
Abstract
PURPOSE We report a study on the developmental status of human resource staffing and service functions of community health services (CHS) in China and offer recommendations for improving the CHS in the future.
METHODS A study questionnaire was completed by 712 CHS organizations distributed in 52 cities and districts in all areas of China using a multilevel stratified randomized sampling method. Data were collected on the backgrounds, human resources, and service functions of CHS organizations.
RESULTS We found that 68.2% of doctors and 86.5% of nurses employed in CHS centers have low-level medical training. The doctor-nurse ratio in CHS centers is 1.2 to 1 and in CHS stations is 1.3 to 1. More than 50% of CHS organizations have developed on-the-job training programs, causing cost trends for staff training to increase. Although the delivery of basic clinical services and public health services is steadily increasing, 58.6% of stations are open less than 12 hours per day. Health records are established in a high proportion of CHS organizations. Two kinds of health education—general public health education, and personal education for specific problems—have been adopted by more than 92% of CHS centers and 90% of CHS stations.
CONCLUSIONS Desired functions for CHS organizations have been partially achieved. Training for doctors and nurses engaged in CHS should be promoted and improved as quickly as possible. Training in basic clinical services and management of noncommunicable chronic diseases should be strongly promoted. Changes in government policies should be pursued to promote effective support for the development of CHS.
INTRODUCTION
China is undergoing the most rapid industrialization and urbanization in the history of humankind. As a result, both the level of education and the expectations of the population have increased. The Chinese government is revising its approach to how medicine is practiced within the health care system. At present, one important task is how best to develop community health services (CHS) centers throughout China. To realize this effort, it is necessary to understand the context of China’s medical education and health care system.
China’s Medical Education System
In China, medical educational programs include 5- to 8-year post–high school training programs, 3-year post–high school programs, 4-year post–middle school programs, and barefoot doctors.1 The 3-year post–high school programs and 4-year post–middle school programs were copied from the Soviet Union and were adopted by China after the Cultural Revolution in 1976. Currently, 5- to 8-year post–high school training is the most frequently used medical training program. The 3-year post–high school programs are decreasing, and 4-year post–middle school programs have almost disappeared. Because local physicians were in short supply when P. R. China was founded in 1949, the so-called barefoot doctors, who were basically farmers with no proper medical education, usually only 3 to 6 months of basic medical training, took care of the primary health care needs in their communes.2,3 Today, on-the-job training is being emphasized for the remaining group of barefoot doctors.4
China’s Medical Professional Titles
The term physician in China refers to medical health care professionals who come from a wide range of educational backgrounds: 5- to 8-year post–high school training programs, 3-year post–high school programs, 4-year post–middle school programs, and barefoot doctors.1 The 3 levels of professional physician titles—senior, middle, and junior—are based primarily on length of training. A junior doctor from a 5-year post–high school training program usually needs about 5 years of medical practice to move from the junior to the middle level and a total of 15 years to achieve the senior-level professional title. A basic health care clinician with a 3-year post–high school program or 4-year post–middle school program will need much more practical time to reach a higher professional title. Generally, the higher the medical degree achieved, the less practical time will be needed to attain a higher professional title.
China’s Medical Care System
The Chinese government has 2 health care systems, one based on hospital systems and the second based on CHS centers. Hospital systems are developed around tertiary and secondary hospitals in cities and around township hospitals in rural areas. CHS organizations include CHS centers and their affiliated stations.
Chinese Community Health Services
At present, China faces several major health care problems.
-
The population is aging. In 2005, persons older than 65 years of age accounted for 7.69% of China’s total population.5 China, however, has no geriatric subspecialty to manage chronic disorders and comorbid conditions in elderly patients in communities.3
-
There is an uneven allocation of health care resources between urban and rural areas. Sixty-two percent of the population of China lives in rural areas, whereas 80% of the medical institutions are concentrated in cities. In 2005, high-level medical resources tended to be concentrated in large-capacity hospitals.5 Only 29% of Chinese people have health insurance. Out-of-pocket expenses accounted for 58% of health care spending in China in 2002.2
-
The types of diseases are changing. The causes of morbidity and mortality have shifted from acute infectious and communicable diseases to chronic non-communicable diseases.
