
Abstract
PURPOSE Patients seeking care for medically unexplained physical symptoms pose a major challenge at primary care sites, and there are very few well-accepted and properly evaluated interventions to manage such patients.
METHODS We tested the effectiveness of a cognitive behavior therapy (CBT)-type intervention delivered in primary care for patients with medically unexplained physical symptoms. Patients were randomly assigned to receive either the intervention plus a consultation letter or usual clinical care plus a consultation letter. Physical and psychiatric symptoms were assessed at baseline, at the end of treatment, and at a 6-month follow-up. All treatments and assessments took place at the same primary care clinic where patients sought care.
RESULTS A significantly greater proportion of patients in the intervention group had physical symptoms rated by clinicians as “very much improved” or “much improved” compared with those in the usual care group (60% vs 25.8%; odds ratio = 4.1; 95% confidence interval, 1.9–8.8; P<.001). The intervention’s effect on unexplained physical symptoms was greatest at treatment completion, led to relief of symptoms in more than one-half of the patients, and persisted months after the intervention, although its effectiveness gradually diminished. The intervention also led to significant improvements in patient-reported levels of physical symptoms, patient-rated severity of physical symptoms, and clinician-rated depression, but these effects were no longer noticeable at follow-up.
CONCLUSIONS This time-limited, CBT-type intervention significantly ameliorated unexplained physical complaints of patients seen in primary care and offers an alternative for managing these common and problematic complaints in primary care settings.
- Mental health
- somatization disorder
- chronic pain
- pain management
- health care delivery/health services research
- primary care
- disadvantaged
- access to health care
- Hispanics
- Latinos
- psychotherapy, brief
INTRODUCTION
Patients seeking care for medically unexplained physical symptoms (those physical symptoms that remain unexplained after proper physical and laboratory evaluations) are a frequent and problematic occurrence in primary care, and these symptoms may augur mental health problems.1–7 It is difficult to approach these patients from a mental health perspective because only some of them acknowledge psychological issues as contributing factors, and many reject psychological explanations.8 Stigma and limited resources may play a role, particularly in the case of disadvantaged, minority populations. Despite an increased awareness of somatization syndromes and depression and the availability of effective interventions that can be administered in primary care,9–12 appropriate treatments are rarely implemented, possibly because patients are not properly recognized because of their somatic presentations or do not accept psychiatric treatment or referral.
Despite the frequency of somatization syndromes, there was no effective management for them until recently. Two decades ago, investigators studied the effects of a consultation letter on outcomes of patients with multiple severe, unexplained physical symptoms (somatization disorder).13 This simple intervention provided a brief list of “dos” and “don’ts” to primary care physicians dealing with such patients and led to a modest functional improvement and decreased health expenditures. For many years, this intervention was the only one with empirical evidence supporting its efficacy in treating these patients. Recently, however, results of 2 new studies have shown substantial promise in managing patients who are high users of health care and have high levels of unexplained physical symptoms.14,15 Smith et al14 reported on an intervention that led to more effective recognition and treatment of these patients in primary care. Allen et al15 performed a controlled study of a time-limited cognitive behavior therapy (CBT)-type intervention on somatization disorder as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) in a mental health clinic. This intervention yielded significant effects beyond those associated with a traditional consultation letter, ameliorating medically unexplained physical symptoms, improving functional status, and decreasing health care costs in a chronically ill population.15
The present study builds on the work of Allen et al15 by testing the effectiveness of the same intervention when administered in primary care clinics, this time targeting a broader, ethnically diverse population with less severe somatic presentations.
METHODS
Clinical Settings
The study was conducted after approval from the University of Medicine and Dentistry of New Jersey’s institutional review board. The study settings were 2 university-based primary care clinics located in New Brunswick, NJ. The first (Chandler Clinic) is a federally qualified health center that is under the aegis of the dean for community programs in the medical school and staffed by the Division of General Internal Medicine of the Robert Wood Johnson Medical School. The clinic offers comprehensive services to an underserved, ethnically diverse, low-income urban population, more than 50% of whom are uninsured. The second (Monument Square) is an outpatient clinic operated by the Department of Family Medicine of the medical school and serves primarily a white, middle-class, urban population in the city. Each of these 2 sites had at least 1 primary care physician who was also a coinvestigator in the study and was very familiar with the project. Altogether, at the 2 clinics and for the duration of the study, about 8 physicians (residents and attending physicians) performed the initial evaluations and referred patients to our research team, either directly or through social workers and nurses working at the clinic.
