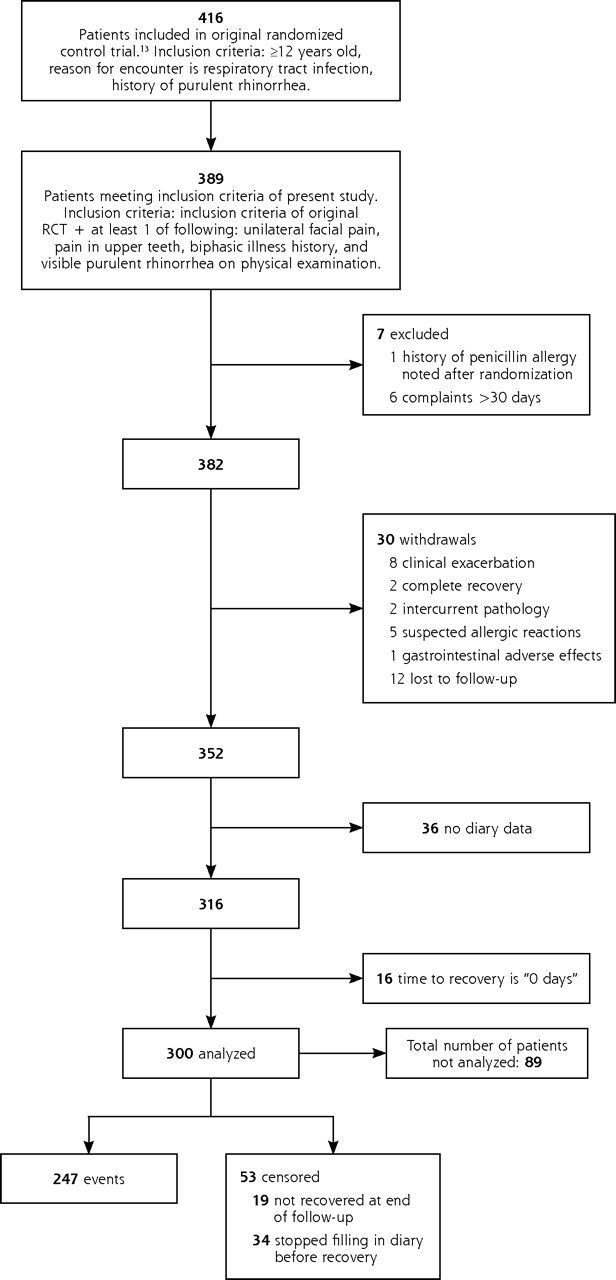
Of the 416 patients included in the original RCT, 389 met the inclusion criteria for this study. Of these, 89 patients could not be analyzed, for the following reasons: 7 were excluded after randomization; 30 withdrew before the end of the study; 36 did not have diary data on recovery time, and 16 felt “well” from the first day onward, so that their time to recovery was zero days. The reasons for exclusion or withdrawal are shown in the flow chart (Figure 1⇓).
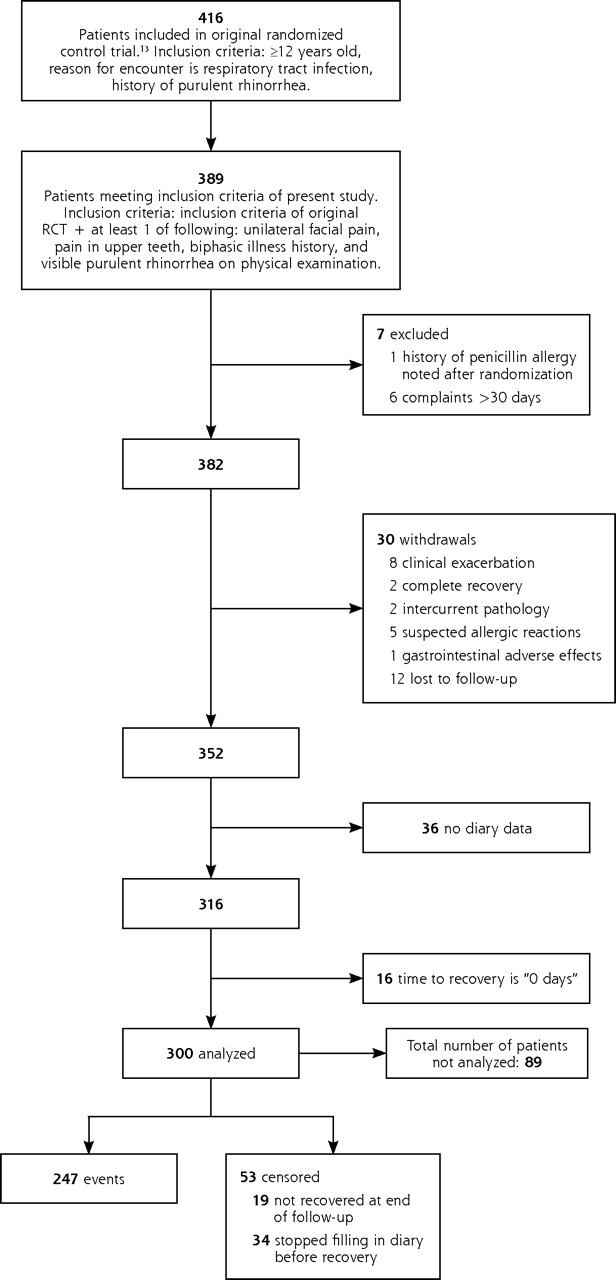
Flow chart of patients studied.
