
Abstract
PURPOSE Primary care needs new models to facilitate advance care planning conversations. These conversations focus on preferences regarding serious illness and may involve patients, decision makers, and health care providers. We describe the feasibility of the first primary care–based group visit model focused on advance care planning.
METHODS We conducted a pilot demonstration of an advance care planning group visit in a geriatrics clinic. Patients were aged at least 65 years. Groups of patients met in 2 sessions of 2 hours each facilitated by a geriatrician and a social worker. Activities included considering personal values, discussing advance care planning, choosing surrogate decision-makers, and completing advance directives. We used the RE-AIM framework to evaluate the project.
RESULTS Ten of 11 clinicians referred patients for participation. Of 80 patients approached, 32 participated in 5 group visit cohorts (a 40% participation rate) and 27 participated in both sessions (an 84% retention rate). Mean age was 79 years; 59% of participants were female and 72% white. Most evaluated the group visit as better than usual clinic visits for discussing advance care planning. Patients reported increases in detailed advance care planning conversations after participating (19% to 41%, P = .02). Qualitative analysis found that older adults were willing to share personal values and challenges related to advance care planning and that they initiated discussions about a broad range of relevant topics.
CONCLUSION A group visit to facilitate discussions about advance care planning and increase patient engagement is feasible. This model warrants further evaluation for effectiveness in improving advance care planning outcomes for patients, clinicians, and the system.
INTRODUCTION
Despite the benefits of advance care planning for patients, primary care clinicians face barriers to effective counseling on the issue, including their limited time and a lack of clinic-based support.1–4 The Dying in America report5 emphasized the need to integrate advance care planning into clinical care, and the Centers for Medicare and Medicaid Services recently approved reimbursement for counseling on advance care planning.6 Advance care planning is an ongoing process that involves multiple conversations among individuals, family members, and health care professionals.1,7 Studies show that many US decedents had not discussed preferences for end-of-life care with someone close to them, completed a living will, or established a durable power of attorney for health care.8,9
Primary care clinics are uniquely positioned to implement new models that engage patients in advance care planning.10 The American Academy of Family Physicians recognizes group medical visits (GMVs) as a strategic approach within the patient-centered medical home.11,12 GMVs, also called shared medical appointments, engage patients in health promotion and disease management.13–18 Older adults enrolled in chronic disease management GMVs showed improved health status, satisfaction with care, and self-efficacy, as well as decreased health care utilization.19 Key GMV strengths include increased patient satisfaction, support for behavior change, and patient engagement.16,18
Given how GMVs support patient engagement through group interaction, we developed the first advance care planning group visit, the “Conversation Group Medical Visit.” This model leverages group dynamic to transform the typical patient-clinician encounter related to advance care planning. This article describes a pilot demonstration of the new model.
METHODS
Setting and Participants
Seniors Clinic at the University of Colorado Hospital (Aurora, Colorado) is a patient-centered medical home that provides primary care for about 1,900 older adults. The team includes physicians and mid-level providers (11 clinicians representing 4.5 clinical full-time equivalents), a social worker, nurses, pharmacists, medical assistants, and schedulers. Seniors Clinic patients average 83 years old; 63% are female, 69% white and 13% black. Seniors Clinic has a long-standing, monthly GMV focusing on geriatric well-being. Building on this experience, we developed the Conversation GMV as a pilot demonstration project to promote advance care planning. The name reflects use of The Conversation Starter Kit as a teaching tool.20 Results are from 5 cohorts who participated in visits between November 2013 and June 2014. This project was approved by the Colorado Multiple Institutional Review Board.