-
There is a strained relationship between patients and physicians. Country doctors have limited training, and many peasants seek care directly from specialists at large hospitals. Busy specialists often have insufficient time to communicate adequately with patients. There are 2 major complaints emerging from the Chinese people: they report that it is “expensive health care to receive” and that they have “inconvenient access to health care.”1
To address these problems, China has drafted new goals and approaches to medical education and the medical care system that are directed toward improving the health of China’s huge population.3 Family medicine training (ie, general practice) and family physicians (ie, general practitioners) were introduced to China at the end of the 1980s.6
Family medicine (general practice) achieved formal status as an academic discipline in medical schools in 1999.3 Several education and training programs for family medicine include basic sciences and theory of family medicine in medical schools, on-the-job training programs, continuing education for family doctors,1 and residency training programs. Of the many levels of physician training in China, doctors who work in CHS organizations often have 3 or fewer years of professional training and are still widely referred to as family doctors, ie, general practitioners.
China initiated its CHS program in 1997. Since then, the CHS has become an important part of medical care through which continuing and comprehensive health care can be provided. The public health responsibility for promoting good health in all age-groups can be increased in community settings by family doctors (general practice doctors) and their primary care teams. The scope of the CHS organization is described symbolically by the government as “1 body, 6 aspects.” The body is the CHS organization. The 6 aspects consist of basic clinical services, prevention, health education, women and children’s care, elderly care, immunizations, and physical rehabilitation.1,3,6
CHS centers and stations have similar functions but have different service populations. A center is in charge of 3 to 6 stations for every 30,000 to 100,000 residents according to the size of a region, and each station provides services to about 10,000 residents. The station reports cases to the CHS center, and the latter collates and reports cases to the local health administration department. Both the centers and stations are paid primarily by the government.7