The demographic and clinical characteristics of the 89 patients not included in the analysis are compared with those of the 300 included patients in Table 1⇓. On average, patients analyzed in this study were more likely to feel ill and were more fatigued. This may have been due to the exclusion of patients who felt “well” at baseline; on the other hand, it may have been due to the fact that patients who recovered very quickly were less inclined to keep their diary, and follow-up for these patients is therefore lacking.
Comparison of the Patients Meeting Inclusion Criteria Who Were and Were Not Analyzed in the Study
Prognostic Variables
Of the 300 patients included in the present analysis, 247 recovered before the end of the observation period (247 events), while 19 had complaints for more than 15 days and 34 stopped keeping their diary before recovery (53 censored). Radiographic data were available for 218 of the 300 patients.
With regard to the prognosis, the crude hazard ratios show that 4 symptoms were significantly associated with a slower recovery: a higher clinical sum score, a general feeling of illness, facial pain, and reduced productivity (Table 2⇓). Two other factors—sex and fatigue—had P values less than .20 and were therefore also included in the multivariate analysis. Fatigue and reduced productivity were strongly correlated with each other (P <.001), and very few patients with reduced productivity were not fatigued; therefore, we did not include fatigue in the multivariate analysis.14
Prognostic Variables and Patient Recovery: Results of Cox Proportional Hazard Regression Analyses (N = 300)
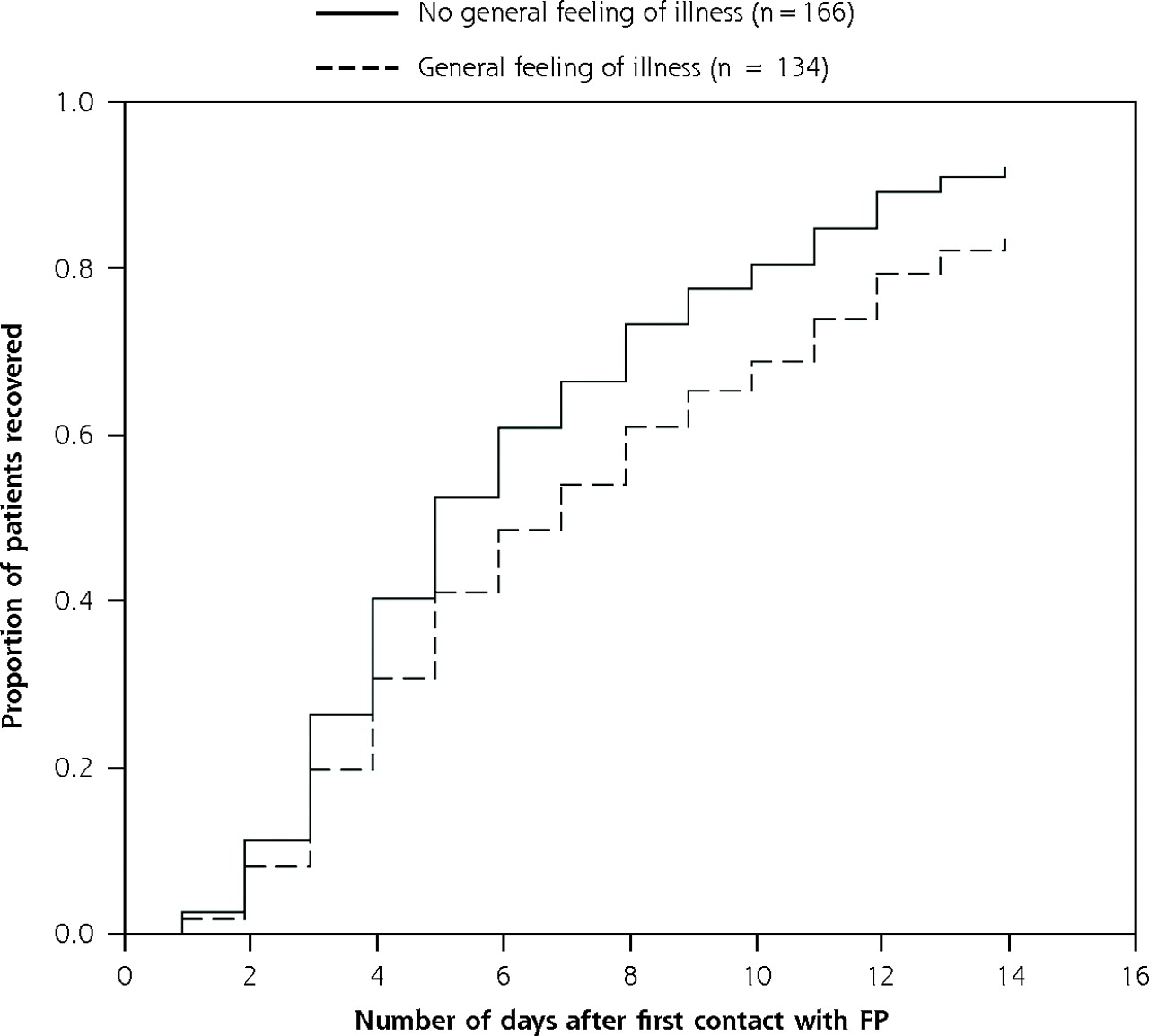
The 5 variables included in the multivariate analysis did not interact. Two symptoms independently predicted a slower recovery: a general feeling of illness