
Abstract
PURPOSE Recent clinical practice guidelines on prostate cancer screening using the prostate-specific antigen (PSA) test (PSA screening) have recommended that clinicians practice shared decision making—a process involving clinician-patient discussion of the pros, cons, and uncertainties of screening. We undertook a study to determine the prevalence of shared decision making in both PSA screening and nonscreening, as well as patient characteristics associated with shared decision making.
METHODS A nationally representative sample of 3,427 men aged 50 to 74 years participating in the 2010 National Health Interview Survey responded to questions on the extent of shared decision making (past physician-patient discussion of advantages, disadvantages, and scientific uncertainty associated with PSA screening), PSA screening intensity (tests in past 5 years), and sociodemographic and health-related characteristics.
RESULTS Nearly two-thirds (64.3%) of men reported no past physician-patient discussion of advantages, disadvantages, or scientific uncertainty (no shared decision making); 27.8% reported discussion of 1 to 2 elements only (partial shared decision making); 8.0% reported discussion of all 3 elements (full shared decision making). Nearly one-half (44.2%) reported no PSA screening, 27.8% reported low-intensity (less-than-annual) screening, and 25.1% reported high-intensity (nearly annual) screening. Absence of shared decision making was more prevalent in men who were not screened; 88% (95% CI, 86.2%–90.1%) of nonscreened men reported no shared decision making compared with 39% (95% CI, 35.0%–43.3%) of men undergoing high-intensity screening. Extent of shared decision making was associated with black race, Hispanic ethnicity, higher education, health insurance, and physician recommendation. Screening intensity was associated with older age, higher education, usual source of medical care, and physician recommendation, as well as with partial vs no or full shared decision making.
CONCLUSIONS Most US men report little shared decision making in PSA screening, and the lack of shared decision making is more prevalent in nonscreened than in screened men. Screening intensity is greatest with partial shared decision making, and different elements of shared decision making are associated with distinct patient characteristics. Shared decision making needs to be improved in decisions for and against PSA screening.
INTRODUCTION
Screening for prostate cancer using the prostate-specific antigen test (PSA screening) is a common practice in the United States. Each year approximately 40% to 50% of men aged 50 years and older undergo PSA screening,1 often without their knowledge.2–6 The test has become so routine that in one highly publicized case a physician was sued for malpractice for not ordering it.7 Yet PSA screening remains controversial.8,9 The PSA test has limited accuracy, and evidence for its effectiveness in reducing mortality is conflicting.10 Prostate cancer has a heterogeneous natural history; although fatal in some men, it is indolent in most, and outcomes for individuals are difficult to predict. PSA screening can thus lead to overdiagnosis and unnecessary diagnostic evaluation and treatment. For these reasons, professional organizations, including the US Preventive Services Task Force (USPSTF), American Cancer Society (ACS), and American Urologic Association (AUA), have issued clinical practice guidelines recommending that clinicians inform patients about the pros, cons, and uncertainties of PSA screening, and that screening decisions be based on patient preferences.11–13 These elements are essential for informed decision making14,15 and for shared decision making.14–16
PSA screening decisions in the United States, however, fall short of these ideals. National surveys have shown that many men who undergo PSA screening are poorly informed, and screening decisions are typically made by clinicians alone.17–21 PSA screening in the absence of shared decision making exposes men to its potential harms without their knowledge and has been a dominant focus of policy debates.4,17,19,22 The USPSTF’s revised guidelines address this problem by not only discouraging routine screening, but recommending that physicians “should not offer or order PSA screening unless they are prepared to engage in shared decision making.”10,22,23
A problem that has attracted less attention is nonscreening, or test nonuptake,24 in the absence of shared decision making. This problem is equally important if one believes that existing evidence remains insufficient to recommend for or against screening, as critics of the revised USPSTF guidelines have argued,25–27 yet empirical data on its extent are lacking. National surveys have measured shared decision making in PSA screening rather than nonscreening—focusing on men who have undergone screening18 or considered it during some recent time interval.19 They have also used either brief measures of shared decision making18,19 or smaller, nonrepresentative sample populations.28 We thus have an incomplete understanding of the extent of shared decision making in PSA screening and the implications of alternative policy approaches to this problem.
