
Abstract
Despite the increasing prevalence of chronic conditions and multimorbidities, the essential attributes of the structure and delivery of primary care continue to be defined in terms of disease-specific approaches and acute conditions. Effective improvements will require alternative ways of thinking about chronic care design and practice. This essay argues for an ecosystemic understanding of chronic care founded on a communal and a dynamic view of the response of the patient, family, and health professionals to chronic illness. The communal view highlights the cocreative nature of the response to illness and the need to integrate the skills and resources of all the participants; what and how the participants learn in the course of the illness become central to chronic care. The dynamic view draws attention to the unfolding of illness management activities over time and to the need to engage the illness at specific time points or recurring time intervals that have the potential for important change in the experience of the participants. Chronic care would then include design for community, with an emphasis on the patient and family as necessary participants in the health care team. It would also include design for emergent learning and practice whereby health professionals go beyond standardization of care processes to develop new ways to harness the participants’ imagination and learn from the changing experience of illness. Health professionals would also learn to cultivate trust, communal engagement, and openness to experimentation that facilitate collective learning, and help sharpen the participants’ responsiveness to the emergent.
- Chronic illness
- health professionals
- ecosystem
- family
- learning community
- complexity
- health care delivery/health services research
- psychosocial factors
- systems theory
- models, theoretical
INTRODUCTION
The increasing prevalence of chronic conditions and multimorbidities has stimulated numerous efforts to improve chronic care.1–5 The essential attributes of the structure and delivery of primary care continue to be defined in terms of acute conditions and disease-specific approaches, however.6 Encounters for chronic care are still treated as if they were unique events rather than a continual process of care.4,7
The aim of this essay is to suggest an alternative way of thinking about the structure and delivery of chronic care. Its central claim can be summarized as follows: chronic care is what the patient, family members, and health professionals do to achieve specific health outcomes within the evolving opportunities and constraints of chronic illness. Chronic care in this view is an ecosystemic response to illness: a collective and more or less adaptive response of the patient, family, and health professionals to the changing biological and psychosocial manifestations of the illness. In the following sections, I unpack this claim by first reviewing the main features of chronic care activities. Next, I propose 2 perspectives that can help integrate these features into chronic care design and practice. Finally, I discuss implications for chronic care design and present recommendations for clinical practice.
THE NATURE OF CHRONIC CARE ACTIVITIES
Chronic care activities have 2 main characteristics. First, they entail a conceptual shift from disease management to illness management. Disease management refers to clinicians’ understandings of the biomedical model of disease progression.8 In contrast, illness management refers to how patients, families, and other members of the social community perceive, explain, and cope with the illness.9,10 The confluence of these 2 perspectives encompasses the lived experience of illness, its associated cultural and social categories (spiritual, ethnic, folk, and family beliefs), and their interactions with the psychobiological processes of chronic pathology.10 Shared understandings among health professionals, patients, and families about the meaning of illness, suffering, recovery, and death become central to chronic care.11
Second, unlike acute illnesses, chronic illnesses bring a dynamic complexity inherent in their lengthy and multifactorial nature. Caused by irreversible pathologic alterations, chronic illnesses often leave residual disability and require intermittent periods of care and complex treatment.12–16 Changing patterns of illness are created from the interaction of the disease, its consequences, and the social context—all dynamic in nature, and requiring continual monitoring and complex management.
Together, these characteristics help specify 2 features of chronic care activities: (1) they occur at the confluence of processes that are rooted in the biological, psychosocial, and cultural realms of human experience; as such, they raise issues of shared meanings and mutual dependencies among the participants; and (2) they weave together the developmental threads of chronic illness, of patient and family, and of the health care team.17 Chronic care appears as a collective enterprise, mobile, changing, and riddled with renewed instabilities that reflect variable qualitative and quantitative differences in how diseases are manifested over time and in how patients, family members, and health professionals respond to them. How then can we integrate these features into our conception of chronic care design and practice?
INTEGRATING CHRONIC CARE DESIGN AND PRACTICE
Two perspectives are necessary. Both draw on approaches in human ecology.18 The first, a communal view, recognizes the interdependent nature of illness management activities. The second, a dynamic view, recognizes the mobile and shifting qualities of illness experiences.