and reduced productivity (Table 2⇑). The association for general feeling of illness is also depicted graphically in Figure 2⇓. In the group of patients without either of these symptoms, 50% had recovered after 5 days, and 75% had recovered after 8 days. In contrast, among the patients with a general feeling of illness, 50% had recovered after 7 days, and 75% had recovered after 12 days. Similarly, among patients with reduced productivity, the corresponding values were 6 days and 12 days.
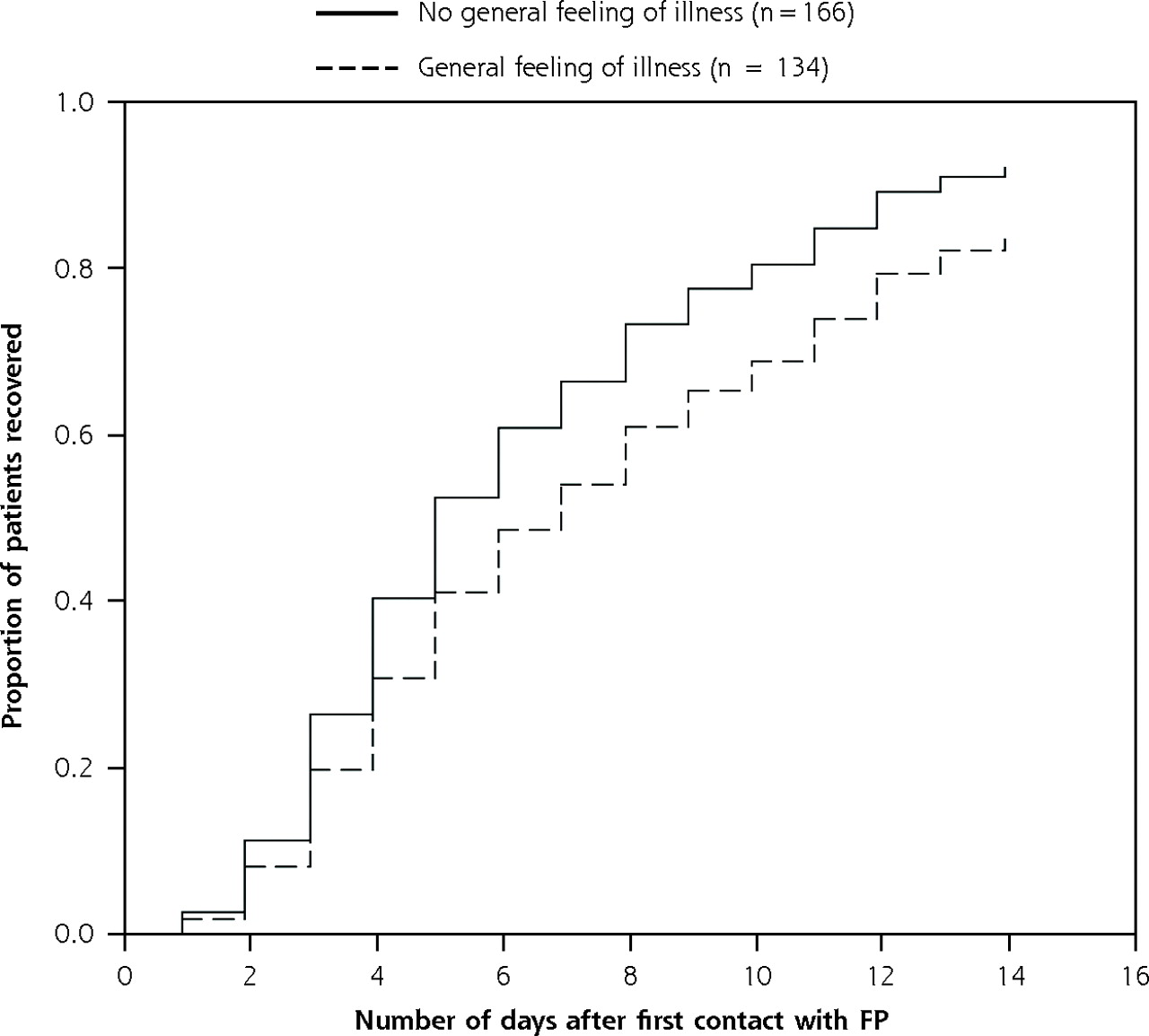
Recovery of patients according to their general feeling of illness at baseline adjusted for covariates.