The objective of the current study was to provide population-level evidence on the prevalence of shared decision making in both PSA screening and nonscreening. Using a large nationally representative health survey of the US public, we ascertained the extent of physician-patient discussions of the advantages, disadvantages, and uncertainties associated with PSA screening among screened and unscreened men aged 50 to 74 years. We then conducted analyses to (1) estimate the US population prevalence of both PSA screening and nonscreening in both the presence and absence of shared decision making; (2) examine the association between critical elements of shared decision making and PSA screening uptake and intensity of use; and (3) identify patient characteristics associated with shared decision making.
METHODS
Data Source and Study Population
We used data from the 2010 National Health Interview Survey (NHIS), an annual survey of the public conducted by the National Center for Health Statistics, and a principal source of health information on the US civilian, noninstitutionalized population.29 The NHIS collects information on sociodemographic characteristics, health status, and health care utilization, and in 2010 the NHIS included a Cancer Control Supplement, developed and cosponsored by the National Cancer Institute and the Centers for Disease Control and Prevention. The NHIS obtains a nationally representative sample of US adults using complex random, stratified, clustered, multistage sampling with oversampling of African-American and Hispanic households. In-person interviews are conducted by US Census Bureau interviewers. Methodological details are at http://www.cdc.gov/nchs/nhis.htm.
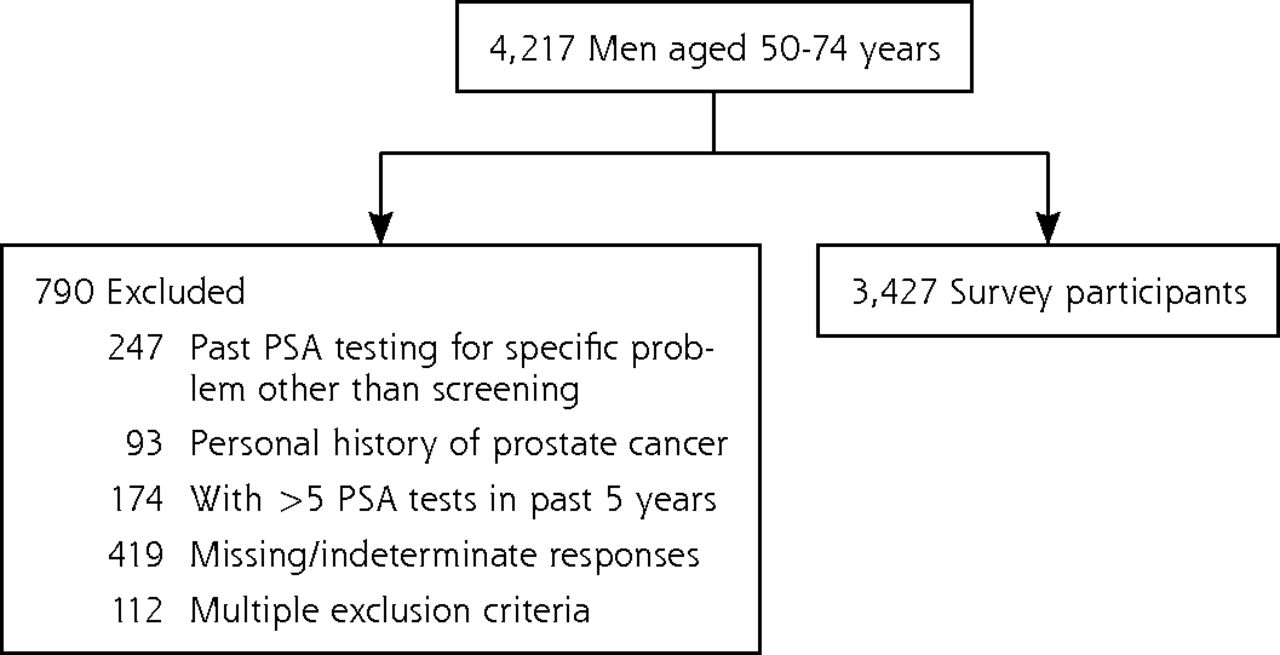
Male respondents were asked whether they ever had a PSA test; those responding yes were asked the date and main reason for their most recent test: (1) part of a routine physical examination/screening test, (2) because of a specific problem, and (3) other. Our analysis included men who reported either testing for routine screening or no past testing. We included men aged 50 to 74 years to reflect the most conservative screening age recommendations of the clinical practice guidelines at the time.11,12 We excluded men who reported testing for a specific problem, a personal history of prostate cancer, or more than 5 PSA tests in the past 5 years, given that high-frequency testing is almost always undertaken for diagnostic rather than screening purposes.