The Communal View of Chronic Care
In an ecosystemic approach, chronic care is a communal engagement of its participants in a set of recurring activities that are part of the same human enterprise: preserving life, establishing viable relationships with the environment, surviving together.18 Chronic care in this view is a communal adaptive system, an association of specific individuals who through an organization of their resources, differentiated activities, and skills, act as a unit to preserve, improve, and expand life to the maximum attainable under the prevailing opportunities and constraints of their environments (physical, biological, homes, workplaces, hospitals, clinics).18–21
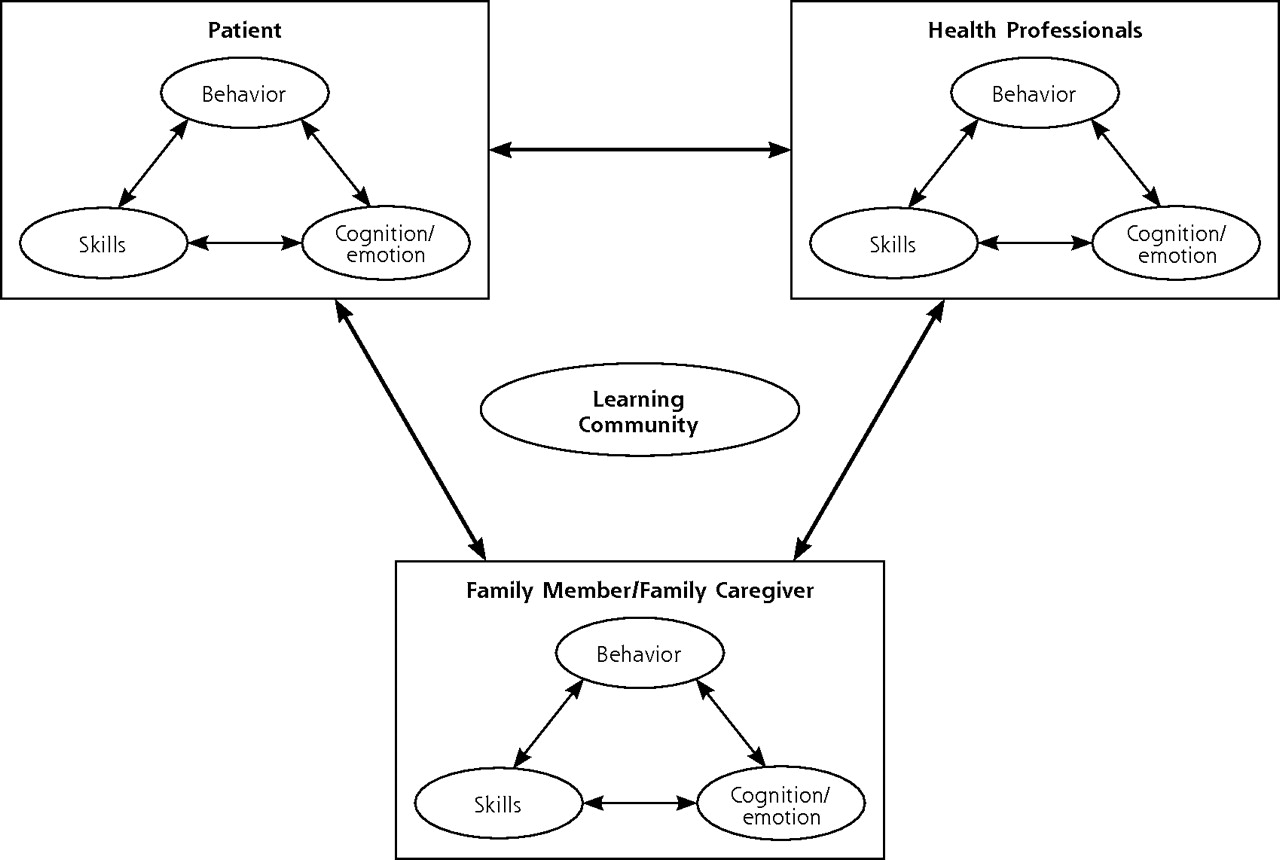
In this ecosystem, several linkages are created among the participants’ activities and between specific niches they occupy.18 As Figure 1⇓ indicates, encounters between the patient, family members, and health professionals bring together multiple cognitive and emotional representations of the illness, multiple behavioral modalities, and multiple skills that underlie behavior performance.22,23 Health professionals provide knowledge and expertise in health care. Patients provide self-care skills and the physiologic energy to accomplish self-care activities.8,24 Family members also invest time, energy, emotions, money, and other resources into coping with the illness.25,26 Chronic care appears as a more or less effective arrangement of mutual dependencies and collaborative efforts, a network of communication and relationship ties among patients, family members, and health professionals, designed to achieve common health goals.18,21,27

Interactions of the patient, family members, and health professionals: the encounter of multiple competencies.