By the end of the 2002, 2,406 CHS centers and 9,700 CHS stations had been established in China.2
To understand our suggestions for improvement of CHS in China (which we based on our experience), it is necessary to describe the status of human resources and service functions of CHS found by this national survey.
METHODS
Our survey was conducted by questionnaire interview in August and September of 2003. The questionnaire was made up of a standard set of questions for directors of selected CHS centers, including questions on background information, human resources, and service functions.
Sampling Methods
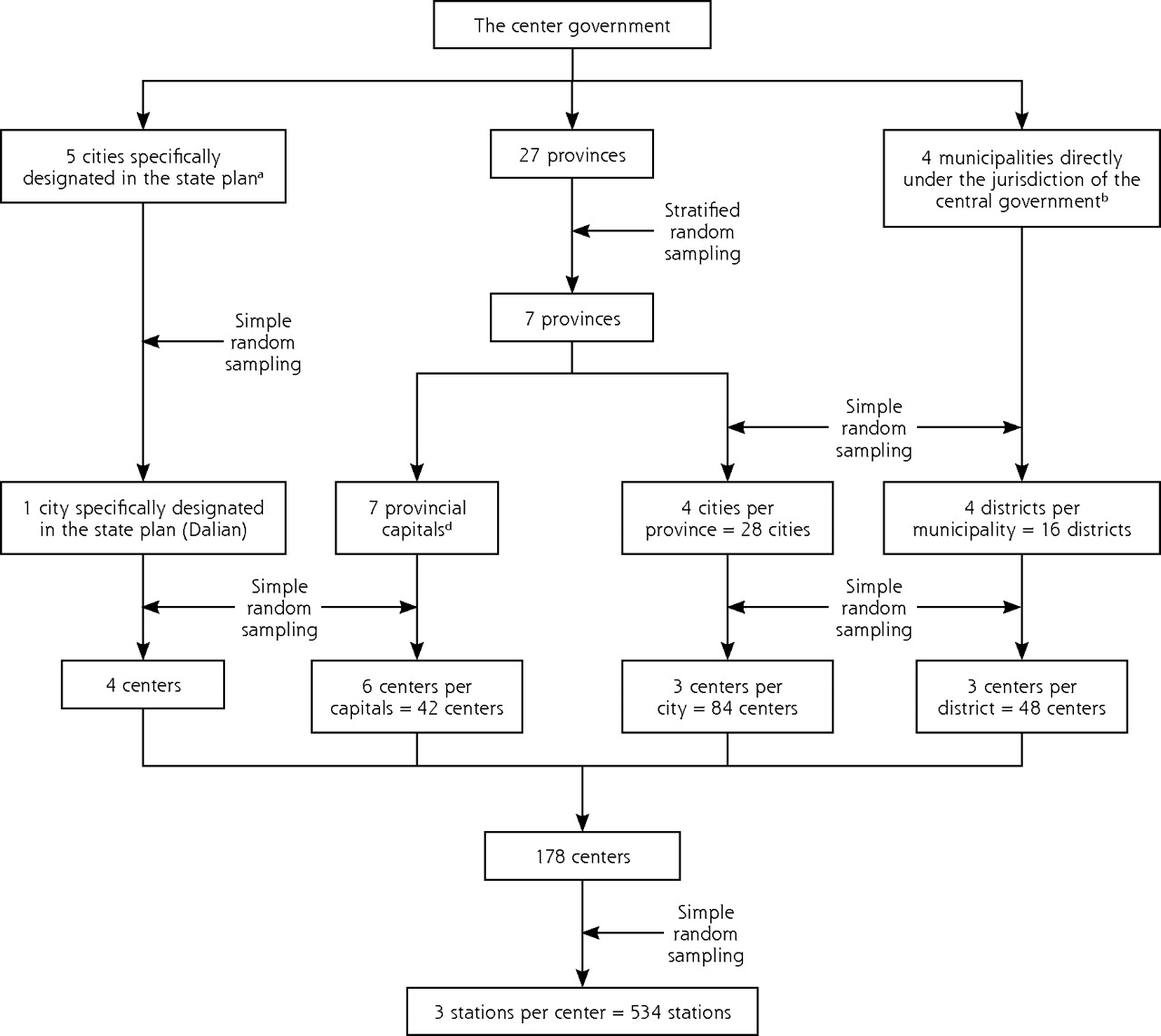
Following suggestions from the Ministry of Health of China, about 7% of CHS organizations, including centers and stations (712) were selected by the multilevel stratified random sampling method (Figure 1⇓).
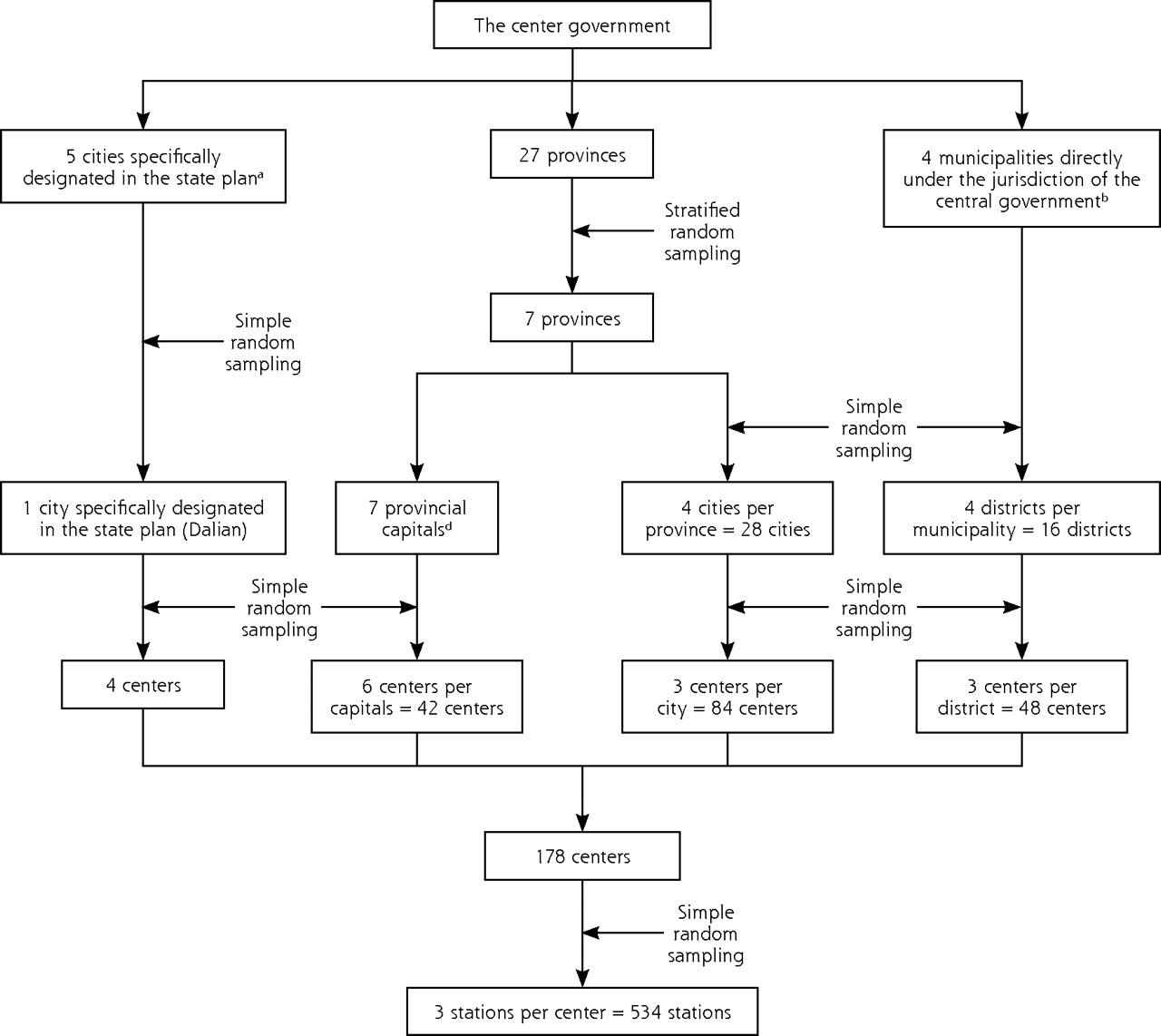
Sampling flow of community health services centers and stations in 2003 in China.
a Five cities specifically designated in the state plan (this city is similar in size to a provincial capital) include Xiamen, Ningbo, Qingdao, Shenzhen, and Dalian, which are controlled by provincial governments politically and managed by the central government economically.19
b Four municipalities (a municipality is roughly equivalent to a province) are directly under the jurisdiction of the central government, including Beijing, Shanghai, Tianjin, and Chongqing.
c Considering level of local economic as a stratification factor, 27 provinces were stratified into 7 strata. Every stratum includes 4 provinces with similar economic levels, except 3 provinces in the last stratum. Each province was selected from every stratum by simple random sampling.
d Seven capitals of selected provinces were selected in terms of economical and political characteristics.
Training Programs for This Survey
For the survey 2 training programs were conducted, 1 for trainers and 1 for interviewer training. The trainer program was conducted by 4 researchers of the Ministry of Health of China in Beijing, in which 12 trainers came from 7 provinces, 4 municipalities, and Dalian. The interviewer-training programs were conducted by 11 trainers in selected provinces; 51 interviewers came from 7 provincial capitals and 28 cities, and 16 districts and municipalities. A standardized training manual and methods were used in the training programs.