Conceptual Definitions and Measures of Shared Decision Making
Definitions of shared decision making vary in conceptual breadth and number of essential elements.30–33 We defined shared decision making in accordance with ACS, AUA, and USPSTF guidelines for PSA screening that existed during the 2010 NHIS; all recommended that patients be provided with key information about the advantages, disadvantages, and uncertainties of PSA screening, and that patients’ preferences be considered.12,13,16 These essential elements of informed decision making31,32 constitute shared decision making when facilitated by health care clinicians.14–16 All 3 guidelines in 2010 recommended shared decision making, assigning responsibility to “health care providers,”16 “clinicians,”13 or “physicians”12 to inform and involve patients in screening decisions. Correspondingly, we focused on shared decision making and the extent to which physicians provided key information to patients.
Physician discussion of advantages and disadvantages were measured using 2 items: (1) “Did a doctor ever talk with you about the advantages of the PSA test?” and (2) “Did a doctor ever talk with you about the disadvantages of the PSA test?” Physician discussion of uncertainty was measured by a single item: “Did a doctor ever tell you that some experts disagree about whether men should have PSA tests?” Scientific uncertainty is not the only uncertainty pertaining to medical interventions,34 and expert disagreement is not the only manifestation of scientific uncertainty. Scientific uncertainty, however, is central to the controversy surrounding PSA screening,12,13,16,20,23,25,35 and expert disagreement is a final manifestation of this uncertainty. Questions used yes or no response categories and were asked of all respondents including nonscreened men (for screened men, questions were preceded by the phrase, “Before you had the PSA test…”). All questions underwent 2 rounds of cognitive testing and modification by expert staff. We used responses to the advantages, disadvantages, and uncertainty items to create a composite variable, extent of shared decision making, with 5 categories ranging from no elements to all elements, reflecting the discrete information elements discussed by physicians.
Sociodemographic and Health-Related Variables
The analysis included sociodemographic and health-related factors examined in previous studies18,19,36–41: health insurance, presence of usual source of medical care, family history of prostate cancer, self-reported health status, number of chronic diseases. Physician recommendation for PSA screening was measured by the question, “Has a doctor ever recommended that you have a PSA test?”
PSA Screening Intensity
To assess PSA screening intensity, we created a 3-level variable from an item asking men whether they ever had a PSA test; those who answered no constituted the lowest intensity category (none). Remaining men were stratified into low- and high-intensity categories based on the total self-reported number of PSA tests in the past 5 years: men reporting 1 to 3 tests were categorized as low intensity (less than annual), men reporting 4 to 5 tests were categorized as high intensity (approximately annual). This approach underestimates high-intensity screening in younger men who may not have undergone 4 to 5 tests even if screened annually. Additional analysis including men aged 40 to 49 years, however, resulted in no significant differences in the proportions of men in the 3 intensity categories.