An important corollary of the communal view is that the encounters of the patient, family, and health professionals are also those of a learning community—a group of individuals who through language and conversations negotiate meanings and learn about the illness, about each other, and about themselves.28,29 Indeed, the participants in chronic care activities are purposeful human beings whose behavior is shaped by the ideas, meanings, and interpretations that they have of themselves and their environments.30,31 Because chronic illness changes how patients and families perceive themselves and what they can do, they also develop new meanings and new ways of responding to their environments, including their encounters with health professionals.28,32 In turn, health professionals learn from the patient and family, and from the collective work and knowledge that are triggered and nurtured by the clinical encounters. Insights from complexity theory reinforce this view as they indicate that learning can emerge from the interactions and enacted differences among adaptive agents.33–37 In their conversations, for example, health professionals, patients, and family members may have differences in opinion, beliefs, behaviors, knowledge, and ways of thinking. As a result of these differences, learning—in the form of shifts of understanding and novel patterns of thoughts, emotions, and behaviors (eg, conflicts, rules, prescribing behaviors)—can emerge and spread through subsequent conversations and interactions among the participants.33,37
A communal view therefore highlights the need to integrate the identities, skills, and resources of all the participants.28,29 It also underlines the cocreative nature of the response to chronic illness.18,34–37 What and how the participants learn in the course of the illness become central to chronic care.28,29,36
The Dynamic View of Chronic Care
In the dynamic view, we recognize the episodic and changing nature of the interdependencies among the participants. Chronic care requires ongoing adjustments marked by some phases when the patient is self-reliant and other phases when he or she is dependent on health professionals.38 These phases reflect the mobile nature of the locus of control over change.39 Managing this shifting reality requires flexible designs that can match the variable patterns of illness and their associated demands and resources.
In the dynamic view, we also recognize the patterned influence of time on chronic care activities. Time in chronic care shifts away from single events to recurring episodes, and from a linear view of past, present, and future to a variable integration of specific recurring activities and durations at the level of the patient, family, and health professionals. In other words, chronic care time has rhythm, and temporal rhythms must be included in the context of illness management. For health professionals, many standing patterns of behavior—blood sampling, radiographic screening, physician-patient meeting—have more or less predictable delays and occur only at certain times of the day, week, or month.26,40,41 For the patient and family, chronic care activities are also intermittent—their temporal spacing being regulated by the recurring needs for food, rest, and other daily needs—and only a subset of these activities involves the interaction of the patient with health professionals.18,32,42 Considering time also introduces a historical dimension through which these activities are understood in terms of the patient’s and family’s unique history with illness, developmental issues, expectations, resources, and vulnerabilities at different life stages.32
A dynamic view of chronic care therefore draws attention to the unfolding of illness management activities over time and to the need to engage the illness at specific time points or recurring time intervals along its lines of deployment—specific time phases that have the potential for important qualitative or quantitative change in the experience of the participants.17,32
Characteristics of the Ecosystemic Approach
In summary, an ecosystemic approach to chronic care highlights 3 units of analysis: the group of participants in care activities, their environments (biological, psychosocial, health care organization, family unit), and their adaptive response to chronic illness. What takes primacy in this triad is the adaptive component: the evolving arrangements of mutual dependencies and linkages among the participants and their environments. Effective arrangements of these linkages allow the participants to act as a unit, with shared goals, shared meaning and learning, mutual awareness and understanding of the contributions of each participant (representations, emotions, skills, behaviors), and well-timed communications. Three characteristics of this adaptive ecosystem are essential to chronic care design and practice: it is spread across and beyond the health care organization to include the patient and family as necessary participants; it has rhythm; and it is fluid—its specific structure and function emerging from the demands of the illness, the available resources to meet them, and the evolving encounters of the participants.
IMPLICATIONS FOR CHRONIC CARE DESIGN
Based on the preceding discussion, chronic care design must support community development, emergent learning, and the coordination of efforts within identifiable constraints, resources, and rhythms.