Patients could participate if they were aged 65 years or older, spoke English, and received primary care at Seniors Clinic. Patients were asked to participate if they were referred by their primary care clinicians, self-referred in response to clinic-based flyers, or were referred by a partner or friend. We encouraged clinicians to refer patients they felt would be able to participate in a group setting; that is, patients who did not have significant cognitive, hearing, or mental health impairments. We did not test the cognitive function of referred patients or exclude patients based on cognitive function. Clinicians were not asked to prioritize patients with poor health status, difficulty with advance care planning conversations, or known end-of-life needs. We sent referred patients an invitation letter and followed up by telephone to describe the program and schedule the 2 sessions. Our goal was to have 8 to 12 patients per cohort based on an estimate of appropriate size to foster group discussion around advance care planning.
Conversation Group Medical Visit
The Conversation Group Medical Visit aims to engage patients in a discussion of key advance care planning concepts and support patient-initiated advance care planning actions—choosing surrogate decision makers, deciding on preferences during serious illness, discussing preferences with decision makers and health care providers, and documenting advance directives in the electronic health record (EHR).21 The group visits involve 2 sessions of 2 hours each, 1 month apart, co-facilitated by a geriatrician and a social worker. Table 1 provides an overview of the GMV structure, facilitator considerations, session format, and documentation and billing details. The discussions include sharing experiences related to advance care planning, considering values related to serious illness, choosing surrogate decision makers, deciding how much flexibility to allow decision makers, and having conversations with decision makers and clinicians.22,23 The facilitators aim to support an interactive discussion that affords opportunities for patients to learn from the experiences and perspectives of others. To support the facilitators’ role, we developed a “Facilitators’ Communication Guide” (Table 2), which is similar to other patient/provider communication guides.25 The Conversation GMV aims to help patients identify and achieve individualized goals related to advance care planning, including having conversations and choosing surrogate decision makers.
Conversation Group Medical Visit Structure
Facilitators’ Communication Guide
Like other group visit models,26 this GMV was integrated into the geriatric clinic using existing medical assistants and front desk staff for check-in processes. Patients sign a standard GMV clinical consent outlining their agreement to maintain privacy and acknowledging that routine co-payments apply. Patients receive an agenda for both visits, a personal copy of their EHR highlighting current advance care planning documentation, if any, and a blank medical durable power of attorney form. Facilitators use educational materials to guide the group discussion on advance care planning, including the Conversation Starter Kit,20 videos from the PREPARE website24 (http://www.prepareforyourcare.org) that demonstrate a family’s conversation, advance directives, and other resources, such as out-of-hospital orders.27 The Conversation Starter Kit is a handout that prompts individuals to think about their values and guides conversations about preferences.20 PREPARE is a website designed to help individuals prepare for medical decision making and has been shown to help older adults engage in advance care planning.24 Two of the authors, H.D.L. and R.S., established a licensing agreement between their respective institutions to support the use of PREPARE within this program. The GMV uses PREPARE videos showing various degrees of flexibility in the decision-making role.
After the group portion of the session, patients can request brief individual medical visits with the GMV physician to address acute medical issues. The GMV physician sends visit documentation via the EHR to each patient’s primary care clinician with a description of the patient’s perspectives on advance care planning, preferences for future health care choices, goals for advance care planning, opportunities for follow-up by the primary care clinician, and information about any acute medical issues present. The patient’s EHR is updated with advance care planning preferences and documentation. The visits typically meet criteria for an established office visit of Current Procedural Terminology code 99213.28
Implementation Strategy
After developing the Conversation GMV, the facilitators, schedulers, medical assistants, and program assistants met to coordinate team members’ roles in the clinic workflow. The geriatrician facilitator introduced the goals, structure, and referral process to clinicians and staff during regular meetings, developed an EHR-based referral order, and posted flyers in clinic rooms. We conducted an initial test cohort in September and October of 2013 before officially starting in November 2013. The test cohort included 8 patient volunteers who participated in 2 sessions to confirm that clinic staff could conduct the clinic workflow processes and facilitators could use the Facilitators’ Discussion Guide before the start of the pilot study.
Evaluation Strategy
We used the RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance) to evaluate this pilot demonstration project.29,30 Using this framework, we addressed the following:
Reach: Will older adults participate in an advance care planning group visit?
