
Abstract
PURPOSE We evaluated a peer leader–support program (PLSP) for diabetes self-management in China in terms of acceptability and feasibility; implementation; perceived advantages; disadvantages and barriers; reach and recruitment; effectiveness in terms of diabetes knowledge and clinical impacts; adoption; and sustainability.
METHODS Within each of 3 cities in Anhui Province, 2 subcommunities were randomly assigned to usual care or PLSP. Peer leaders and staff of Community Health Service Centers (CHSCs) co-led biweekly educational meetings. Peer leaders also led biweekly discussion meetings, promoted regular care through the CHSCs, organized informal health promotion activities (eg, walking and tai chi groups), and provided informal individual support to participants through casual contact.
RESULTS Qualitative evaluations indicated acceptance of and positive responses to the program among patients, peer leaders, and CHSC staff. Implementation was successful in 2 of 3 subcommunities, the third failing for lack of staff resources. Reported advantages included peer support as a bridge between CHSCs and their patients. In 2 sites where the PLSP was implemented, analyses controlling for baseline differences and site showed significant benefits for PLSP relative to controls (P <0.05) for knowledge, self-efficacy, BMI, systolic blood pressure, diastolic blood pressure, and both fasting and 2-hour post-prandial blood glucose. The Anhui Provincial Health Bureau has extended the PLSP model to other communities and to cardiovascular disease prevention and management.
CONCLUSION The PLSP was well accepted, feasible given sufficient administrative and staff resources, effective for those who participated, and generalizable to other sites and health problems.
INTRODUCTION
The prevalence of diabetes mellitus among Chinese adults was 11.6% in 2010, or 113.9 million, and the prevalence of prediabetes was 50.1%, or 493.4 million.1,2 Two-thirds of Chinese adults with diabetes have complications3 and only 11.5% exhibit satisfactory glycemic control.4 The Chinese health system, like many others,5 tends to emphasize clinical care but until recently has placed little emphasis on patient education.
A recent review of peer-support interventions documented contributions to basic health needs (eg, reducing childhood undernutrition), to primary care and health promotion, and to chronic disease management.6 Peer support can improve diabetes management7–12 but has not been adopted appreciably in China. An exception is a recent report of telephone peer support provided by a diabetes specialty service for patients of primary care physicians in Hong Kong.11 Peer support implemented through primary care is also a topic of growing interest.13–15
Our research project examined a peer-support intervention for type 2 diabetes in primary care community health services centers (CHSCs) in Anhui Province. Following models for implementation and dissemination research,16–18 it included initial formative evaluation of acceptability and feasibility and, at the end of the study period, assessment of advantages, disadvantages, barriers, reach, recruitment, effectiveness (within an evaluation subsample), and program sustainability and adoption.
METHODS
Setting
The Community Chronic Disease Management System provides population-wide primary care through CHSCs and their community health service stations (CHSSs). The government provides ¥25/person/year (in 2009–2010, approximately US$3.50) to CHSCs to deliver a defined package of 11 basic public health services. For diabetes, these include a yearly clinical assessment; quarterly blood sugar assessment; health education addressing healthy diet, physical activity, and medication adherence; and routine home follow-up visits. Traditionally, the CHSCs provide health education mainly through leaflets and brochures for patients with diabetes or through diabetes education presentations in community locations. These activities are coordinated through the Anhui Provincial Center for Disease Control and Prevention (CDC). Against this backdrop, the Peer Leader Support Program (PLSP) was implemented in 3 cities in Anhui.