Designing for Community
There is much to know about the requirements of a design that recognizes the patient and family as necessary participants in the care team.26 The challenges of designing for community go beyond giving the patient and family a voice in decisions.26,43–45 They are those of negotiating meanings not just in conflicting multicultural encounters, but also in the clashing of the narrative logic of the experience of illness and the deductive logic of medicine.11,28,46,47 They are also those of dispersed communities (eg, health care organization, family unit), time, and fluctuating demands of the illness with varying dependence on health professionals.38,39 The challenges also reside in how to organize the relationships among the participants: how to recognize, coordinate, value, and leverage their engagement to the health care organization.48 An example of a useful area of investigation is the architectural and technological design of the spaces wherein the encounters among patient, family, and health professionals occur.28,48,49
Designing for Emergent Learning and Practice
Chronic care activities evolve over time with potentially changing goals.26,42 Central to this adaptive system is the ability to detect changes through continual monitoring, and to use those changes as feedback that activates relevant strategies—changing roles for the patient, family members, or health professionals, developing or introducing new skills into the group.26 Learning in chronic care is then better conceived in terms of the emergent events and collaborative tasks that structure chronic care.4
The emergent nature of chronic care activities challenges the planned didactic strategies that follow evidence-based guidelines. Designing for emergent learning and practice is more about the definition of goals, constraints, and coordination of resources than the detailed formulation of fixed competences and places for learning or practice. Examples of constraints/resources include patients’ access to resources that support self-management or the physiologic factors that impinge on their energy to manage the illness. Other examples include the available technology, the relevant mix of professionals, the locations for collaborative practice (health care organization, family unit, or both), and the schedules, roles, potential partners, and financial arrangements within the practice and the family unit.39
Designing for emergent learning and practice would then leave ample space for imagination, improvisation, and creative adjustment to the more or less predictable experiences of illness. To be anchored in the communal engagement of practice, imagination and improvisation would rely not only on dry runs and simulations, periodic review sessions, and keeping up with new technologies and research literature, but also on the development of an organizational culture that favors a sense of community, trust, and openness to experimentation and discovery.17,28,32,50,51 Ongoing experiences with process change methods such as the Plan, Do, Study, Act (PDSA) cycles suggest that the “try it and see” attitude, combined with group processes and leverage on the health care organization through its senior leaders, is an essential element of successful collaboratives.52 Models of communities of practice are also promising for the chronic care context for their potential to integrate learning and practice.48,53 Communities of practice can provide an effective social context for reflection on collective experience during and outside of the clinical encounters, and can help develop and refine the knowledge used in practice iteratively.28,50,54
RECOMMENDATIONS FOR CLINICAL PRACTICE
The following recommendations can serve as a guide for designing for community and emergent learning and practice.
-
Develop your “village square” by assembling team members around clinical tasks and social situations. Create lively gathering places where the participants can get to know each other and develop a sense of belonging to a larger community. The village square can take different forms—Web-based forums, lively water cooler areas, workshops, and group meetings for patients to discuss their self-management strategies. The goal here is to deepen the connections with patients, their families, and team members as a group of people who have agency, a specific history with illness, and who live a particular life.39,55
-
Elicit and foster participation. Make trust and compassion strategic requirements of chronic care, encourage self-reporting of mistakes, and target your interventions to relationships, not solely to individual patients or team members. For example, for diabetic patients to change their diet, their connection to their family members in relation to food selection, preparation, and eating schedule may also need to change; for team members to improve their collective performance, they must understand how they depend on each other.48,56,57
-
Make the patient’s and family members’ perceptions and emotions an essential thrust of clinical efforts.58 Sincere emotional connections are the basis for trust, empathy, and insightful compassion that can help anticipate the confusion and the potential for learning that patients and families bring to the clinical encounters at different stages of the illness.56 What questions will they be asking? What skills will they require? How much do we need to know about them, and how much do they need to know about the professional team? How will their thinking or emotions mesh or clash with professionals’ thinking and emotions?