Effectiveness: Will older adults engage in advance care planning conversations?
Adoption: Will providers refer patients?
Implementation: Will patients come to both sessions?
What aspects of advance care planning will older adults discuss in the GMV?
The maintenance portion of the RE-AIM framework was not evaluated in this pilot.
Data sources included GMV transcripts, patient demographics, and post-session evaluations that were managed using Research Electronic Data Capture (REDCap).31 Detailed project notes captured implementation efforts and outcomes. Referral and participation data included referral source (provider, self, partner/friend) and, among those who declined to participate, reasons for declining. For this pilot demonstration project, we developed and administered patient evaluations to collect demographic information, perspectives on the GMV using a 5-point Likert scale (adapted from author I.L.’s prior GMV evaluations), and assessed impact on advance care planning conversations (from The Conversation Project20). Specifically, after Session 1, patients were asked, “Prior to today’s discussion about advance care planning, have you had this kind of conversation?” After Session 2, they were asked, “Did you have the conversation?” Patients could respond: “No,” “No, but I have thought about it,” “Yes, but at a general level,” or “Yes. The conversations included enough details that I feel confident my loved ones know my wishes.” A Wilcoxon signed-rank test was used to test for change in detailed advance care planning conversations before and after the GMV.
GMV sessions were audio recorded, transcribed, and analyzed using a mixed inductive and deductive approach.32 Data analysis involved systematic organization of the data through open coding, and repeated, constant comparison across coded data to identify consistent themes.33 We used a team approach to analysis, including regular meetings to discuss coded data and to reach consensus on identified themes and their meanings. Initial coding focused on the question, “What aspects of advance care planning will older adults discuss in the GMV?” We reviewed transcripts to catalog specific advance care planning topics, iteratively discussing the themes, interpretation, and potential implications of our findings using the qualitative analysis technique triangulation. Triangulation is a process of convening individuals with different perspectives to facilitate a deeper understanding and trustworthiness of the findings. Our authorship team includes geriatric palliative medicine specialists [H.L., R.S, C.L., and D.M.], a nurse qualitative researcher [J.J.], a group visit specialist [I.L.], implementation scientists [R.G. and D.M.], and academic leaders [R.S. and J.K.].
RESULTS
Reach: Patient Participation
We conducted 5 Conversation Group Medical Visit cohorts in Seniors Clinic (10 total sessions). Of 80 patients approached, 32 participated in at least 1 session, for a participation rate of 40%. Mean age of participants was 79 years, 59% were women, and 72% were white. Table 3 shows patient characteristics, referral sources, and, for patients who were approached but did not participate, reasons for not participating. Among 30 patients who declined to participate, reasons for declining included past advance care planning conversation or existing advance directive (30%), lack of interest (13%), illness (3.3%), lack of transportation (3.3%), and other/unknown (50%). While the goal was to schedule 8 to 12 patients per cohort, actual group sizes ranged from 4 to 9 patients due to patient cancelations.
Characteristics of Conversation Group Medical Visit Participants Compared With Patients Who Were Approached But Did Not Participate
Effectiveness: Patient Acceptance of and Engagement in Advance Care Planning Conversations
The majority of patients rated the Conversation Group Medical Visit as better than usual clinic visits for talking about advance care planning, thought they received useful information, felt comfortable talking about advance care planning in the group, and found talking with others about advance care planning to be helpful (Figure 1). Patients reported an overall increase in advance care planning conversations with loved ones after participating, including an increase in conversations with enough details that the patient felt confident that their loved ones knew their wishes (19% to 41%, P = .02; Figure 2). Of 24 patients who reported having had an advance care planning conversation, 92% felt comfortable; 58% felt prepared, and 38% felt somewhat prepared.

Patient experience of the conversation group medical visit.
Note: Data are drawn from an evaluation that patients completed to assess their levels of agreement with 4 statements concerning acceptability of the Conversation Group Medical Visit. The evaluation used a 5-point Likert scale. (n = 29; 2 patients did not complete evaluations.)