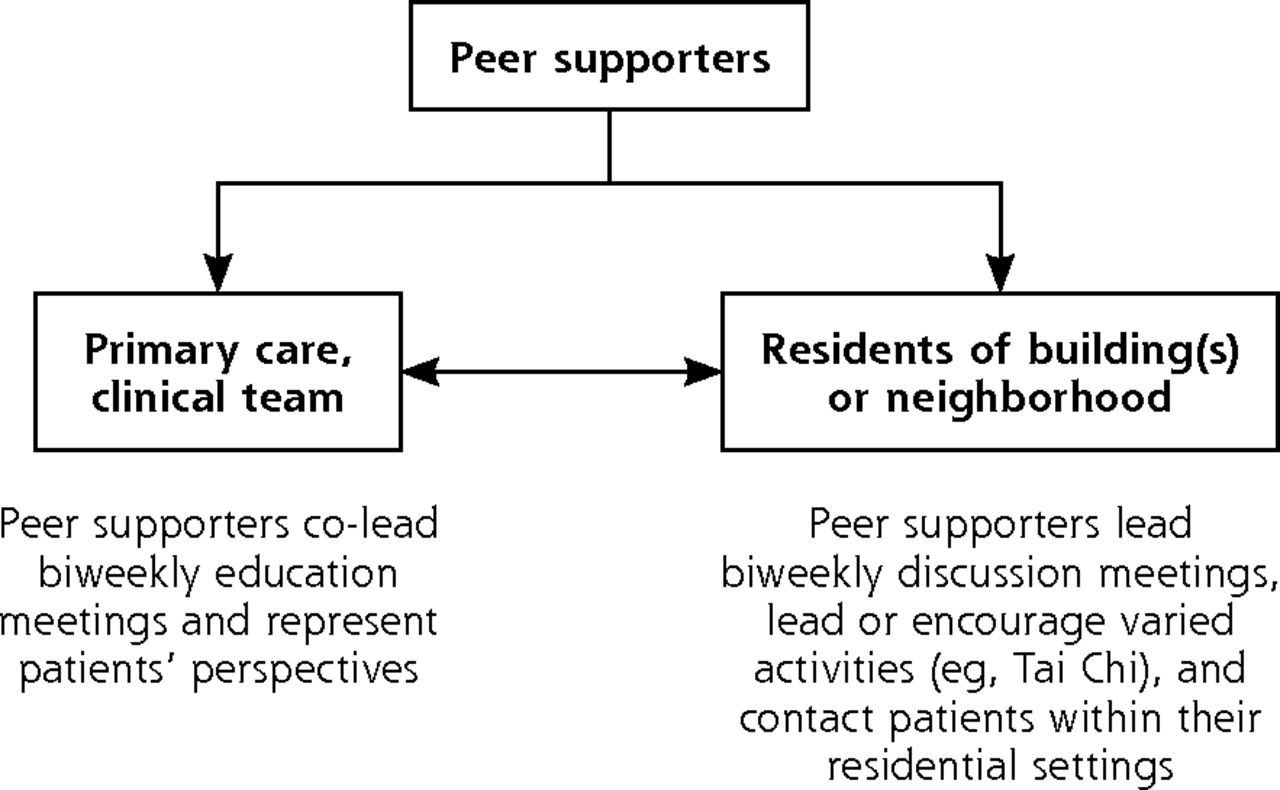
An important feature of the setting was its integration of primary care with communities. Each community is subdivided into subcommunities, each with its own community-neighborhood committee and each served by its own CHSS. Individuals in a particular housing site receive their care through a clinical team assigned to that site. Figure 1, for example, shows the director of a CHSC pointing to a sign in the entrance of a residence indicating the names and telephone contact of the clinical team serving that building. Where the PLSP is implemented, peer leaders receive care through the same team as those with whom they live. Thus, as in Figure 2, peer leaders, their neighbors, and their clinical service team are connected so as to facilitate coherence of clinical care, peer support, and community activity.

Community health center director pointing to a sign in a residence entryway that indicates the names and contact information for clinical team that serves residents of the building.

Relationships among peer leaders, clinical teams, and community residents in the Peer Leader Support Program.
Ethical approval for this study was obtained from the Ethics Committee for Human Research, Faculty of Public Health, Mahidol University (Proof Number: MUPH 2010-079).