Primary Care Patients, Physicians, and Research Personnel
Physicians or nurses at the primary care clinics referred consecutive patients 18 years and older to the research team at the clinics if they believed the patient had repeatedly sought care for medically unexplained symptoms and they thought the symptoms were a source of distress or suspected that they had a psychiatric origin. Patients who consented to participate in the study were interviewed face-to-face by research staff that included 4 doctoral-level psychologists and 4 psychology doctoral candidates, 6 of whom were bilingually fluent and conducted interviews and therapy sessions in Spanish as needed.
On referral, the research staff assessed potential participants either in person or by telephone with a brief screening measure, the Patient Health Questionnaire (PHQ)15 screener from the Primary Care Evaluation of Mental Disorders (PRIME-MD),16,17 to determine whether they met criteria for the study. To ensure selection of patients with sufficiently high levels of unexplained physical symptoms, we used a symptom threshold of 4 or more unexplained symptoms for men and 6 or more for women (ie, abridged somatization as described by Escobar et al2). Patients were not included if they had severe psychiatric disorders (suicidal ideation or psychotic symptoms) requiring more intensive intervention or if they had a major physical disorder that appeared to explain any of the symptoms.
Intervention
The principal goal of the study was to assess the effectiveness in primary care of a time-limited (10- session), standardized, CBT-type intervention expressly designed for patients with somatization problems.18 The intervention focuses on the reduction of physical distress and somatic preoccupation through training in relaxation techniques, activity regulation, facilitation of emotional awareness, cognitive restructuring, and interpersonal communication. More specific details on this intervention can be found in a recently published book containing a manual and step-by-step guidelines for the conduct of each session.18
Each treatment session took approximately 50 minutes (range, 45–60 minutes) except for the first session, which took about twice as long (average, 90 minutes). The 10 sessions were delivered over 10 to 20 weeks, with an average of about 3 months. Audiotapes were made of most sessions. Therapists received training on the intervention protocol from 2 of the authors (L.A.A., R.L.W.). Therapists’ treatment adherence to the study protocol and competence were rated routinely during the study from evaluations of taped sessions.
Patients were randomly assigned to receive 10 sessions of the CBT-type intervention described above plus a consultation letter (intervention condition) or to receive usual clinical care from their primary care physician plus a consultation letter (control condition). In both groups, clinical care was therefore augmented by sending to the patients’ primary care physicians the consultation letter originally developed by Smith et al,13 slightly modified for use in this study. Patients were assigned to the intervention or control group using a computer-generated random number sequence generated by the study statistician before the study. Study personnel conducting assessments were blinded to the participants’ study group and, hereafter, are referred to as blinded evaluators.
Assessments and Instruments
We assessed study patients first at the screening, next at a baseline visit 1 to 2 weeks later, and then at an end-of-treatment visit immediately after the treatment phase of the study was completed (ie, approximately 3 months after baseline). Patients in the intervention group varied in the amount of time required to complete the 10-session intervention and therefore also varied in the timing of the third assessment. We also conducted a follow-up assessment 6 months after the completion of treatment.
All blinded evaluators were trained to administer the study’s structured clinical interview instruments. The training included role playing of assessments, conducting assessments on patients seeking care for unexplained physical symptoms with trainers present, and supervision by trainers who had listened to audiotapes of the trainee’s assessment sessions. To determine inter-rater reliability, assessment interviews were recorded and rated by an additional experienced evaluator.
The instruments used for assessments included the PHQ,16 a self-report version of the PRIME-MD,17 from which we used the 15 somatic symptoms (PHQ-15)19 as a measure of severity of somatic complaints experienced during the month before the evaluation. The PRIME-MD was used to assess symptoms of mood, anxiety, alcohol use, and eating disorders. We used the somatic symptoms module of the Composite International Diagnostic Interview (CIDI)20–22 to elicit lifetime medically unexplained physical symptoms and to diagnose somatoform disorders. Functional status was assessed with the physical functioning subscale from the Medical Outcomes Study (MOS-10) scale’s Short-Form Health Survey developed by RAND.23,24 We used the Hamilton Rating Scale for Anxiety (HAM-A)25 and the 17-item Hamilton Rating Scale for Depression (HAM-D)26 to measure anxiety and depression symptoms, respectively. A visual analog scale (VAS) derived from the CIDI list of somatic symptoms was used to quantify current somatic symptoms reported by the patient. Symptoms initially reported as present were each rated individually along a 100-mm line that ranged from 0 (not present) to 100 (extremely severe). For the analyses, we calculated the mean VAS score only for those symptoms rated as medically unexplained on the CIDI. A Clinical Global Impressions (CGI) scale anchored on physical symptoms was used to assess both the overall severity of somatic symptoms and the subsequent degree of improvement. The CGI consists of scales that evaluate the global severity and degree of improvement of physical symptoms over time. The rater is trained to judge severity and improvement of physical symptoms based on all information available at the time of each assessment (baseline, end of treatment, and follow-up). At baseline, the severity of somatic symptoms (CGI-severity) was rated on a 7-point scale ranging from “not at all ill” to “among the most extremely ill patients.” At the end-of-treatment and follow-up assessments, the blinded evaluator reevaluated the patient’s overall change (CGI-improvement) compared with baseline, with ratings ranging from “very much worse” through “unchanged” to “very much better.” Similar versions of this global scale have been used in a variety of treatment outcome studies, including some among patients with somatic presentations.27,28
We translated, adapted, and pretested all instruments for use with Spanish-speaking patients. Interrater reliability was carefully assessed and calibrated throughout the study and yielded satisfactory intraclass correlation coefficients for the key instruments (r >0.70).