Data Analysis
We calculated descriptive statistics of the study population’s characteristics, prevalence of shared decision making, and PSA screening intensity. We fit separate multivariable polytomous and binary logistic regression models, adjusting for all sociodemographic and health-related characteristics, for the following dependent variables: (1) PSA screening intensity, (2) discussion of advantages and disadvantages, and (3) discussion of uncertainty. For the first model, we included extent of shared decision making as an independent variable. For the second and third models, examining predictors of shared decision making, discussion of uncertainty, and discussion of advantages and disadvantages, respectively, were included as independent variables to examine associations of different shared decision-making elements with one another. We used the Wald χ2 test to assess statistical significance, using a stringent cutoff (P <.01) to minimize type I error from our large sample size. We used SUDAAN 9.0.1 (RTI International) to adjust for the survey’s complex sampling design, using weights provided with the NHIS data file to account for selection probability and nonresponse and to provide estimates representative of the US population.
RESULTS
For the 2010 NHIS, interviews were conducted with 27,157 adults (response rate 60.8%). Of 4,217 men aged 50 to 74 years, 3,427 met eligibility criteria and were included in the study population (Figure 1). Study population characteristics are shown in Table 1. Approximately 55.8% of men reported ever having a PSA test, and 65.5% of them had testing within the past year. Physician recommendation for PSA screening was reported by 52.5%. No past screening was reported by 44.2%, low-intensity screening by 27.8%, high-intensity screening by 25.1%.

Study population of men aged 50–74 years, National Health Interview Survey, 2010.