FP = family physician.
Hazard ratio = 0.68 (95% confidence interval, 0.53–0.88); P = .003.
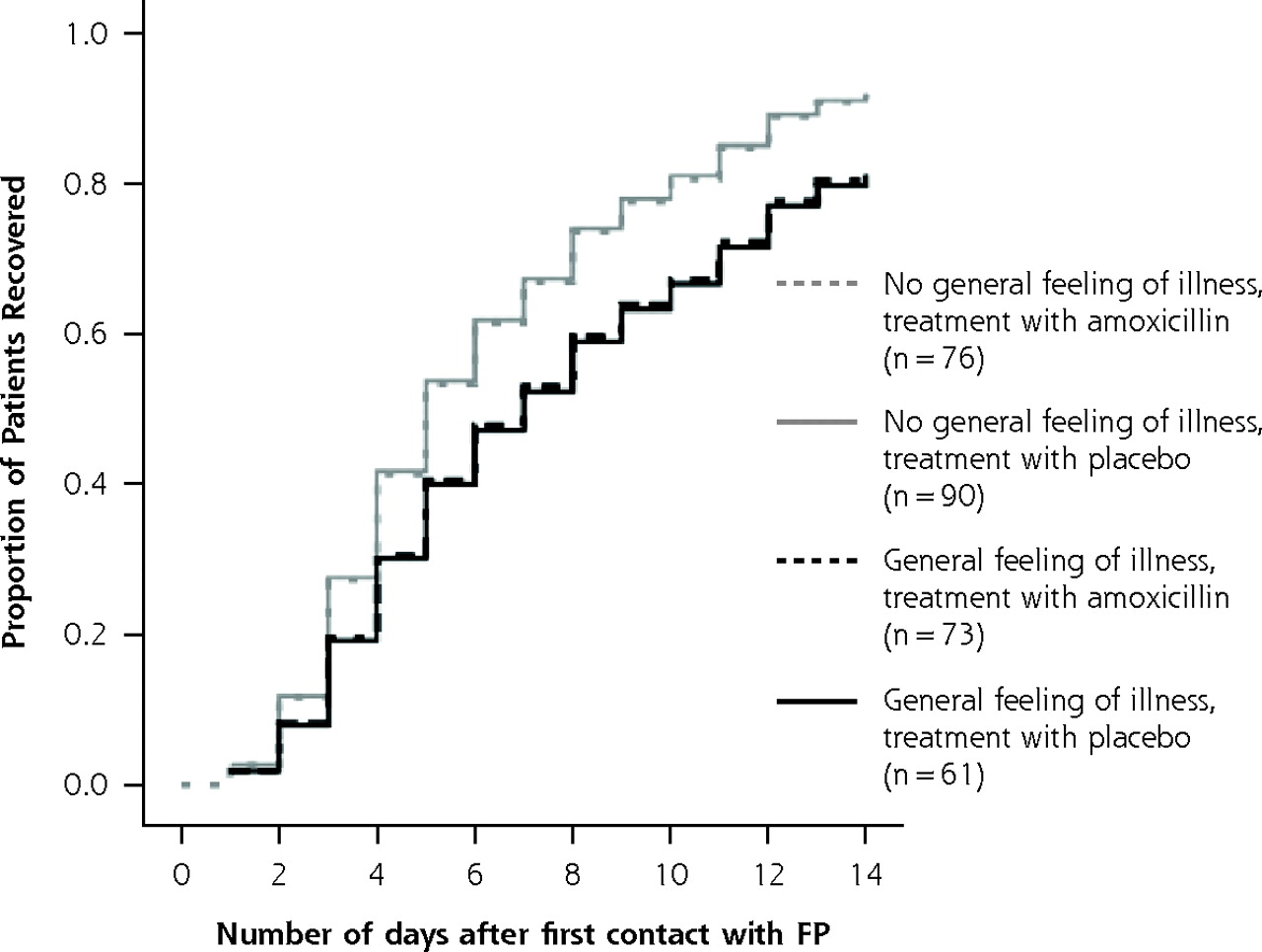
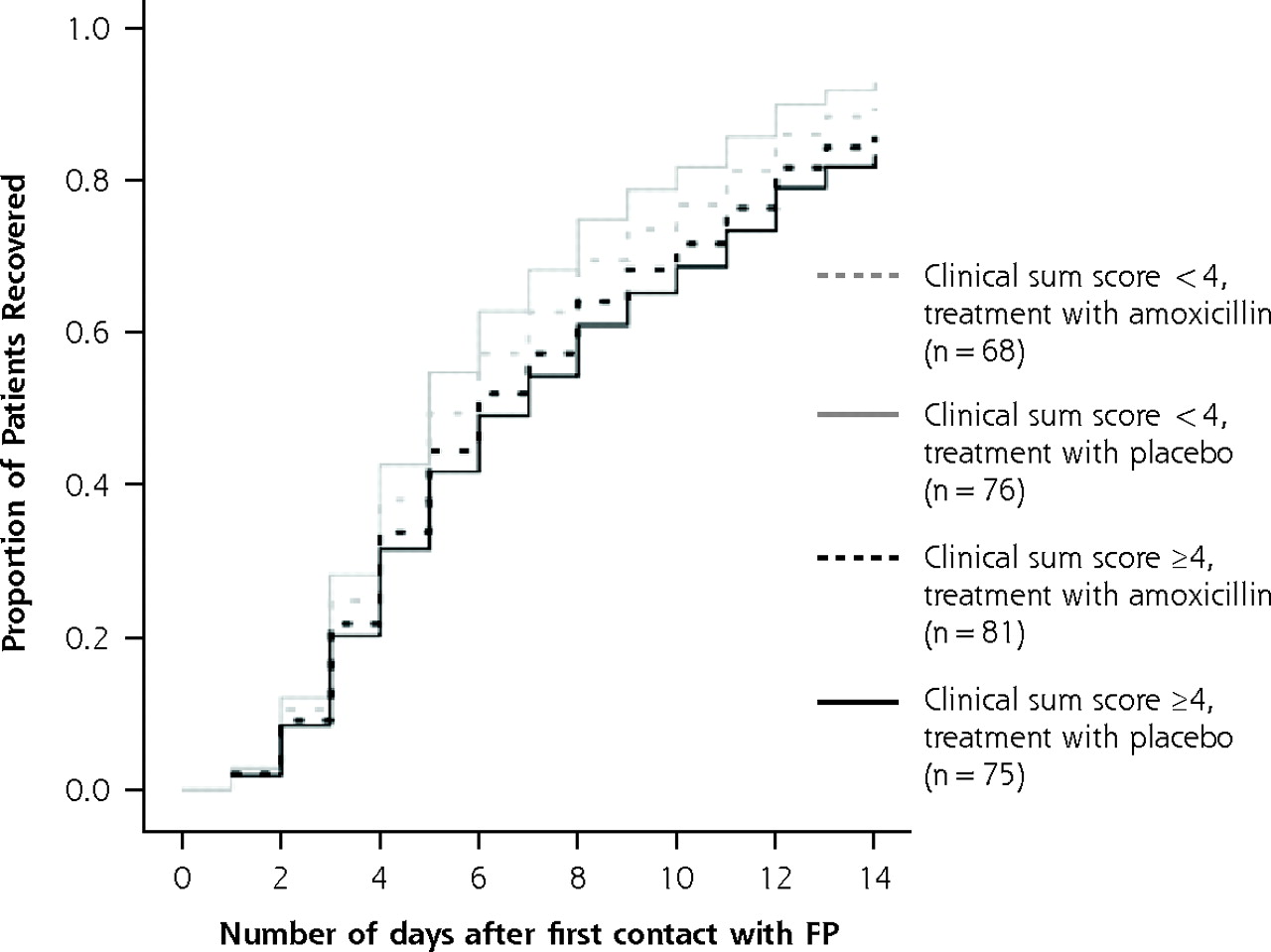
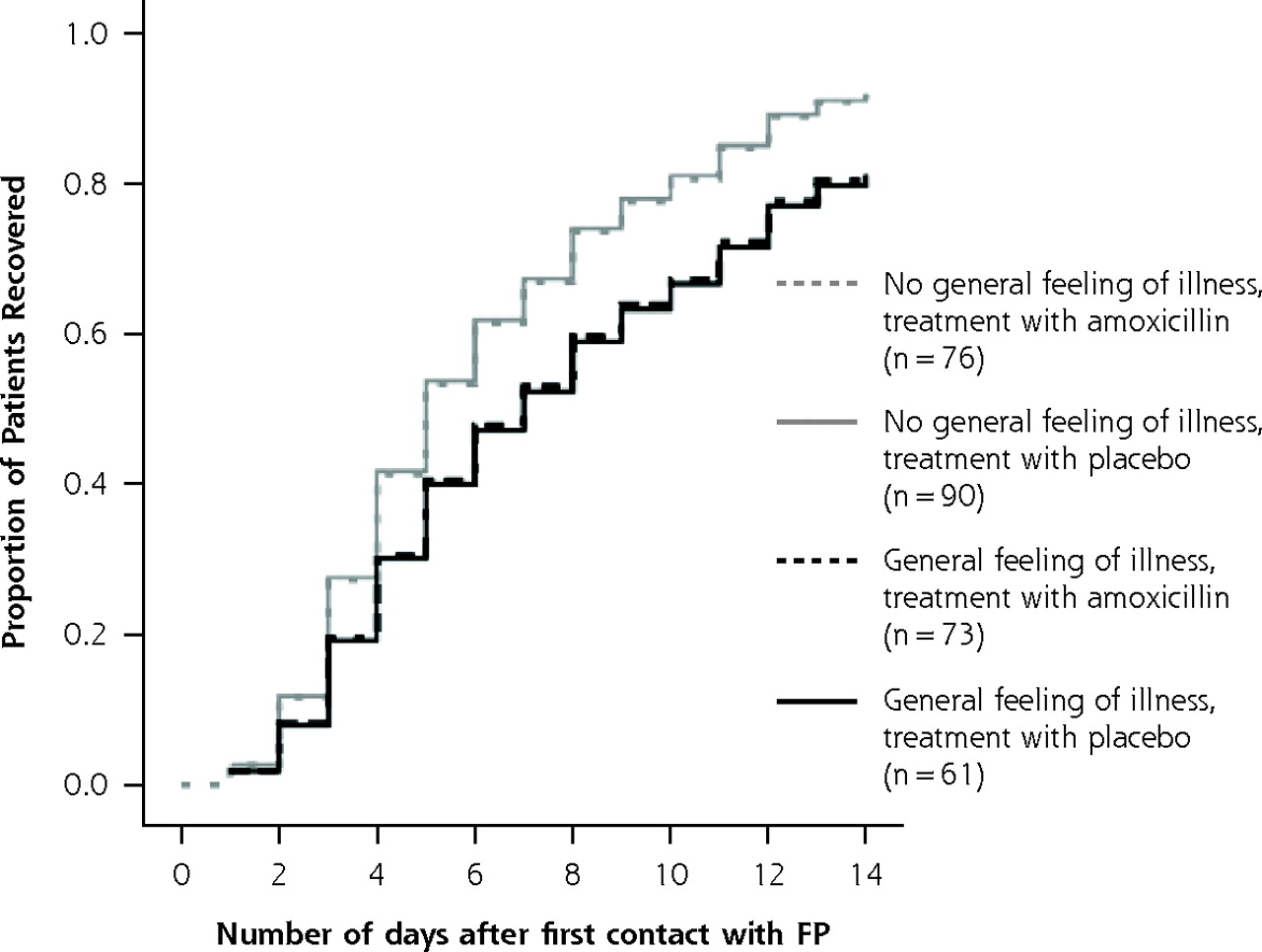
The analysis that tested for interactions showed that amoxicillin did not influence patients’ prognosis and that there was no significant interaction between any variable and treatment group (Table 3⇓). Figures 3⇓ and 4⇓ illustrate this finding for patients with a high clinical sum score and for patients with a general feeling of illness at baseline, respectively.