Data Analyses
The study’s primary outcome measures were the CGI global rating of severity of physical symptoms (CGI-severity) and the CGI rating of improvement of physical symptoms (CGI-improvement). As done in the study of Allen et al,15 treatment response status was determined by transforming the 7-point CGI somatic symptom improvement ratings to binary ratings: patients rated as “much improved” or “very much improved” were considered to be treatment responders, whereas all others were considered to be nonresponders. Secondary outcome measures included the physical subscale from the MOS-10 and the HAM-D, HAM-A, and VAS scores.
We used an intent-to-treat approach, based on data from all randomized participants, in all analyses except the responder analysis described later. We evaluated the intervention and control groups at baseline, at the end of treatment, and at the 6-month follow-up. Unpaired t tests (for continuous variables) or Fisher exact tests (for categorical variables) were used to assess baseline differences between groups. We analyzed the continuous data gathered in the study using a mixed model repeated measures analysis of variance. The fixed effects of treatment in this mixed model included group (intervention vs control), time of assessment (baseline, end of treatment, 6-month follow-up), and the group-by-time interaction. In modeling within-patient error, we used a covariance matrix assuming compound symmetry. The interaction between study group and time in the mixed model was of most interest. When the interaction was significant (P <.05), we performed planned comparisons to assess whether changes in outcome measures observed in the intervention group (between baseline and the end-of-treatment and follow-up assessments) differed from those observed in the control group.
We analyzed response to treatment (responder status), determined by the binary transformation of the CGI-improvement scale, using logistic regression analysis to obtain odds ratios. We entered the CGI-severity rating at baseline in this analysis as a covariate. Patients were considered improved in this binary transformation if their CGI-improvement rating was 1 (“very much improved”) or 2 (“much improved”) and not improved if their rating was 3 or higher.
RESULTS
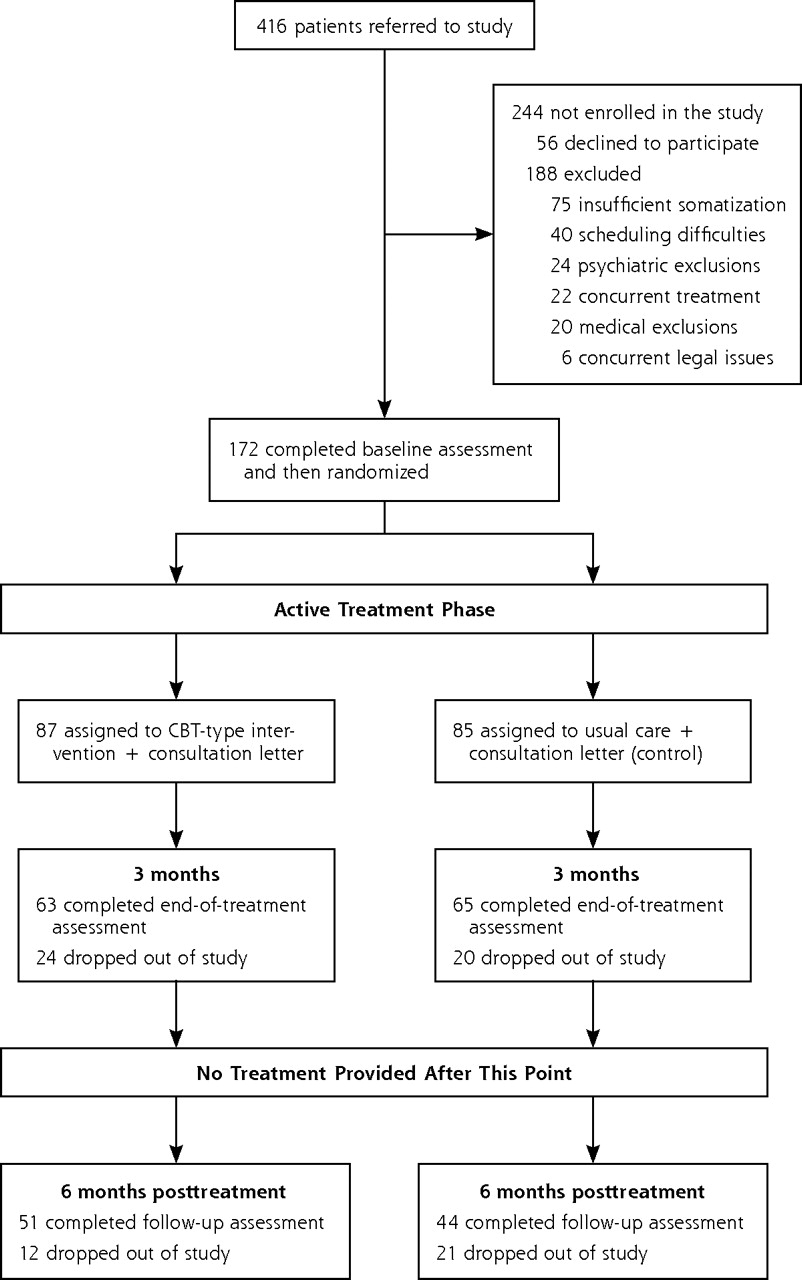
Figure 1⇓ shows patient flow for the study. During the recruitment phase (January 2001 through February 2005), 416 primary care patients were referred to the study. A total of 244 of the 416 patients referred to the study were not enrolled for various reasons (eg, declined to participate, could not make regular visits, or had severe psychiatric problems, such as psychotic symptoms or suicidal ideas, or medical disorders that may have explained the symptoms). A total of 75 of the patients not enrolled were excluded because their symptoms were below the somatization threshold required.
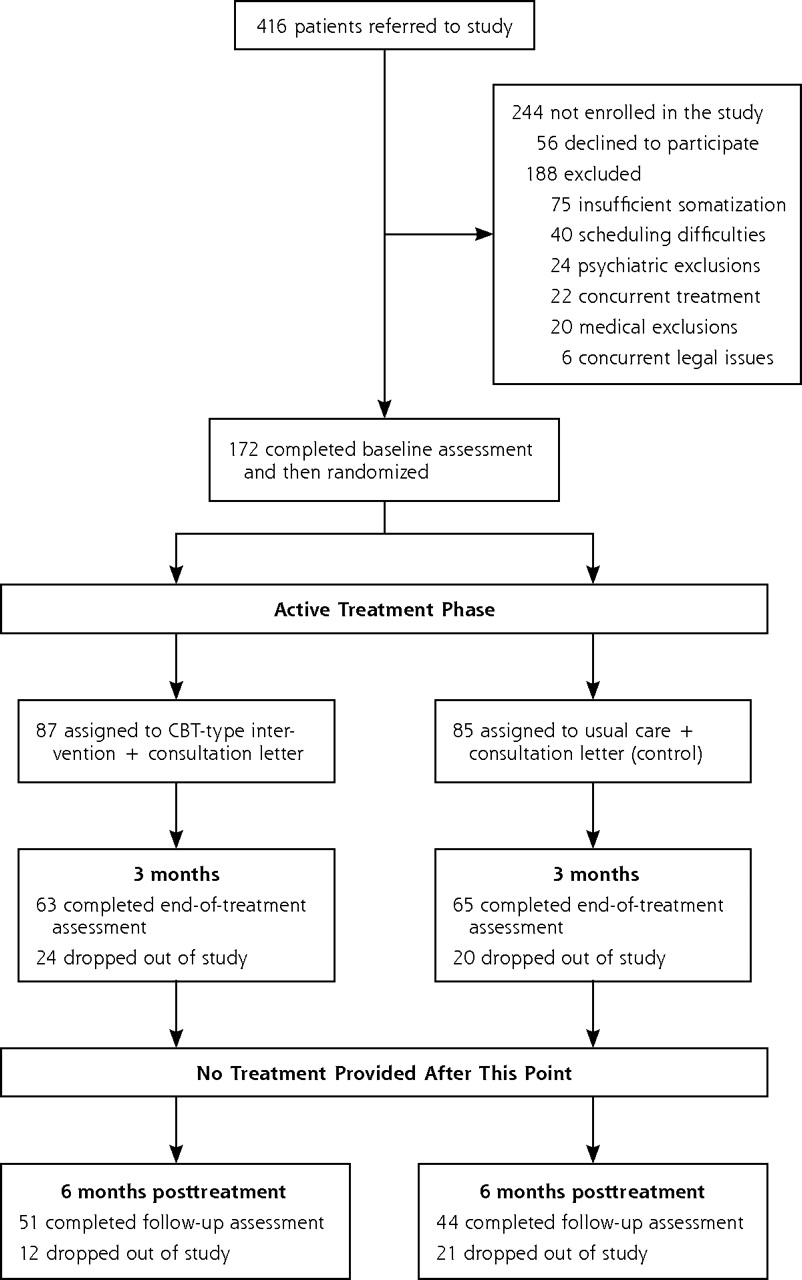
Patient flow.