Selection of Communities
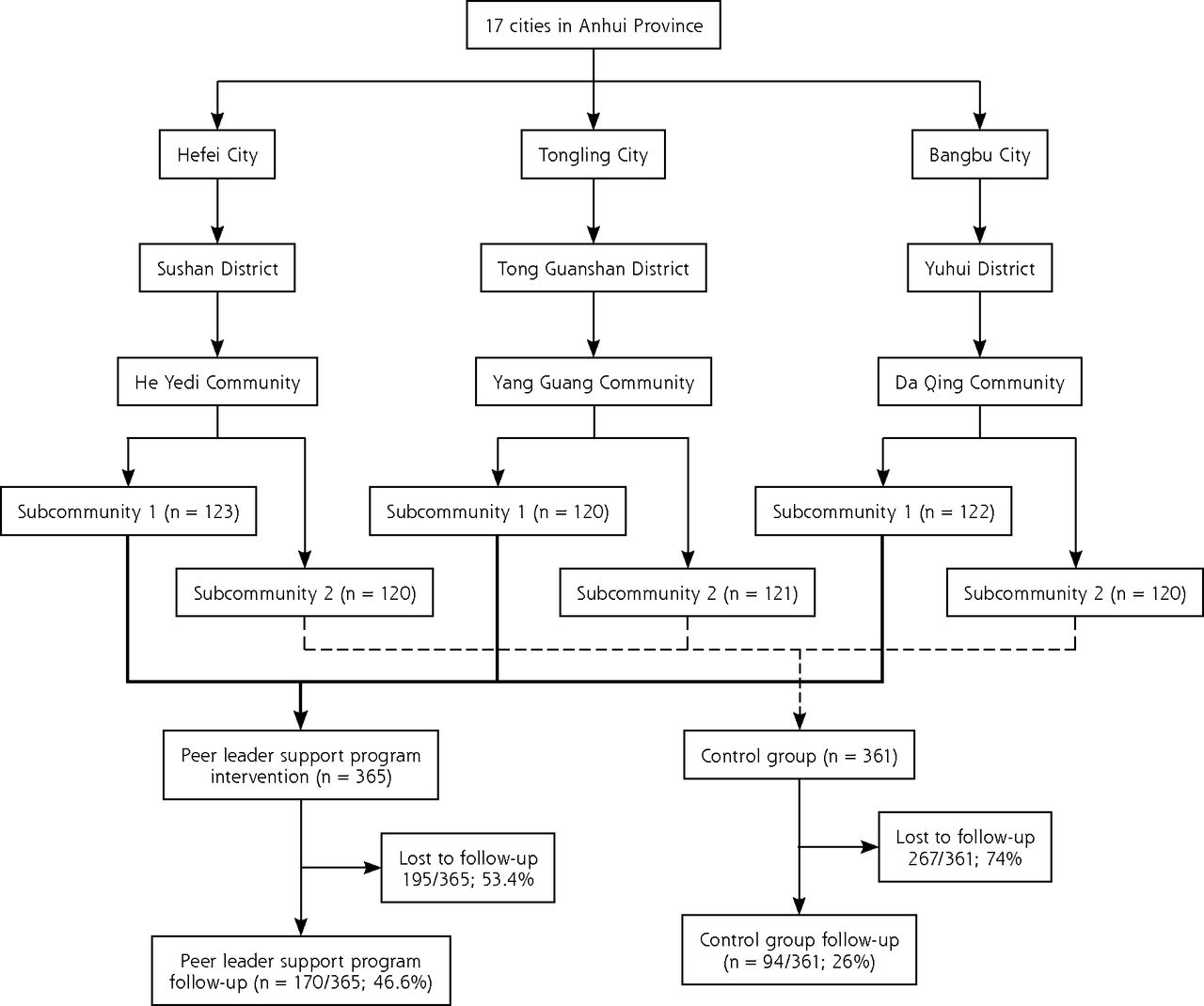
Stratified sampling was used to select 1 city randomly in each of the northern, southern, and middle regions of Anhui. A district was then selected within each city and, within each district, 1 community of about 20,000 residents was randomly selected (Figure 3). These were the Yang Guang Community of Tonglin, the Da Qin Community of Bangbu, and the He Ye-di Community of Hefei. Two subcommunities with similar characteristics in terms of demographics, customs, and social norms were randomly chosen from each community. The 2 chosen subcommunities, each served by its own CHSS, were then randomly assigned to intervention and control conditions.

Recruitment and retention of study sites and participants.
Formative Evaluation
Formative evaluation addressed the feasibility, adaptability, and acceptability of the program and its key features relative to community and organization policy. It was also intended to engage and empower local communities to be part of program development. Focus groups were held in 2 communities and individual interviews in all 3 communities. The interviews included the leaders of each of the 6 CHSSs, 2 in each community, that had agreed to participate in the study, along with the leader of the district health bureau and the leader of the neighborhood committee associated with each of the 6 CHSSs.
Each focus group was conducted by 2 research team members. A third team member checked their notes for accuracy against audiotapes of the group meetings and participated in analysis. Content analyses identified the common concepts across sites and across roles. Response patterns and themes were similar for the 2 focus groups, so further groups were not pursued. Similar methods were used to evaluate implementation at the end of the study, also including interviews with patients and peer supporters.