Fifty-two interviewers, including 1 trainer from Dalian, conducted interviews with 178 directors from 178 selected CHS centers. Because 534 selected CHS stations are affiliated with the 178 selected CHS centers, both the centers’ and stations’ questionnaires were answered only by directors of the centers. One hundred seventy-eight interviews were conducted, and the completed questionnaires were mailed by 52 interviewers to the Ministry of Health.
Quality Control
There were 3 steps to develop the questionnaire. Initially question lists were developed by collecting and extracting information from references. The questions were then evaluated by a formal consensus process based on a nominal group technique. Finally, the questionnaire was defined by a pilot survey.
We conducted the pilot survey on 14 directors of CHS organizations from 2 districts of Beijing and Tangshan, and we assessed internal consistency reliability (Cronbach’s α) and reproducibility (over a 1-month period in 14 stable directors) of the questionnaire. The questionnaire was internally consistent (Cronbach α = .80) and reliable (intraclass correlations = 0.80 and 0.85). Content validity of the questionnaire was also confirmed by epidemiologists and statisticians. The results indicated that the questionnaire has good reliability and validity.
The interview was conducted face to face between interviewers and interviewees. The interviewees were assured that they would remain anonymous during the interview and the analysis. There was a strict review process and supervision by the team to ensure the survey quality. Data were entered twice independently and checked for errors to enhance the accuracy.
Data Analysis
Descriptive statistical methods were used to analyze the data by using SAS, version 8.01 (SAS Institute Inc, Cary, North Carolina).
RESULTS
Human Resource Staffing in CHS Organizations of China in 2003
Compared with centers, CHS stations do not have a sufficient number of doctors and nurses (Table 1⇓), and they have lower professional titles and less thoroughly trained medical backgrounds and (Tables 2⇓, 3⇓). The doctor-nurse ratio is about 1.2 to 1 in CHS centers and 1.3 to 1 in stations (Table 1⇓).