In the end, 172 patients aged 18 to 75 years formally entered the study and were randomly assigned to the study groups. Table 1⇓ describes their baseline characteristics and shows that there were no significant demographic differences between the 2 study groups. Of these 172 patients randomized, 74% completed the end-of treatment assessment, and 55% completed the 6-month follow-up assessment (Figure 1⇑).
Baseline Characteristics of the Study Patients
Physical Symptoms at Baseline
At baseline, the most common unexplained physical symptoms reported by these patients were pain symptoms, such as headache (70%), back pain (62%), abdominal pain (59%), chest pain (56%), and joint pain (48%). Other common symptoms included feeling faint (54%), excessive flatulence (42%), and lump in the throat (37%).
Psychiatric Symptoms and Medication Use at Baseline
A majority (92%) of all patients entering the study had high levels of depression and anxiety symptoms based on their PRIME-MD, HAM-D, and HAM-A scores. Twenty-six percent of the patients in the intervention group reported taking psychotropic medications (typically antidepressants), compared with 41% of patients in the control group. The effect size was small (Good-man-Kruskal τ = .024; P <.12) and in the opposite direction of what would be expected if medications were to have an effect on outcomes of interest. The use of these medications therefore did not appear to account for the better clinical outcomes observed in the intervention group relative to the control group (described below).
Mixed Model Analyses