Implementation of the Peer Leader Support Program
The formative evaluation indicated substantial support for the PLSP model and for a systematic study of its effectiveness. Therefore, the program was not altered before implementation.
Peer Leader Selection and Training
CHSC staff recruited 19 peer leaders who had been diagnosed with type 2 diabetes for more than 1 year, were willing to volunteer, and generally adhered to both medication and behavioral management regimens. Additional criteria were altruism, positive and sociable personality, availability of time, an understanding of the importance of patient confidentiality, good relationships with community residents, and leadership in their communities. Further selection was based on willingness to liaise with CHSC staff in response to unanticipated problems, to commit to the project schedule, to take on the responsibilities of peer leaders and adhere to program policies, to attend 3 days’ training, and to contact group members frequently. Peer leaders were retired adults who had had diabetes for a mean of 9.3 years. Although some were nonprofessionals, a number had work experience in teaching, nursing, or the like. Sixteen of 19 were male (84.2%).
The Anhui CDC research team provided 3 days’ training for the peer leaders, including an introduction to the PLSP and training in basic skills and diabetes self-management. Training emphasized the key functions of peer support promoted by Peers for Progress:19,20
Assisting and encouraging daily diabetes management
Providing social and emotional support
Linking with community resources and primary care at the CHSSs
Providing ongoing support
Peer leaders were told how to seek support from their CHSS staff, CDC professionals, and tertiary hospital specialists if needed. They also met with each other bimonthly to share their experiences and exchange lessons. A peer leader handbook included materials for use with participants. CHSC staff also received training in the PLSP.
PLSP Meetings and Activities
Nineteen “peer support groups,” 1 for each peer leader, were set up in the subcommunities randomized to the PLSP condition. Each group consisted of 10–15 participants. The protocol called for twelve biweekly education meetings over 6 months to be co-led by peer leaders with CHSC staff involvement titrated to peer leaders’ needs. Meetings lasted 1.5 to 2 hours and covered a range of topics such as diet, physical activity, medications, foot care, stress management and depression, barriers to self-management, and obtaining resources and support from the community, family, friends, and the health system. For efficiency, groups were often combined, resulting in meetings of more than 30 participants and consequently limited opportunity for discussion. Accordingly, the protocol also called for peer leaders to lead 12 biweekly discussion meetings over 6 months. These reviewed the topics of the education meetings and included sharing experiences and modeling self-management practices.
Peer leaders also led or encouraged informal activities (for instance, walking and tai chi groups) among group members. Because peer leaders and participants lived within the same subcommunities, casual interactions and activities were common.
Recruitment
Participants were identified through a Community Chronic Disease Management System in each CHSC. We used the following inclusion criteria: (1) a diagnosis of type 2 diabetes made at a hospital, based on WHO criteria21; (2) age at least 15 years; (3) residence in 1 of the project communities for more than 1 year. Exclusion criteria included inability to participate due to physical or mental disabilities.
CHSC staff contacted eligible patients by phone to explain the purpose of the study and details of the PLSP. Those providing consent were invited to visit their CHSS to provide baseline self-report and biophysical data. Generally, CHSS staff conducted face-to-face interviews for self-reported data because most participants had little education or were illiterate. Some interviews were also conducted by staff in participants’ homes.
Evaluation
Implementation was monitored through research team records and work report forms of the CHSCs. Perceived advantages, disadvantages, and barriers to implementation were assessed through focus groups and interviews with community and clinic leaders, peer supporters, and patients at the conclusion of the PLSP. Assessment of sustainability and adoption was based on research team and CHSC records and reports.
Effectiveness
After community needs assessments and participant recruitment in the 6 subcommunities, baseline collection of clinical and self-report data took place over a 6-month period, from June to December, 2009. The intervention ran from January to July, 2010. Due to a public health emergency between August and October, follow-up data collection was delayed to October through December, 2010.
Evaluation included measures of diabetes knowledge, self-management practices, attitudes toward self-management, self-efficacy, and social support, as detailed in Supplemental Appendix 1 (http://annfammed.org/content/13/Suppl_1/S50/suppl/DC1). The measures were developed for this study. They were pilot tested in a subset of 35 adults with diabetes recruited from a CHSC outside the study communities. Internal consistency (Cronbach’s α) was 0.877 for diabetes knowledge, 0.815 for self-management practices, 0.842 for attitudes, 0.861 for self-efficacy, and 0.811 for social support.