Results of Cox Regression Analysis for Interactions Between Prognostic Variables and Treatment Group*

Illness course in patients according to treatment and clinical sum score.
FP = family physician.
Note: For the sum score, 1 point was given for each of the following: purulent rhinorrhea, postnasal drip, temperature ≤37.5°C, complaints present for ≤7 days, biphasic illness history, pain on bending, unilateral facial pain, and pain in upper teeth. Possible range of scores: 0 to 8 points.
* Cox regression analysis for interaction between clinical sum score and treatment group (see also Table 3⇑). Model: clinical sum score (<4 /≤4) + treatment group (amoxicillin/placebo) + clinical sum score × treatment group. P value for interaction = .36.
Illness course in patients according to treatment and general feeling of illness.
FP = family physician.
* Cox regression analysis for interaction between general feeling and treatment group (see also Table 3⇑). Model: general feeling of illness (present vs absent) + treatment group (amoxicillin vs placebo) + general feeling of illness × treatment group. P value for interaction = .91.
DISCUSSION
Our main findings are that in patients with suspected acute rhinosinusitis, most signs and symptoms, and abnormalities on radiographs are not informative with respect to determining the subsequent course of the illness; furthermore, it is impossible to predict on the basis of signs, symptoms, and abnormal radiographs which patients will benefit from antibiotics. Two subjective indicators of a patient’s overall health—a general feeling of illness and reduced productivity—are associated with slower recovery, but antibiotic treatment does not speed recovery in these patients.
Study Strengths and Limitations
Our study methods have both strengths and limitations. The strengths of this study are the size and representativeness of the population: all patients were regular family practice patients consulting their family physician with signs or symptoms that have been associated with acute rhinosinusitis in well-performed diagnostic trials. The sample size was sufficiently large to detect relevant differences in recovery rate. The number of patients with signs of severe infection (high fever and bad pain) was limited, however. Although this is a reflection of the reality of family practice, wherein serious acute illnesses are infrequent,15 we cannot exclude the possibility that antibiotics may influence the prognosis in such patients. Most prognostic variables studied were related to the current episode of illness, and it is possible that other contextual or personal circumstances, such as previous medical history, coping skills, and social support, may also influence recovery speed. A previous study on the prognosis of rhinosinusitis found, however, that emotional distress did not influence the course of this illness.11
Rationale for Study Design
We chose amoxicillin instead of the broader-spectrum amoxicillin-clavulanate because amoxicillin is the recommended first-line drug for rhinosinusitis in several practice guidelines,16–18 and in our geographic area, respiratory pathogens were sufficiently sensitive to this antibiotic during the trial.13 It is possible that resistance patterns of respiratory pathogens have changed since then, but this does not alter our conclusion that an active antibiotic was not significantly more effective than a placebo.
We selected the prognostic variables studied based on their clinical relevance and usefulness in routine family practice consultation. The exception was radiography, which was included because so far, very little is known about its prognostic value.