Table 2⇓ shows the results of the mixed model analyses for the various outcomes studied. At the end of treatment, there was a significant improvement (group-by-time interaction, P <.05) favoring the intervention group over the control group for physical symptoms (PHQ-15 and VAS scores) and depressive symptoms (HAM-D score). The results of the planned comparisons, conducted when the group-by-time interaction was significant, showed that the intervention group had significant improvements in the PHQ-15, HAM-D, and VAS measures. At the 6-month follow-up, however, the only significant difference observed was in PHQ-15 scores, and there was a trend (P <.07) toward a difference in HAM-D scores; both results favored the intervention.
Changes in Secondary Outcomes by Study Group
Responder Analyses
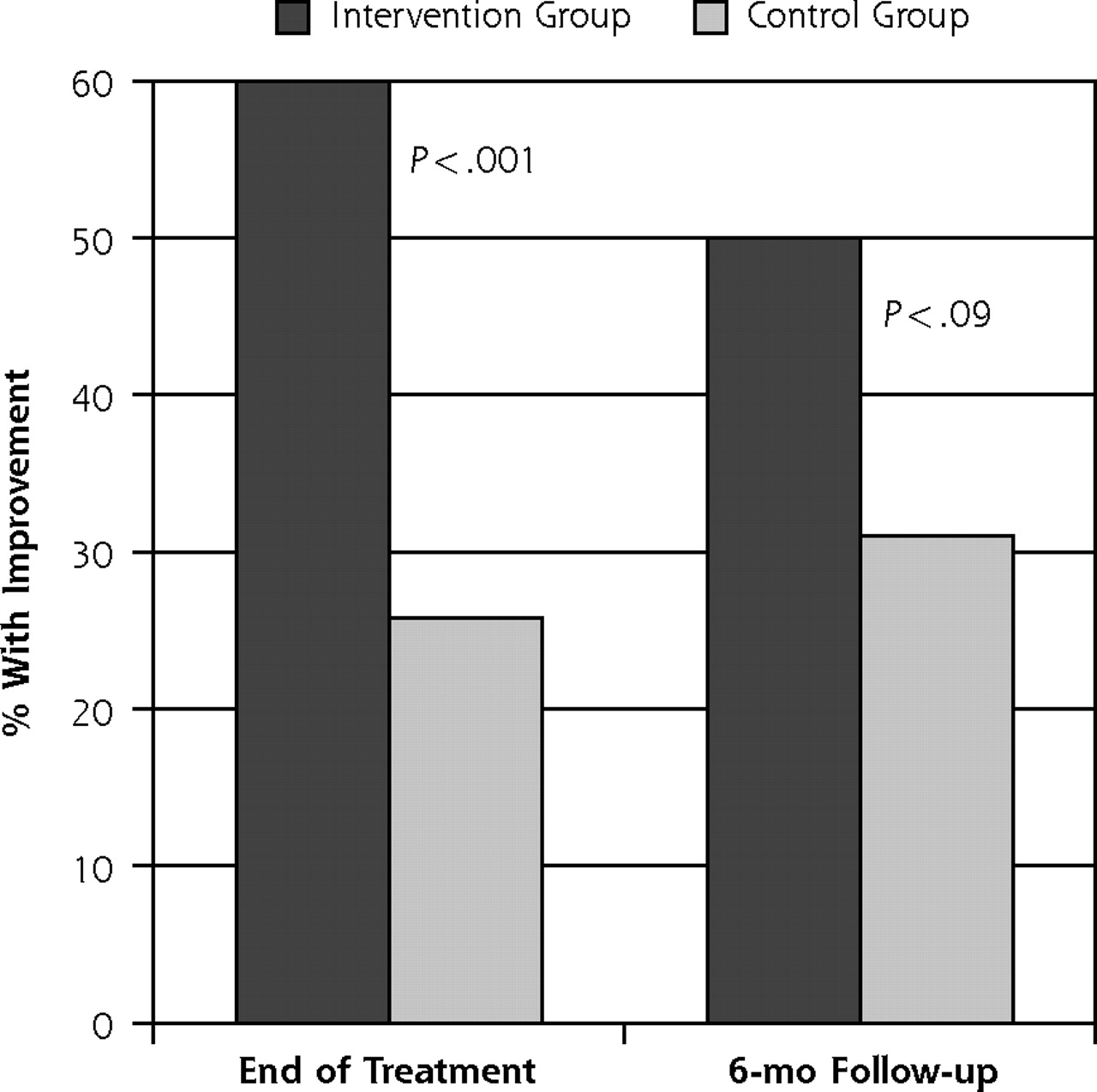
In the analysis of the CGI-improvement for patients with complete CGI data at the end of treatment, a significantly greater proportion of intervention patients were rated by blinded evaluators as “much improved” or “very much improved” at the end of treatment compared with their counterparts in the control group (60% vs 25.8%; odds ratio [OR]=4.1; 95% confidence interval [CI], 1.9–8.8; P <.001) after controlling for baseline CGI-severity (Figure 2⇓). These results suggest that the effects of the intervention were not only statistically significant but also clinically meaningful given that external ratings of “much/very much improved” on the CGI-improvement scale are often used in clinical trials to define clinically meaningful change. At the 6-month follow-up, the effect of the intervention had diminished, with 50% of intervention patients being rated as improved, compared with 31% of control patients (P <.09) (Figure 2⇓).