Statistical Analysis
Analyses compared sites at baseline as well as participants who completed and did not complete follow up. Because patients received services from several peer leaders in each community, analyses did not include nesting of patients within peer leaders. Evaluation of outcomes controlled for site, age, education, income, and sex. With the sample size of 135 PLSP participants completing baseline and follow-up assessments (explained below), power was 0.77 (2-sided, α = .05) to detect a difference in fasting blood sugar of 0.5 mmol/L (9.01 mg/dL) between baseline and follow-up. Analysis was performed with SPSS, Version 19 (IBM) using the general linear model procedure (GLM).
RESULTS
Acceptability and Feasibility
As detailed in Table 1, key representatives from local Community Neighborhood Committees indicated that PLSP would be acceptable and feasible for their neighborhoods. Responses of CHSC directors, staff, and patients were also positive and included expressions of desire for “more training and direction” along with some concern among staff that “…the program may bring a large work burden for us.” Accordingly, health authorities in the 3 cities agreed to provide policy, technical, and modest financial support to the PLSP.
Observations from Participants, Peer Leaders, and Clinical Staff and Administrators Regarding Acceptability and Feasibility of the Peer Leader Support Program (PLSP)
Implementation
Table 2 includes, for each subcommunity, the average numbers of educational and discussion meetings held as well as the numbers of participants enrolled and participating. With only 1 CHSC staff member assigned to manage the program and co-lead group meetings, implementation in community 3 did not achieve protocol objectives. Only 3 peer leaders were recruited and only 3 peer groups of 10 to 15 participants were organized. As a result, most participants from community 3 did not have the opportunity to attend group meeting and activities.
Average Numbers of Key Meetings and Activities and of Participants in Each PLSP Subcommunity
Reach and Recruitment
Women made up 49% of participants at baseline, with no difference by community or intervention. GLM analyses evaluated differences in baseline characteristics by condition (PLSP vs control), community (1, 2 and 3), and the interactions between condition and community. (Supplemental Appendix 1 at http://annfammed.org/content/13/Suppl_1/S50/suppl/DC1.) We found a significant interaction between communities and condition (PLSP vs control) for age and significant differences by condition for education and income. Accordingly, age, education, and income were included as control variables in all statistical evaluations.
Figure 3 shows the flow of 726 participants through the study, 365 in the intervention and 361 in the control subcommunities. Because of the CHSCs’ responsibilities to their communities, PLSP was open to all individuals with diabetes, a number of whom began participating after the program began. As a result, 726 individuals completed baseline survey and 533 completed follow-up surveys. Reasons for loss to follow-up included moving away, ceasing to participate in the program and its evaluation because of lack of time or health problems that interfered, and loss of interest.
Of the 365 individuals in the PLSP study population, 279 (76.4%) attended at least 6 meetings and activities. One hundred and seventy completed both baseline and follow-up and attended 10 or more meetings or group activities. Among controls, 94 completed baseline and follow-up.
Because of the poor implementation in community 3 and its failure to recruit any participants for follow-up in its control subcommunity, it was dropped from further analyses. This resulted in a total of 135 PLSP and 94 control participants from communities 1 and 2 who completed follow-up and were therefore included in the evaluation of changes in study variables. Among those completing follow-up, 41% were women, in comparison to 55.3% of those not completing (P = .002).
Supplemental Appendix 2 compares those completing and not completing follow up on other study variables among PLSP and control sites. Within the PLSP, those who completed follow-up had greater education, greater diabetes knowledge, more positive attitudes toward self-management, and greater BMI. There were several significant interactions between condition and community. While those in PLSP who completed follow-up had greater diabetes knowledge, control participants who completed follow-up had less. Also, those in PLSP who completed follow-up were more likely to report glucose monitoring, but control participants were less likely to do so. Control participants who completed follow-up had lower BMI in contrast to the greater BMI noted above for PLSP participants who completed follow-up. In summary, then, sex, age, education, and income were included as control variables in subsequent analyses of effectiveness. Knowledge of diabetes, attitudes toward self management, and BMI were not included as control variables because they were included as outcomes.