-
Ask not only what you can do for your patients, but also what the patients and families can do for themselves and for your clinical practice. Make cocreation of care plans a strategic requirement of chronic care; patients and families are primary care’s best learning asset as they trigger specific domains of knowledge that become focal points for connecting and organizing the resources of all involved.28
-
Link the business value (caring for patients) to the knowledge value48 and knit a varied quilt. Identify key activities depending on the illness, analyze them in terms of critical knowledge domains, and identify who among the participants needs this knowledge.48 Connect people with different expertise, and leverage the accumulation of experience by making visible both their explicit and tacit knowledge: organize their work around common tasks, record their conversations, collect and communicate their failure and success stories.37
-
Learn more about narrative medicine. Know how to listen to stories and how to tell them.37,46
-
Anticipate accumulation and decline on different accounts. Schedule visits around specific phases of the illness timeline to assess skills, self-regulation, coping behaviors, and resources; schedule assessments for all the participants, not just for the patient and family.17,36
-
Think in terms of incremental change. Think of small experiments to test and implement change and learn from variation.59 Plan also for repeated measures of implementation and outcome; data accumulated over time can reveal the appropriate timing of interventions.50,60
-
Problem-solve, yet be flexible and goal oriented.21 Who is responsible for change? Is the relevant information at the level of the patient, family, health professionals, or the larger social community?39 Comprehensive chronic care goals are then defined as target values at different levels of the ecosystem of illness management including the biological, psychological, familial, and social realms.42,61,62
-
Make a habit of reflection time. Reflection can be organized around broad phases of the illness timeline, such as a 4-stages axis including prediagnosis, diagnosis/treatment, recovery/disability, and death.32 Each of the phases represents a turning point to important change in the illness, its demands, and the resources to meet them. Reflection can also be done before, during, and after the visit, and can, for example, facilitate the production of visit summaries for patients.63
-
Keep a record of your learning process.53
-
Think longitudinally, but remember the circular nature of time. Temporal rhythms provide the beat that influences the pace of what patients do to manage their illness, with whom, when, and where they are able to do it. Create an effective rhythm by adjusting the frequencies of communications among the participants to facilitate collaborative practices, coordinated engagements in care activities, and the development of a sense of community.39,48
-
Challenge assumptions once in a while. Keep asking, why do we do this in this way?64
CONCLUSION
Design for acute care, with its standardization of process, may be likened to that of an ice cube formed in the mold of a cubic slot where water is frozen into a pregiven form. In contrast, design for chronic care is better compared with that of a snowflake that forms itself in a streaming space by tapping into the useful flows of gravity, wind, humidity, dusts, and chemical gradients. As much as each snowflake differs from any other, each patient lives a unique illness experience that generates a unique set of interactions with health professionals. For patients, the streaming space that shapes chronic care includes not only their peculiar list of physiologic constraints tied to specific diseases and comorbidities, but also their need for food and rest, individual preferences, available resources, and uncertain everyday decisions.8 For health professionals, chronic care is shaped not only by their expertise, but also by their intuition and creativity to expand their competence by integrating the patient’s comorbidities, family and work problems, conflicting schedules, economic resources, and constraints.65
The shifts required to implement this understanding represent a cultural change. From an ethos of standardization and prefabricated structures, the move is to a streaming and tracking ethos in which health professionals develop new ways to recognize, value, and manage the communal response to illness; new ways to document and learn from the changing nature of illness experiences; and new ways to cultivate openness, trust, and communal engagement that facilitate collective learning and help sharpen the participants’ responsiveness to the emergent—all essential skills for those who want to foster and enjoy their relationship with each patient.28,48,50,65
Acknowledgments
I am grateful to William Miller for his helpful comments on an earlier version of this manuscript and to Robert Thivierge for directing me to some of the best readings about knowledge management and learning in clinical practice. Special thanks go to Paule Lebel for many stimulating conversations on the topic of medical education. I am also thankful to Martin Fortin, Sharon Hatcher, and Catherine Hudon for their supportive comments.
Footnotes
-
Conflict of interest: none reported
-
Funding support: This work has benefited from support from the Department of Family Medicine at the University of Sherbrooke, the Fondation Relève Médecine 2000, the Department of Family Medicine at the University of Montreal, and the Groupe de Recherche Interdisciplinaire en Santé.
- Received for publication February 22, 2006.
- Revision received October 17, 2006.
- Accepted for publication October 30, 2006.
- © 2007 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- Learning and Caring in Communities of Practice: Using Relationships and Collective Learning to Improve Primary Care for Patients with Multimorbidity
- 'You Complete Me'
- Is 'Clinical Inertia' Blaming Without Understanding? Are Competing Demands Excuses?
- In This Issue: New Concepts for Diabetes and Chronic Disease Management