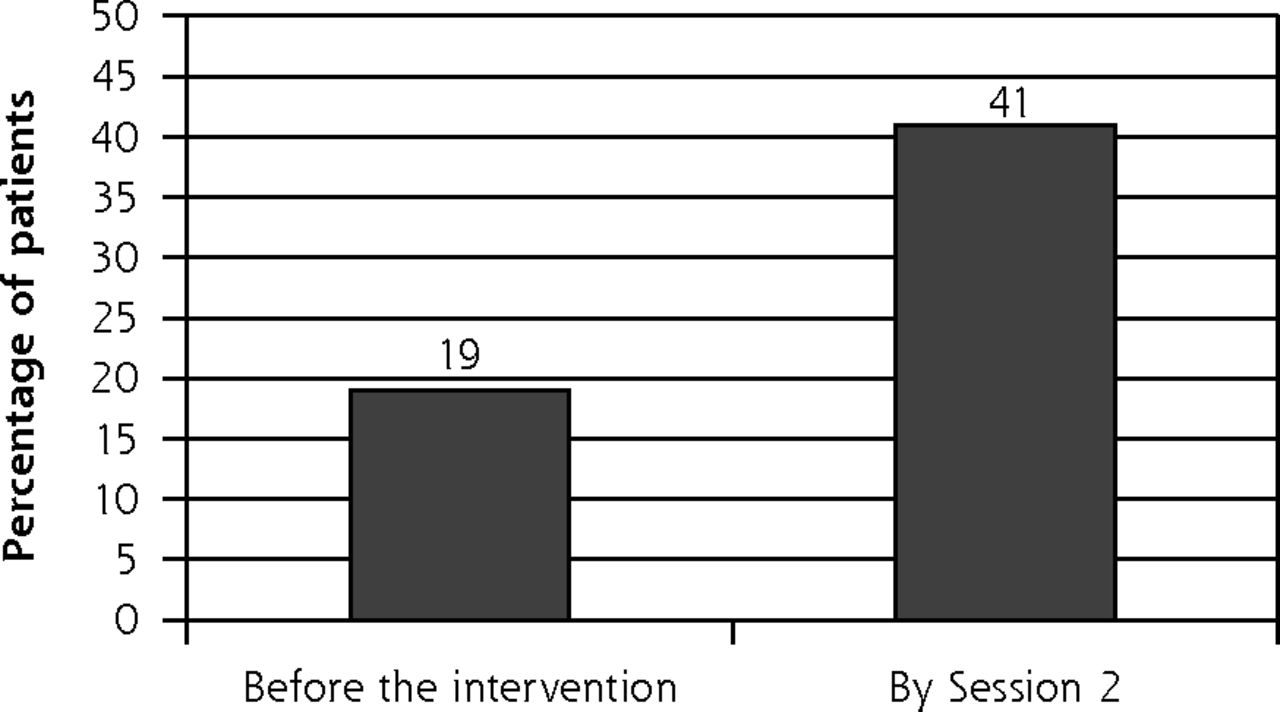
Patient engagement in advance care planning conversations.
Note: During Session 1 and after participating in Session 2, patients were asked if they had had an advance care planning conversation. Bars represent the percentage of patients who answered, “Yes. The conversations included enough details that I feel confident my loved ones know my wishes.” (P = .02)
Adoption: Clinician Referral Patterns
Ten of 11 clinicians referred at least 1 patient to the Conversation Group Medical Visit. The median number of referrals was 5, with a range of 1 to 23, where 23 patients were referred by the geriatrician project lead (H.D.L.). The second largest number of referrals from 1 clinician was 11. More than 80% of participants were referred by their primary care clinicians (Table 3), though some self-referred or were referred by a partner or friend. Among GMV participants (n = 32), there was a range of 0 to 5 patients per provider. Eight of 11 providers had at least 1 patient participate.