Effectiveness
Table 3 includes baseline and follow-up measures of diabetes knowledge, attitudes, self-management behaviors, and clinical outcomes for the PLSP and control participants who completed follow-up in Communities 1 and 2, controlling for sex, age, education, income, and community. Significant interactions between condition and time lapse from baseline to follow-up indicated greater favorable changes for PLSP participants for diabetes knowledge, self-efficacy, BMI, systolic and diastolic blood pressure, fasting glucose, and 2-hour post-prandial glucose. For example, PLSP participants showed a reduction in fasting glucose levels from 7.68 mmol/L to 6.76 mmol/L (138 mg/dL to 121 mg/dL) while those in the control communities showed a slight increase from 6.38 mmol/L to 6.66 mmol/L (115 mg/dL to 120 mg/dL). The difference between these 2 patterns was highly significant (P <.001).
Changes in Outcome Variables Comparing PLSP and Control Participants Who Completed Follow-up
Perceived Advantages, Disadvantages, and Barriers to Implementation
Qualitative evaluation with CHSC staff, peer supporters, and patients at the conclusion of PLSP identified barriers to and facilitators of implementation; these are detailed in Table 4. Barriers ranged from staff and financial resources within the CHSSs to inconvenient meeting times.
Observations of Participants, Peer Leaders, and Clinical Staff and Administrators Regarding Implementation and Emergent Features of the Peer Leader Support Program (PLSP)
Most peer leaders believed that the PLSP benefited both the patients in their groups and themselves, viewed the PLSP as important, were happy with their work, and said they would like to remain peer leaders. Facilitating factors included assistance peer leaders reported receiving from CHSC staff, skills staff reported learning through the program, and 1 CHSC director’s opinion that the PLSP improved provision of care. Staff also advocated greater duration of the PLSP. Participants noted no negative aspects of the PLSP but noted the value of both practical, specific assistance and emotional support it provided.
Sustainability/Adoption
Based on these findings, the Anhui Provincial Health Bureau has expanded PLSP to other communities in the province and to cardiovascular disease prevention and management. This has been facilitated by national health reform, which has enabled the assignment of additional staff to disease management and prevention so that programs like PLSP can become part of routine work, not extra work.
DISCUSSION
To our knowledge, no previous research has examined the feasibility, acceptance, and benefits of peer support for diabetes management based in community primary care in China. The PLSP proved well accepted and feasible if it is provided administrative support and staff resources. It was effective in improving diabetes knowledge and clinical outcomes for those who attended peer-support groups. Peer-led meetings and activities encouraged supportive networks among group members in their familiar neighborhoods in a way compatible with Chinese culture. The Anhui Provincial Health Bureau’s extension of PLSP to other settings and health problems attests to its promise as a broad strategy for improving chronic disease care and prevention.
Group activities are traditional in Chinese culture, especially for older adults. This may have enhanced participation in the informal groups based on shared interests—a jogging group, for example. Additionally, residents living in the same neighborhood are familiar with each other and generally help each other. Also of note, all peer leaders and most participants were older adults (average age 63 ± 9.41 years), and retired (62.8%) providing time to attend group meetings and activities. Practical, specific support from the PLSP may have contributed to participants’ increased self-efficacy.24
Success of the PLSP for diabetes and its extension to prevention and management of cardiovascular and other diseases also benefitted from recent policies of the national government encouraging the primary care CHSCs to serve as “health gatekeepers” and to manage referrals to specialist care and hospitals.25 This includes the government’s providing ¥25/person/year to CHSCs for implementing 11 primary care and preventive packages.
Emotional support emerged as a benefit of the PLSP. With cultural emphases on harmony and the interests of the family, relatives are obligated to support each other but, at the same time, reluctant to place a burden on their families.26 The PLSP apparently provided a setting in which individuals could discuss feelings without fear of obligating others.
Several aspects of the roles of peer leaders deserve attention. Co-leading educational meetings with CHSS staff might be thought to compromise the “peerness” of the peer leaders. They reported, however, that they valued not having to worry about making mistakes, but being able to focus on their roles as peers and the activities they promoted. This reflected a view of their role as distinct from and complementary to health professionals, not as “junior doctors.”