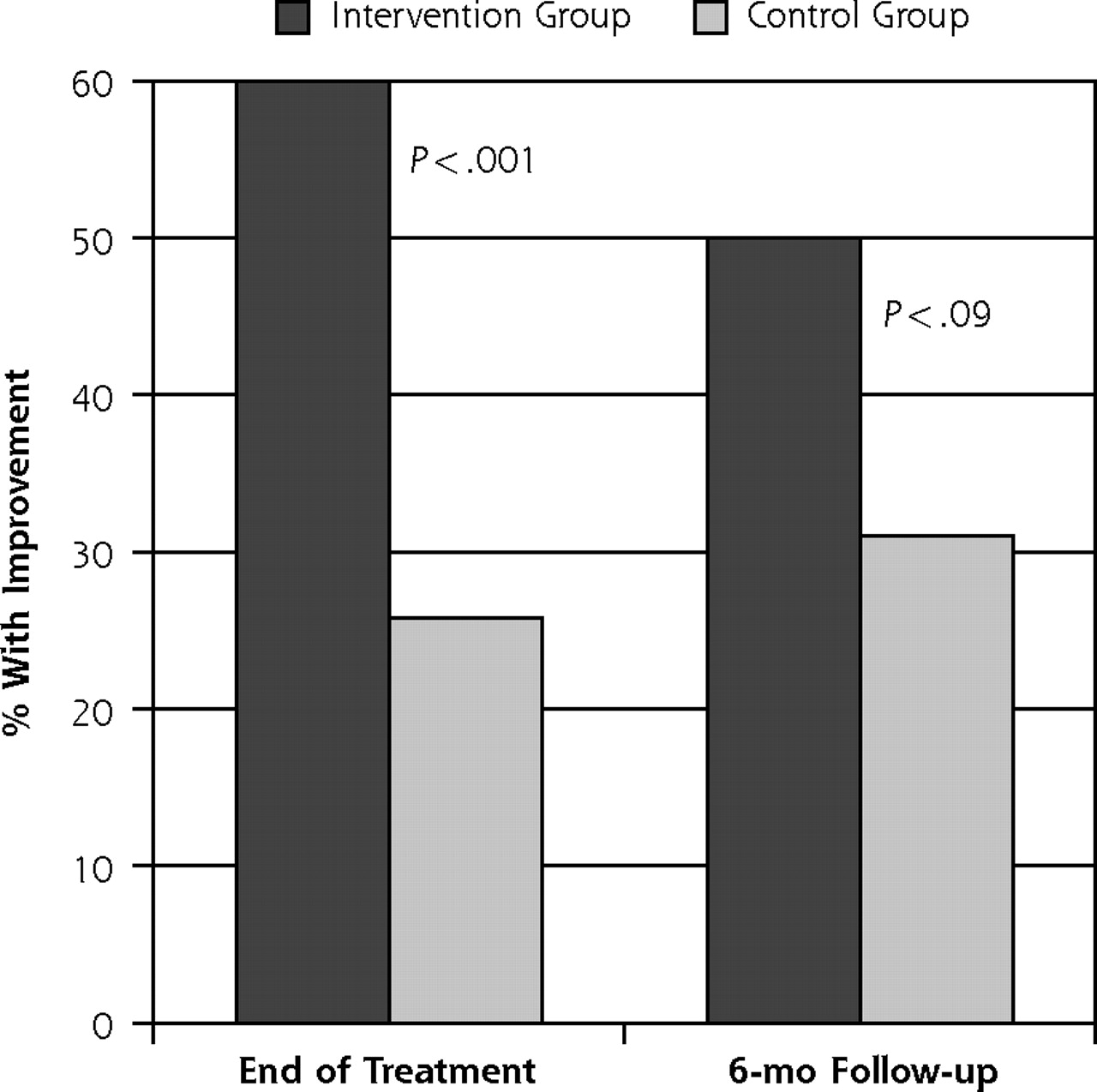
Percentage of patients with an improvement in physical symptoms.
Note: Improvement was defined by a rating of “very much improved” or “much improved” by blinded evaluators on the Clinical Global Impressions improvement (CGI-improvement) scale. P values were derived from logistical regression analyses wherein time and treatment condition were evaluated for their ability to predict responder status.
Effect of Broken Blind
We carefully examined the maintenance of the study blind and whether it may have affected the results. Maintenance was assessed in 3 ways. First, following the end-of-treatment assessment and the follow-up assessment, blinded evaluators completed a measure labeled Diagnostician Assessment of the Blind in which they were asked, “Did a research staff or patient directly tell you the treatment condition?” Second, the follow-up assessments were tape recorded whenever possible (ie, when patients gave consent) and the tapes were reviewed by a blinded assessor to ascertain whether any information had been disclosed that threatened the blind (eg, a patient talked about being in therapy). Third, instances wherein the blind was broken outside the study procedures (eg, a clinician saw a patient in the clinic with a therapist) were reported and accounted for. The blind was considered as possibly broken for a total of 17 patients, 12 of 87 (13.8%) in the intervention group and 5 of 85 (5.9%) in the control group. Eliminating these patients from the analyses did not change the significant benefits of the intervention described above. For example, at the end of treatment, 58.8% of patients in the intervention group and 25.9% in the control group continued to be “much/very much improved” on the CGI-improvement scale (OR = 3.8; 95% CI, 1.6–8.6; P <.002).
Effect of Changes in Depression
To determine whether the difference in physical symptom improvement between groups persisted after controlling/adjusting for changes in depression, given the limits of the data available, we added a difference score to the set of independent variables modeled in the responder analysis. Specifically, we added the difference between HAM-D scores at baseline and end of treatment to the logistic regression analysis, including only patients with complete data. In this analysis, a significantly greater proportion of patients in the intervention group were rated by blinded evaluators as “much/very much improved” at the end of treatment, after controlling for changes in depression scores and for baseline severity of symptoms (OR = 3.5; 95% CI, 1.5–8.3; P <.004).