Characteristics of Study Population (N = 3,427), 2010 National Health Interview Survey
Table 2 shows the independent and joint distribution of shared decision-making elements. No physician-patient discussion of either advantages or disadvantages was reported by 65.1% of men, whereas discussion of advantages only was reported by 16.9%, disadvantages only by 0.9%, advantages and disadvantages by 17.0%, and uncertainty by 12.1%. Only 8.0% reported discussion of all 3 elements (full shared decision making). Partial shared decision making (1 to 2 discussion elements) was reported by 27.8%, ranging from 2.5% for disadvantages only to 14.6% for advantages only.
Prevalence of Elements of Shared Decision Making in PSA Screening Study Population (N=3,427), 2010 National Health Interview Survey
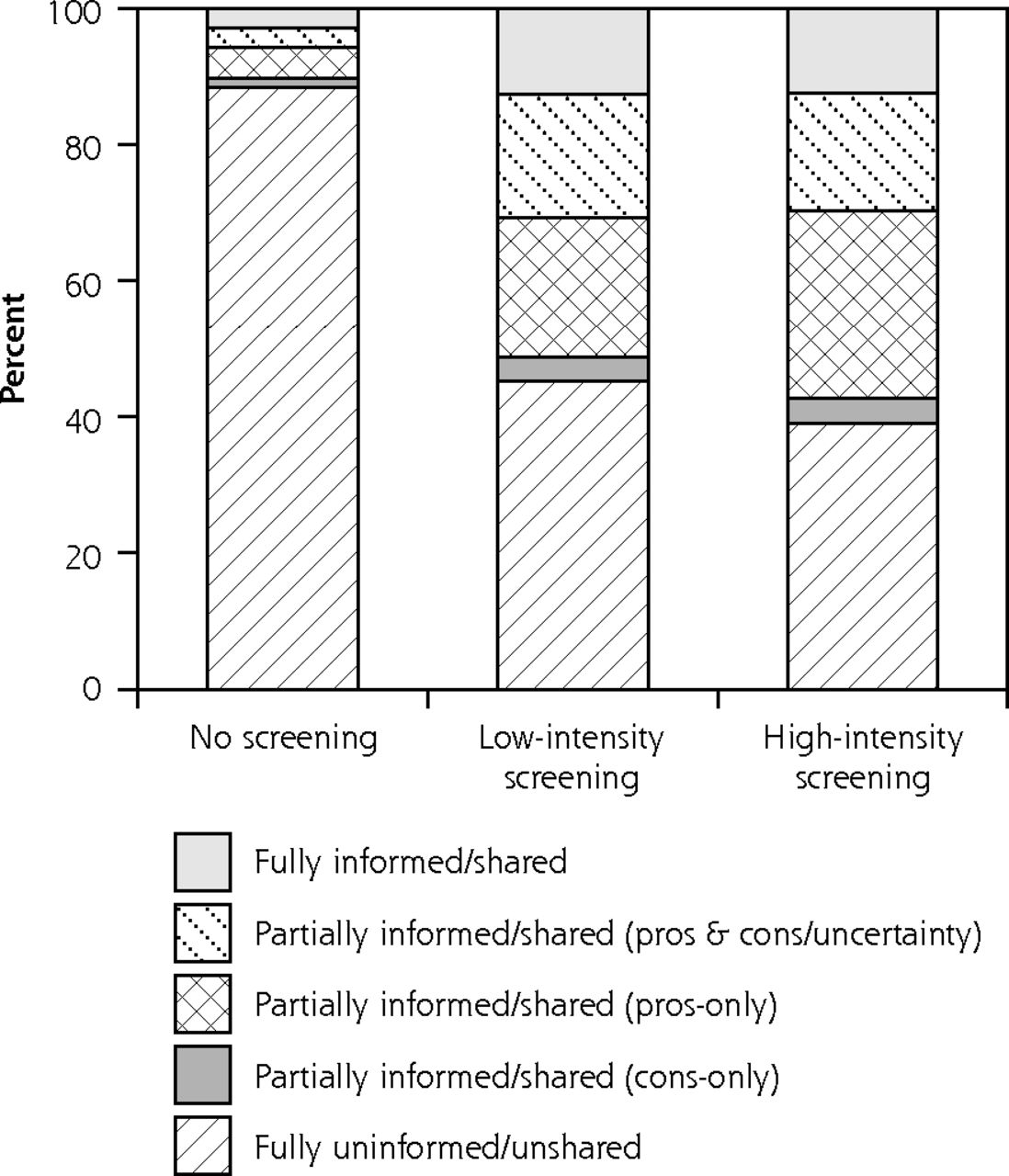
Table 3 shows the factors associated with PSA screening intensity in adjusted analyses (unadjusted analyses are in Supplemental Table 1, available at http://annfammed.org/content/11/4/306/suppl/DC1). Increasing age, higher education, usual source of medical care, and physician recommendation were associated with higher intensity screening. Partial shared decision making (1 to 2 discussion elements) was associated with higher intensity screening (compared with no shared decision making), but full shared decision making (all 3 discussion elements) was not. Figure 2 displays these data in terms of unadjusted column percentages, showing the extent of shared decision making in the nonscreening, low-intensity, and high-intensity screening groups. Of nonscreened men, 88% (95% CI, 86.2%–90.1%) reported no shared decision-making elements and 3% (95% CI, 2.0%–4.2%) reported all 3; corresponding proportions for men undergoing high-intensity screening were 39% (95% CI, 35.0%–43.3%) and 13% (95% CI, 9.9%–15.6%).