Average Number of Different Staff Positions in CHS Organizations in 2003 in China
Average Designation of Professional Titles in CHS Organizations in 2003 in China
Average Number of Doctors and Nurses and Their Medical Educational Background in CHS Organizations in China, 2003
More than 50% of CHS organizations have developed the on-the-job training programs. Expenditures for staff training have increased from 2000 to 2002, and the percentages of training costs in the total expenditures of CHS centers and stations are also rising (Table 4⇓).
Average Staff Training Expenditures per CHS Organization, 2000–2002 (USD:RMB = 1:7.7)
Service Functions of CHS Organizations of China in 2003
The basic clinical and public health services provided by CHS organizations have increased from 2000 to 2002 (Table 5⇓). Although the hours of operation approach 24 hours a day in most of the CHS centers, the operating hours of CHS stations are often insufficient (Table 6⇓). CHS centers provide more public health services than do stations, and the proportion of CHS organizations establishing health records is at a high level (Table 7⇓). The discrepancy between the total number of centers and stations in Tables 6⇓ and 7⇓ and total number in Figure 1⇑ is due to administrative changes between 2002 (the year when the sampling materials were produced) and 2003 (the year when the fieldwork was done); some township-level units were split into 2, each with its own health center.
Quantity of Some Services Provided by All CHS Organizations From 2000 to 2002 (in Thousands)
Hours of Service Availability in CHS Organizations in China
CHS Organizations Providing Different Public Health Services in China in 2003
The number of CHS organizations providing management of noncommunicable chronic diseases increased markedly from 2000 to 2002 (Table 8⇓).
Number of Noncommunicable Chronic Disease Management in CHS Organizations in China, 2000 to 2002
Many methods for health education in CHS have been developed. Most CHS organizations have adopted visual health educational materials, health consultation, and oral education presentations in clinics.
DISCUSSION
Human Resources in CHS Organizations
Nurses play an important role in taking care of patients in CHS organizations, especially in the management of noncommunicable chronic disease, family (home) care patients, and home visits. Because CHS stations are usually distributed in residential areas, residents can visit a family (general) doctor conveniently at those stations. There is an obvious need to allocate more doctors and nurses to stations. The central government is using several methods to attract more doctors and nurses with better educational backgrounds to work at CHS organizations and to reach the aim of a doctor-nurse ratio of 1 to 1 or more,7 including service lists for CHS organizations, raising salaries for medical staffs based on finished tasks, and providing more opportunities to participate in continuing medical education programs and academic conferences.
When CHS was first developed, the Chinese government provided more support for comprehensive hospitals than for CHS organizations. The result was a huge disparity between the 2 systems in salary and opportunities for promotion. Many doctors and nurses with better educational backgrounds or higher professional titles preferred to work at hospitals. Patients naturally elected to see doctors in hospitals because of their higher prestige and perceived levels of training.8
The Chinese government implemented several programs since 2000 to improve the competency of the less-educated doctors and nurses in CHS organizations, especially station staff. First, the central government established favorable policies for CHS workers, for example, by raising salaries and subsidies and shortening tenure periods for promotion to higher professional titles, in an attempt to attract experienced doctors and nurses to take jobs in CHS organizations.9 Second, some specialists from tertiary hospitals are encouraged to take on part-time work in CHS organizations. Third, the government provides on-the-job training programs, degree advancement education programs, and practical skills training programs for CHS doctors and nurses, and it gives them more financial support to finish these programs.6
Such on-the-job training programs, which provide opportunities for trainees to improve their skills and obtain a higher professional title, will result in the retraining of most of the less-educated professionals currently working in CHS organizations and allow them to become eligible family (general) doctors in accordance with the national training standards. Incentives of ¥1500 and ¥900 will be paid for 1 family doctor and 1 nurse to complete 300 and 200 study hours, respectively.7 Meanwhile, costs for this program will be audited by provincial health administration departments.10
Service Functions in CHS Organizations
CHS organizations provide basic clinical and public health services. Basic clinical services consist of diagnosis and treatment of common diseases, traditional Chinese medicine, emergency care, family (home) care beds, home visits, and referral services. Public health services include management of noncommunicable chronic diseases, maternal and child care, elderly care, resident health record management, health care contracting, physical rehabilitation, planned immunizations, and health education.7
The number of family (home) care beds and home visits is increasing gradually. Family (home) care beds are convenient for the family and allow the doctor to visit patients at home so that patients receive better medical care. Although the family (home) care beds are considered necessary by family doctors and patients, the heavier work burden and lower service reimbursement have limited their numbers. It is therefore essential to define reasonable service lists and improve pay to increase the number of family (home) care beds.11
Home visits are considered a useful basic clinical service for CHS. Home visits can be used to assess discharged patients and to manage patients with noncommunicable chronic diseases in the home.12 Currently the home care team, which includes a family doctor, a nurse, and preventive medical staff, is responsible to implement this task in each CHS organization. The rules relating to home visits and their funding are still in the process of being upgraded.