To detect an effect of amoxicillin in patients with different clinical characteristics, we used statistical tests for interactions. These tests are much more valid for investigating whether a treatment effect differs among complementary subgroups than are separate tests for significance within subgroups.19
Search for Prognostic Variables
Two previous studies10,11 have looked for factors influencing the prognosis of acute rhinosinusitis. Stalman et al11 found that in patients who had clinically suspected acute rhinosinusitis, female sex, a duration of symptoms for more than 14 days before medical contact, and the absence of cervical adenopathy independently influenced the duration of pain. Lindbaek and Hjortdahl10 found that in patients with suspected acute sinusitis and a sinus CT image showing an airfluid level or complete opacity, a higher clinical severity score and older age predicted slower recovery. Results of these 2 studies differ from each other, as well as from our results. Possible explanations are disparities in the populations studied or the outcomes measured. Our study population was considerably larger than the populations in these studies, however, making our results more reliable. Yet, when several studies investigating the same question find conflicting results, it also might indicate that a clear-cut prognostic sign or symptom simply does not exist.
A study by Young et al12 attempted to identify subgroups of patients with clinically suspected acute rhinosinusitis who might benefit from antibiotics. The subgroup of patients with visible purulent rhinorrhea or postnasal drip had a somewhat faster recovery after 7 days if given antibiotics, but after 14 days, the difference was no longer significant. We could not confirm these results in the present study. This difference might be related to the fact that in the earlier study, outcome data were available for only 3 time points (days 7, 14, and 28), whereas in our analysis, we had day-to-day data that gave a better picture of the actual course of the illness. With respect to radiographic findings, our results are in accordance with those of Young et al,12 as we also found that patients with an abnormal radiograph of the sinuses did not benefit from antibiotics.
The results of some RCTs2–5 suggest that there is a limited group of patients in whom antibiotics can be beneficial. The aim of our study was to identify this group of patients from clinical or radiographic features; however, we did not succeed. Our inability to identify these patients could mean that this group is actually very small and our study, despite its size, lacked sufficient power to identify this group. Yet, as the graphical illustrations show (Figures 3⇑ and 4⇑), the differences are so small that even if they were statistically significant, they would not be clinically relevant. Another explanation may be that it is not possible to identify patients who will benefit from antibiotics by using the variables we studied.
Our results can nonetheless be useful in daily practice in another way. Patients are entitled to—and greatly appreciate—correct information on the prognosis of their illness for reassurance, as well as for making realistic plans for their immediate future.20 Physicians often tend to be too optimistic in predicting the duration of disease,21 which can cause unnecessary anxiety, early reconsultations, and inappropriate antibiotic prescribing. In this context, our study contributes to a better understanding of the natural course of acute rhinosinusitis.
Patients with clinically suspected acute rhinosinusitis are a large and familiar group in family practice. Yet, their clinical pictures can be quite divergent, and deciding on a treatment is often an uncertain process of weighing different clinical signs and symptoms, and guessing which patients might have bacterial rhinosinusitis and thus need antibiotics. We tried to approach this problem from a pragmatic point of view by focusing on the clinical and radiographic picture instead of on the presumed diagnosis. We found that in a representative group of patients with rhinosinusitis, neither individual signs or symptoms of sinusitis, or their sum, nor radiographic information were useful for predicting an unfavorable prognosis or the effect of amoxicillin. It is clear that acute rhinosinusitis is a self-limiting disease, and our results allow us to formulate clear-cut recommendations for practice. The best policy for patients with suspected rhinosinusitis—but without signs of complications or severe infection (high fever and bad pain)—is to wait for spontaneous recovery. If necessary, bothersome symptoms, such as pain or nasal obstruction, can be suppressed with treatment aimed at the symptoms. Our study did not find evidence that any signs or symptoms warrant antibiotic treatment or that radiography has added value in this setting.
Footnotes
Conflicts of interest: This study was partly funded by Eurogenerics NV, Belgium, a pharmaceutical company distributing generic medication. None of the researchers or authors was linked in any way to this company. The design of the study, data analysis, and reporting happened completely independent of Eurogenerics.
Funding support: This study was funded by a grant by Eurogenerics, NV, Brussels, Belgium, and by the Department of General Practice and Primary Health Care, Ghent University, Ghent, Belgium.
- Received for publication November 28, 2005.
- Revision received March 13, 2006.
- Accepted for publication March 31, 2006.
- © 2006 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The role of antibiotics in the treatment of acute rhinosinusitis in children: a systematic review
- Acute sinusitis
- Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial
- On TRACK: The Search for the Holy Grail
- Annals Journal Club: Antibiotics for Common Respiratory Infections
- A New Look at an Old Problem: Inappropriate Antibiotics for Acute Respiratory Infections
- In This Issue: Prescribing Drugs: What Do Patients and Pharmaceutical Companies Really Want?