Factors Associated with PSA Screening Intensity,a 2010 National Health Interview Survey
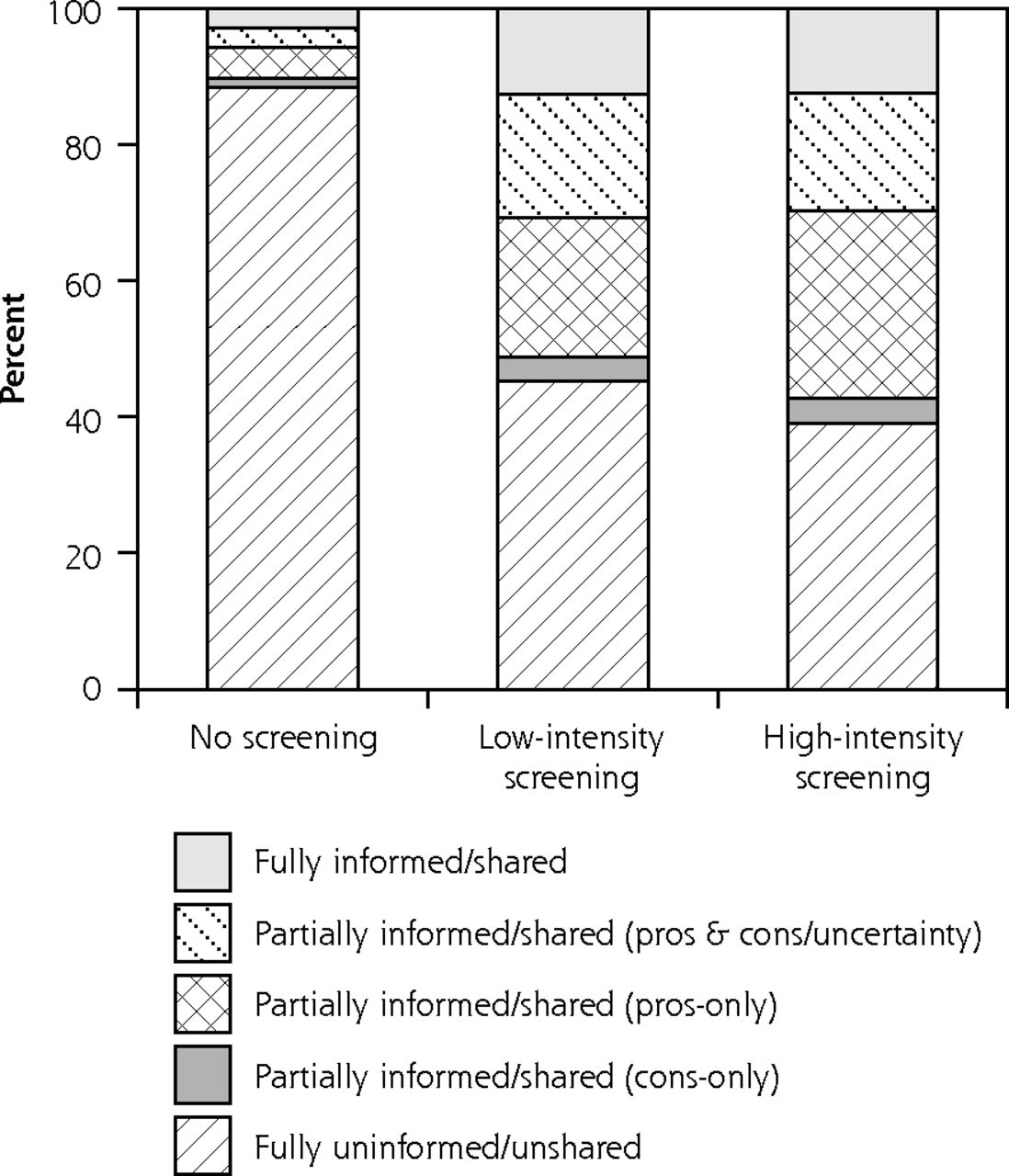
Extent of shared decision making by intensity level of PSA screening, 2010 National Health Interview Survey
PSA=prostate-specific antigen.
Notes: Extent of shared decision making (unadjusted percentages) according to the physician’s discussion of the following elements: advantages, disadvantages, and uncertainty. Fully informed is discussion of all elements. Partially informed/shared (pros+cons/uncertainty) is discussion of advantages and disadvantages or advantages and uncertainty. Partially informed/shared (pros-only) is discussion of advantages only. Partially informed/shared (cons-only) is discussion of disadvantages only, disadvantages and uncertainty, or uncertainty only. Fully uninformed/unshared is no discussion of decision-making elements. PSA screening intensity levels are as follows: no screening = no past history; low-intensity = 1–3 tests in past 5 years; high-intensity = 4–5 tests in past 5 years.