Peer leaders reported good working relationships with CHSS staff, providing feedback to CHSS staff about group members’ needs, questions raised, and needs for specialty referrals. Participants valued the peer leaders as “our” representative who could express “our” needs and requirements to CHSCs and tertiary hospital specialists. In this, peer leaders may offer a valued counterforce to the otherwise hierarchical nature of medical care. The PLSP also embodied community participation strategies needed for chronic disease prevention and control in the daily lives of individuals.27,28 This was valued by CHSC directors, 1 of whom noted that peer leaders may serve as “the bridge to link our CHSC with patients in their served neighborhood.” This reflects broader discussion of contributions of peer support to primary care.13–15
Men comprised 84% of peer leaders. Most women invited to become peer leaders felt that, although they were retired, housework and looking after grandchildren prevented their commitment to group meetings and activities. Also, most women in the generation sampled have lower education levels than their male counterparts.
Variability in implementation underscores the importance of organizational support to program implementation, issues just beginning to be studied in peer support.15 The limited implementation in Community 3 also reflects transitions in which hospitals have become CHSCs but, in so doing, have needed new income sources. At the time of the study, the Community 3 CHSC focused on clinical income and also lacked public health professionals and experience, limiting its PLSP implementation. These transitions are now generally completed and the associated limitations less common. That some peer-leader activities varied from group to group (especially informal activities not specified in the protocol) raises issues concerning standardization and our achievement of treatment fidelity. The PLSP addressed this through standardization not around specific activities but around key functions of peer support (assistance in daily management, social and emotional support, linkage to clinical care and community resources, and ongoing availability of support).20,29
Limitations
Within this dissemination and implementation study, threats to validity and potential sources of bias included randomization of communities before collection of baseline data, collection of outcome data by community nurses not blinded to community allocation, conduct of focus groups and structured interviews by research staff, failure of analyses to include duration of diabetes and some measure of complications, and substantial numbers lost to follow-up.
Initiation of the PLSP may have motivated CHSC staff to provide better diabetes care. Monitoring of prescribing practices, however, did not indicate differences in delivery of routine diabetes care between intervention and control subcommunities.
The present results are consistent with other reports of benefits of peer support in diabetes management.7–12 Interestingly, the study of telephone peer support in Hong Kong11 failed to achieve incremental clinical benefit when added to comprehensive care that included coordination through a registry, initial patient education, and initial appraisals, quarterly reports and algorithm-based recommendations for care to patients and clinicians.30 Consonant with the present study’s identification of the importance of emotional support, the Hong Kong peer-support program reduced emotional distress as well as hospitalizations among approximately 20% of participants who were initially above norms on measures of anxiety, depression and stress.11
Acknowledgments
We would like to thank the following organizations which supported this programs: Hefei City Health Bureau, Hefei City CDC, Shu-shan District CDC, Heyidi CHSC, Tongling City Health Bureau, Tongling City CDC, Tong guan-shan District CDC, Yangguan CHSC, Rendong CHSS, Bangbu City Health Bureau, Bangbu City CDC, Yuhui District CDC, Daqing CHSC.
We also thank Jennifer Butterworth Robinette, MA, who provided valuable assistance in preparing the manuscript.
Footnotes
Conflicts of interest: Edwin B. Fisher, PhD, receives salary support for his role as Global Director of Peers for Progress from the American Academy of Family Physicians Foundation and has also received compensation for serving as a consultant and advisory board member for the Foundation for activities unrelated to the present paper.
Funding support: Funding for this research was provided by the American Academy of Family Physicians Foundation through the Peers for Progress program with support from the Eli Lilly and Company Foundation and by the Anhui Provincial Health Bureau.
Previous presentations: Reciprocal cooperation between peer supporters and community health centers in China. Zhong X. Annual Meeting of the Society of Behavioral Medicine; April 11 – 14, 2012; New Orleans, Louisiana. Peer support interventions for diabetes and community health centers in China. Zhong X. Biannual International Congress of Behavioral Medicine; August 29 – September 1, 2012; Budapest, Hungary.
Supplementary materials: Available at http://www.AnnFamMed.org/content/13/Suppl_1/S50/suppl/DC1/
- Received for publication August 18, 2014.
- Revision received March 13, 2015.
- Accepted for publication March 24, 2015.
- © 2015 Annals of Family Medicine, Inc.
References




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pre-diabetes virtual health management community (VHMC) intervention and group interaction management model in China: a randomised clinical trial protocol
- Effectiveness of a clinic-based randomized controlled intervention for type 2 diabetes management: an innovative model of intensified diabetes management in Mainland China (C-IDM study)
- Key Features Of Peer Support In Chronic Disease Prevention And Management