Implementation: Patient Retention and Aspects of Advance Care Planning Discussed
Patient retention was 84%, with 27 of 32 patients participating in both sessions. One patient missed Session 1 but came to Session 2, making the total for that session 28 patients. Key discussion themes included sharing personal values and challenges related to advance care planning and discussing a broad range of patient-raised topics related to advance care planning.
Theme 1. Patients Shared Personal Values and Challenges Related to Advance Care Planning
The Conversation GMVs encouraged patients to share experiences related to advance care planning in the group setting. Patients told stories that reflected their personal values and challenges they had faced concerning serious illness or the experiences of loved ones as they approached death. In a discussion of future care preferences, some individuals had not thought much about what was important to them, while others had. One patient expressed her personal values:
We had this very discussion when a new [health care professional] came into my life and was just almost insisting that I have all kinds of tests and things. I don’t want to live forever. I want to live when the quality of my life is in balance.
In the discussion about choosing a surrogate decision maker, some individuals said they had already made a choice and reported having completed formal documentation. For others, however, considering a surrogate was challenging because they weren’t sure they could trust available surrogates to follow their wishes. One woman shared her challenges in considering her husband as her decision maker:
One of the things that surprised me was he said he didn’t want to be the care agent. He didn’t know if he could ask that things be removed. He is more emotional than I am.
Theme 2. Patients Initiated Group Discussions of a Broad Range of Advance Care Planning Topics
The facilitated discussions introduced key advance care planning concepts (see Table 2, Facilitators’ Communication Guide) and encouraged patients to share related experiences, questions, successes, and challenges. Beyond the topics raised by facilitators, patients in each session raised questions and concerns for discussion. Table 4 provides examples of the breadth of such topics. Many questions were practical, for instance about how to ensure that advance directives be available when needed. One patient asked,
The methods of getting that advance directive to the right person at the right time are not clear to me. How do they know? If you are 3 sheets to the wind, you can’t do anything…. You have to make arrangements before that happens.
Topics Brought Up By Conversation Group Medical Visit Patients
In addition to questions about aspects of advance care planning, patients raised a broad range of topics pertinent to older adults with serious illnesses, including assisted living facilities, nursing homes, palliative care and hospice. One woman commented,
[My husband had] hospice in a nursing home. It was just wonderful…. They just kept him very comfortable…. It was a beautiful death. It is a horrible thing to say, but it was a peaceful, wonderful end to his life.
Members of smaller cohorts (those of 4 to 6 patients), tended to mention fewer personal examples, ask fewer question, and discuss a smaller range of advance care planning experiences and topics than those in larger groups.
DISCUSSION
The Conversation GMV is a novel approach to facilitating advance care planning in primary care. The model uses the group visit to engage patients in detailed advance care planning conversations by providing a safe and supportive environment where patients share personal values and challenges and ask a range of questions related to advance care planning. Older adults were willing to attend visits of this new clinical model, found it helpful, and were willing to share personal values and challenges related to advance care planning. Patients initiated discussions on a broad range of advance care planning topics. A GMV focused on advance care planning can tailor information and discussion to questions that patients consider important. Three-quarters of patients had advance care planning conversations after participating in Session 1, including 41% who had detailed conversations, and many reported feeling comfortable and prepared.
This GMV may influence outcomes that are important to patients and primary care clinicians. Potential patient-centered outcomes include improved satisfaction, knowledge, and motivation to participate in advance care planning. The GMV may facilitate advance care planning actions, including values clarification, conversations with surrogate decision makers and clinicians, and advance directive completion. It may also increase primary care clinicians’ knowledge of their patient’s wishes and their ability to provide medical treatment aligned with those wishes. Future work should formally evaluate the effects of the Conversation GMV on providers and clinic staff.