With respect to predictors of shared decision making, 4 factors were positively associated with physician-patient discussions of advantages and disadvantages (Table 4): black race, Hispanic ethnicity, physician recommendation, and discussion of uncertainty. Two factors—higher education, discussion of advantages and disadvantages—were positively associated with discussion of uncertainty, whereas no or only public health insurance was negatively associated.
Factors Associated with Physician-Patient Discussion of Advantages and Disadvantages of PSA Screening and Uncertainty About PSA Screening, 2010 National Health Interview Survey
DISCUSSION
The current study adds to mounting evidence that shared decision making is an uncommon occurrence in PSA screening.18,19,21,41 Most PSA screening occurs with incomplete or no physician-patient discussion of its associated advantages, disadvantages, and uncertainty. These elements of shared decision making occur at different rates and are associated with different factors, suggesting variation in specific shared decision-making practices for individual patients. The communication of scientific uncertainty is especially infrequent and represents an important target for future shared decision making efforts.
The most significant study finding was that the absence of shared decision making applies not only to PSA screening but also to nonscreening. Because it included—for the first time in a national survey—both screened and nonscreened men, our study was able to show that the relative population prevalence of physician-uninformed nonscreening (screening nonuptake24 in the absence of shared decision making) exceeds that of physician-uninformed screening (both low- and high-intensity combined)—corresponding to annual US population-weighted totals of 12,141,033 vs 6,393,735 men, respectively. This difference may be partly inflated by screening received unknowingly by some men,2–6 but its sheer magnitude is difficult to attribute to underreported testing alone.
These findings provide empirical justification for a broader focus in the current policy debate about PSA screening. Much of this debate has focused on PSA screening in the absence of shared decision making and its potential harm of undesired, unnecessary treatment of screening-detected cancer. Our study, however, suggests that the more prevalent problem is nonscreening in the absence of shared decision making—the harm of which is the failure to allow individuals to decide for themselves if screening is beneficial. The importance of this problem is disputable, as shown by ongoing debate over the revised USPSTF guidelines.249,20,26 Physicians have no ethical obligation to discuss or offer nonbeneficial interventions. If, however, the benefits of PSA screening remain disputable based on available evidence—as guidelines in 2010 affirmed and many experts continue to believe25,27—then nonscreening in the absence of shared decision making is problematic.
Our study also provides new evidence of the potential effects of shared decision making on screening. PSA screening is common and associated with several factors, including physician recommendation, older age, higher education, and having a usual source of medical care. These findings reinforce concerns that PSA screening is often undertaken in men less likely to benefit from it and driven in part by access to health care.18,19 We showed that screening intensity is associated with shared decision making; it is greater with partial than with full or absent shared decision making (Table 3). This finding is partly consistent with past evidence. Clinical trials have shown that decision support reduces uptake of PSA screening,42–45 consistent with our finding that men who reported being fully informed about advantages, disadvantages, and uncertainty had a lower likelihood of undergoing high-intensity screening. The association between greater screening and discussion of advantages only was also observed in the national DECISIONS survey.19 This association was nonsignificant—likely reflecting power limitations that were due to the DECISIONS study’s smaller sample size (N = 375)—but has face validity, suggesting a biasing effect of physician-patient discussions limited to screening advantages.
More difficult to explain is our finding of higher screening intensity even in partial shared decision-making discussions limited to screening disadvantages (Table 3). One explanation is that PSA screening discussions are influenced by factors other than their content—eg, the timing or manner in which these discussions are conducted. For example, physicians may communicate screening disadvantages in a manner that downplays their importance. The very discussion of screening by a physician may also convey a promise of benefit, ie, an implicit recommendation for screening.46–51 Alternatively, patients may demand PSA screening or have positive preconceptions that may make them disregard information about its disadvantages or resist physicians’ attempts to discourage screening. Other unmeasured patient factors, eg, physician-patient racial and sex concordance, may also influence screening discussions.52,53 More research is needed to test these and other explanations and to determine how the process of communication about PSA screening, as well as its content, influences decision making. In any case, our findings suggest that this communication process could be improved.