The 2004 survey results showed that operating hours were shorter in stations than in CHS centers. For most residents, the stations are closer to their homes, and thus the doctors or nurses are more accessible and visiting them is more convenient.13,14 The residents hope that stations will increase their open hours, especially for emergency and night services. The central government is considering enriching medical staff in stations and giving more subsidies to help stations prolong their hours of operation.15–17
Public health services are a primary component of CHS. The core tenets of public welfare are embodied in these services. Care for children includes establishing children’s health records and vaccinating children aged 0 to 6 years, regular well-child periodic visits, and supervision of their care. Maternal care includes periodic health examinations, health education, and birth defect monitoring. Through maternal care, the health status of pregnant woman can be effectively supported, and fetal development can be followed medically. Maternal care plays an important role in reducing the mortality and morbidity of pregnant women and neonates.
An accurate and organized health record is important to CHS: (1) doctors record their diagnosis and treatment strategies in the health record; (2) the health record embodies the essential principles of availability of information, which contributes to the continuity of general practice and reflects the biopsychosocial medical model; (3) the health record is the legal record for CHS; and (4) the health record becomes a tool for the assessment of the quality of CHS care.18
In China, the overall disease profile now resembles that of a developed country, with more than 78% of deaths caused by noncommunicable chronic diseases in 2003.20 It is important for medical staff to prevent and treat noncommunicable chronic diseases effectively, and the Chinese government believes improving the management of noncommunicable chronic diseases in CHS centers and stations is essential. The following steps are being undertaken to facilitate chronic disease management: (1) establishing a CHS information system in many provinces that includes a patient registry and reminder system; (2) emphasizing the role of work teams in the management of noncommunicable chronic diseases; and (3) developing clinical guidelines for treating noncommunicable chronic diseases.
Health education is considered an important way for enhancing health and of helping people access health care.19 There are 2 main methods of health education used in CHS organizations in China. One is public health education for all residents, in which visual health educational materials, health leaflets, videodiscs, and health classes are used. The other is education for patients, called personal education, which helps patients to acquire medical knowledge of self-care techniques. Because the population with health problems usually want to get more information, this personal education can be conducted easily by family doctors and is actively welcomed by patients.
There has not been any follow-up since the initial national CHS survey in 2003. Another national survey is needed to update these data so we can generate more feedback for experience-based suggestions and can apply theoretical analysis for improving the Chinese CHS.
Acknowledgments
We are grateful to staff from the Ministry of Health of the People’s Republic of China for support and technical advice; to Liqun Liu for his help in designing the survey; to Jing Guan for her help in fielding the survey; to Yuxiang Yan for her help in organizing and analyzing the data; and to Kurt C. Stange, Xijuan Fu, Wei Wu, and Shige Song for helpful comments on an earlier version of the paper. We also appreciate O. Daniel Smith, MD, family physician for his editorial assistance.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: The research was financially supported by the Ministry of Health of the People’s Republic of China.
- Received for publication October 11, 2007.
- Revision received March 18, 2008.
- Accepted for publication March 27, 2008.
- © 2008 Annals of Family Medicine, Inc.




{kind=link}
Jump to section
Related Articles
Cited By...
- Overprescribing In China, Driven By Financial Incentives, Results In Very High Use Of Antibiotics, Injections, And Corticosteroids
- Development of undergraduate family medicine teaching in China
- Measuring quality in the therapeutic relationship--Part 1: objective approaches
- Funding for Primary Care (or Lack Thereof) and Community Health Centers: Impact of Title VII Training Programs
- In this Issue: Access to Care, Spirituality, and Relevant Research