Some of the results suggest a need to understand barriers and facilitators to real-world implementation of the model. The 40% participation rate is higher than seen in other GMV studies involving older adults and other medical topics, suggesting that patients are interested and will participate in GMV on advance care planning.13,34,35 On the other hand, the actual group sizes were lower than our goal and were limited by the rate of referrals, the number of patients who were unable to participate, and last minute cancelations and rescheduling. Patients in groups of 4 or 5 seemed less engaged in the discussion than those in groups of 7 or 9 patients, suggesting that group size may have an important effect on outcomes. Future cohorts could be over-scheduled by 2 or 3 patients given the frequent occurrence of last-minute cancelations. The Conversation GMV must also meet the needs of older patients with sensory, cognitive, and functional limitations, which is an issue beyond the scope of this pilot demonstration.36
Key barriers to future implementation may include the need for sustainable workflows for patient referral and scheduling as well as financial support for facilitator and staff training. Key factors promoting implementation may include strong, team-based interest in improving advance care planning, available clinic resources to conduct group visits (for example, meeting space, trained staff, and advance care planning patient education materials), and reimbursement models that support advance care planning and group-based care delivery.
The cost considerations of this model are similar to those of other GMVs.15,37 Potential financial challenges include adequate reimbursement for services, including patient co-payments, though multiple health care systems are successfully implementing and sustaining GMVs.15,25,36 The Conversation GMV can be facilitated by providers other than physicians, such as nurse practitioners or physician assistants,38 as long as they are trained in GMV facilitation and counseling in advance care planning. The Centers for Medicare and Medicaid Services recently approved payment for CPT codes for counseling in advance care planning, supporting the integration of advance care planning into clinical settings.6
Future evaluation should assess communication of patient preferences within the health care system, including documentation of advance directives. This project warrants formal evaluation, since it may be an effective model for integrating high-quality, patient-centered advance care planning into primary care.
Acknowledgments
The authors would like to thank John Scott, MD, a pioneer in group medical visits since 1991, who established and taught many patients and health care providers the value of the group medical visit, and has been discussing advance care planning in this context for over a decade. Dr Scott and Ingrid Lobo, MD, a current champion for group medical visit implementation at our institution, laid the foundation for the development of the Conversation Group Medical Visit. We also appreciate the excellent clinical work of the University of Colorado Seniors Clinic staff who assisted with implementation and conduct of this project. Additional special thanks to Sue Felton, MA, and Dana Lahoff, LCSW, for their tireless assistance with the development, implementation, and evaluation of this model in our local primary care setting.
Footnotes
Conflicts of interest: authors report none.
Funding support: This pilot demonstration project is supported in full or in part by The Colorado Health Foundation (#5509), University of Colorado Hospital/University Physicians Incorporated Primary Care Strategic Initiative Fund, a Junior Faculty Career Development Grant from the National Palliative Care Research Center (NPCRC), and the Colorado Clinical & Translational Sciences Institute (CCTSI) with the Development and Informatics Service Center (DISC) grant support (NIH/NCRR Colorado CTSI Grant Number UL1 RR025780) for use of REDCap-based data management. The sponsors had no role in the design, methods, or preparation of the manuscript. The views in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Previous presentations: These results were initially presented at the 2015 American Academy of Hospice and Palliative Medicine Annual Assembly; February 25–28, 2015; Philadelphia, Pennsylvania.
- Received for publication July 14, 2015.
- Revision received November 11, 2015.
- Accepted for publication November 24, 2015.
- © 2016 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advance care planning in COPD: guidance development for healthcare professionals
- Clinician Perspectives on Group Visits for Advance Care Planning Among Caregivers and Older Adult Patients With Heart Failure
- Feasibility of Group Visits for Advance Care Planning Among Patients with Heart Failure and Their Caregivers
- Effect of an Interactive Website to Engage Patients in Advance Care Planning in Outpatient Settings
- Barriers, enablers and initiatives for uptake of advance care planning in general practice: a systematic review and critical interpretive synthesis
- CPR decision-making conversations in the UK: an integrative review
- A Group Visit Initiative Improves Advance Care Planning Documentation among Older Adults in Primary Care
- In This Issue: Confronting Constraints on Individual Behavior & Outcomes