Our study has several limitations. Its reliance on self-report and focus on the occurrence of screening discussions anytime in the past, rather than within a recent time frame, introduces measurement error from recall problems. Our approach, however, has the advantage of maximizing sensitivity for detecting shared decision making that may have occurred in the more distant past and led to subsequent screening refusal, as well as for detecting the absence of shared decision making in nonscreened men. Another limitation is our operationalization of shared decision making in terms of only 3 necessary—but not sufficient—content elements of physician-patient discussions. We did not measure such process elements as elicitation of patient preferences.30–32 More stringent criteria requiring the joint presence of all these elements would have produced even lower estimates of the prevalence of shared decision making. Further research is needed to develop feasible measures of shared decision making for population surveillance.
Other limitations of our study include its cross-sectional design, inability to rule out PSA testing conducted for diagnostic purposes, and use of patient self-report to ascertain both shared decision making and PSA screening. Patient perceptions of care may diverge from actual care; nevertheless, patient perceptions are important outcomes that reflect health care quality and predict behavior.54 Yet self-reported screening can be inaccurate55 and biased toward under-ascertainment2–6; our exclusion of men reporting more than 5 tests in 5 years may have exacerbated this bias. More research using direct ascertainment of actual screening is needed.
Finally, we did not measure men’s knowledge about PSA screening or assess whether informed decision making occurred independently of physicians and clinical encounters. This research gap is critical, because numerous barriers make shared decision making about PSA screening challenging to achieve. Barriers include the large number of screening-eligible men, the indisputably limited clinical time available for patient counseling, and the multiplicity and complexity of screening-related uncertainties.20 In the face of these barriers, attempts at shared decision making may not improve clinical outcomes, and the more practical approach may be to provide information about PSA screening apart from the clinical encounters, eg, through community-based screening programs or by means of decision aids delivered by nonphysician personnel.16 Accordingly, the more important outcome may be informed decision making rather than shared decision making.
Despite these limitations, our study provides important new evidence on the prevalence, nature, and potential influence of shared decision making in PSA screening. Shared decision making occurs infrequently, and its absence applies not only to screening but to nonscreening. Essential elements of shared decision making—physician-patient discussions of the advantages, disadvantages, and uncertainty associated with PSA screening—are associated with screening intensity. Further work is needed to confirm these findings, to develop valid, feasible measures of informed and shared decision making for population surveillance, and to improve shared decision making in decisions both for and against PSA screening.
Acknowledgments
We thank Richard Lee and Tim McNeel, Information Management Services, Inc, for programming and data analytic support, and Rachel Ballard-Barbash and Martin Brown for helpful comments on an earlier version of the manuscript.
Footnotes
-
Conflicts of interest: authors report none.
-
Author contributions: Dr Han had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
-
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Cancer Institute or the Centers for Disease Control and Prevention.
- Received for publication October 6, 2012.
- Revision received January 18, 2013.
- Accepted for publication February 5, 2013.
- © 2013 Annals of Family Medicine, Inc.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transcriptome-Wide Association Analysis Identifies Novel Candidate Susceptibility Genes for Prostate-Specific Antigen Levels in Men Without Prostate Cancer
- Diagnosing prostate cancer in asymptomatic patients
- Effect of a Prostate Cancer Screening Decision Aid for African-American Men in Primary Care Settings
- Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis
- Prostate-Specific Antigen Testing Initiation and Shared Decision-Making: Findings from the 2000 and 2015 National Health Interview Surveys
- Recent Patterns in Shared Decision Making for Prostate-Specific Antigen Testing in the United States
- Updated Review of Prevalence of Major Risk Factors and Use of Screening Tests for Cancer in the United States
- In This Issue: A Diversified Portfolio
- Shared Decision Making, Contextualized