These findings indicate that the reduction in depression did not account for the improvement in physical symptoms associated with the intervention.
DISCUSSION
The results of this study show that a time-limited, CBT-type intervention administered at primary care sites by trained psychologists was significantly more effective than usual care for managing patients with unexplained physical symptoms. This same intervention had been previously shown to be efficacious in a randomized controlled trial for patients with more severe forms of somatization when delivered in a mental health setting.15 The current study therefore extends those findings to an ethnically diverse sample of primary care patients with less severe somatic symptoms who were all managed within the same primary care environment wherein they sought care.
Overall, the clinical effect of the intervention was relatively modest and was most noticeable in terms of physical symptoms. Substantial relief of medically unexplained physical symptoms was observed in about 60% of the patients who completed the intervention and persisted for months afterward, although the degree of improvement gradually diminished. This intervention targeted only physical symptoms but also led to a decrease in depressive symptoms, although this effect was less sustained with time.
We made particular efforts to protect the blind in this study and carefully monitored cases in which the blind might have been broken. Between-group differences remained significant even when those few cases in which the blind may have been broken were excluded from the analyses.
Our study did have a number of limitations, nonetheless. First, the study took place in university-based, urban primary care clinics, and less than one-half of patients referred by primary care clinicians were enrolled in the study. Our results may therefore not apply to nonacademic, rural clinics and or to a large segment of the primary care population seeking care for unexplained symptoms. Second, even though we used a control group, patients in this group necessarily made fewer visits to their physicians than did patients in the intervention group; therefore, we cannot rule out nonspecific effects of increased visits and physician attention as explanations for the better outcomes in the intervention group. We think it unlikely that such contact played a major role in this instance because reassurance alone does not appear to provide much benefit to patients with unexplained symptoms.29 Third, the study did not assess other important outcomes, such as use of services (primary care, medical specialty, or mental health services), costs, or patient and physician satisfaction. Fourth, the overall treatment completion rate was far from perfect (74%), but for a study done in a busy primary care site, this value compares favorably with that of other studies.11,30,31 The attrition rate at follow-up was particularly high and may have inordinately attenuated statistical power at the follow-up time point, and the only sustained result that could be observed at follow-up was for the PHQ-15, an instrument that measures severity of somatic symptoms. We did not note any sustained significant changes in depression, anxiety, or physical functioning level as a consequence of the intervention. The lack of a sustained effect in the latter domains may be due to inadequate power at follow-up to detect smaller effects, the focus of the intervention on physical symptoms (not depression or physical functioning per se), or perhaps both.
Although this CBT-type intervention is rather elaborate and time-consuming for busy primary care sites, we were able to show that it could be effectively administered in these 2 urban, university-affiliated clinics. We believe that with proper training of clinicians, the intervention described herein should be relatively easy to implement in many primary care settings, particularly those where mental health consultation can be made available.
Finally, the clinical response to treatment ranged broadly (ie, some patients had a robust response, whereas others had a partial response or none at all), suggesting that some patients may require fewer sessions or less intensive intervention, whereas others may require more. A staged approach to care including several progressive treatment steps (brief educational videos, biofeedback, CBT, additional treatment sessions, or the addition of medications) therefore needs to be considered for future studies as well as for current practice.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: Supported by grants 1RO1MH 60265-01, R21 MH52584, and 1P20MH74634-01 from the National Institute of Mental Health.
- Received for publication November 28, 2006.
- Revision received February 22, 2007.
- Accepted for publication March 17, 2007.
- © 2007 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cognitive behaviour therapy for long-term frequent attenders in primary care: a feasibility case series and treatment development study
- Comparing cognitive-behavioural psychotherapy and psychoeducation for non-specific symptoms associated with indoor air: a randomised control trial protocol
- Somatoform disorders in litigation: causation and prognosis
- Somatic symptom count scores do not identify patients with symptoms unexplained by disease: a prospective cohort study of neurology outpatients
- Effectiveness research on psychosocial interventions among high-utilising patients in primary care
- Effectiveness of Group Versus Individual Cognitive-Behavioral Therapy in Patients With Abridged Somatization Disorder: A Randomized Controlled Trial
- Role of mental health professionals in the management of functional somatic symptoms in primary care
- Guided self-help for functional (psychogenic) symptoms: A randomized controlled efficacy trial
- 'You Complete Me'
- In This Issue: Clinical Diagnosis and Management