
Abstract
The Patient Protection and Affordable Care Act (ACA) mandates that health insurance plans include sufficient access to behavioral health providers, but lacks specific guidelines to define sufficient access. Using a secret shopper methodology, we called behavioral health providers in the Denver metropolitan area networked with 3 large insurance companies. We found that, depending on insurance company and level of training, 9.8% to 59% of providers could offer a new patient appointment, with psychiatry appointments being particularly difficult to schedule. These findings are consistent with similar studies conducted in other regions, suggesting that access to outpatient behavioral health care is limited despite existing ACA regulations.
INTRODUCTION
More than one-half of Americans struggle with a mental health condition in their lifetime1 and in 2014 alone, 18.1% of all US adults experienced a form of mental illness.2 Under the Patient Protection and Affordable Care Act (ACA), health insurance plans must include mental health services as an essential health benefit. But are these services accessible to those who need them?
Network adequacy, a health plan’s ability to offer access to primary and specialty health care providers, is crucial to ensuring access to services. Under the ACA a plan must “maintain a network that is sufficient in numbers and types of providers, including providers that specialize in mental health and substance abuse services, to assure that all services will be accessible without unreasonable delay.”3 The federal requirements, however, do not specify what constitutes a “sufficient” number of providers or “unreasonable delay,” giving each state the power to define and enforce these requirements. Our study examines access to outpatient behavioral health care in 1 major metropolitan area after implementation of the Affordable Care Act.
METHODS
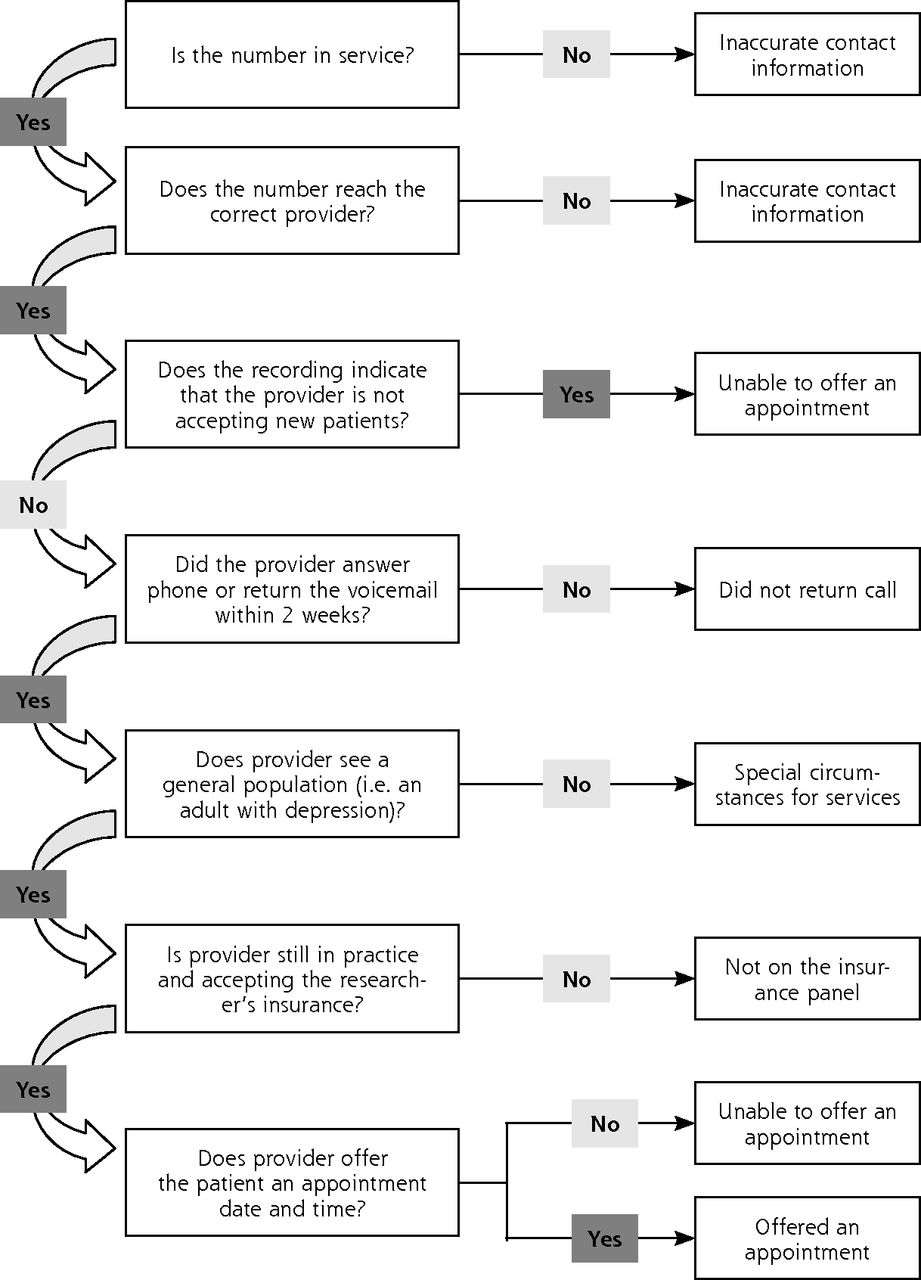
The project used a secret shopper methodology, which has been successfully used in other studies evaluating access to health care.4–6 Three researchers made scripted telephone calls to all behavioral health providers within 20 miles of central Denver who were listed in the online insurance directories of Anthem BlueCross BlueShield, United Healthcare, and Cigna. These companies are the largest insurance providers in Colorado that offer preferred provider organization (PPO) plans through Colorado’s Health Insurance Marketplace.7 The researchers posed as potential patients with mild to moderate depression and inquired about the next available appointment date. Data were collected and organized as summarized in Figure 1. This research was approved by the Colorado Multiple Institutional Review Board.

Method used to organize data collected from phone calls to behavioral health care providers.
RESULTS
Researchers made 1,932 calls to behavioral health providers included in the networks of the insurance companies listed above in 2014–2015. Across the 3 insurance companies, 13.0% of directory entries were inaccurate. Only 43.6% of all calls and 9.8% to 13.6% of calls to psychiatrists yielded appointments. Table 1 details the outcomes of these calls.
Results of Telephone Calls Made to Behavioral Health Care Providers
DISCUSSION
Despite the provisions of the Affordable Care Act, access to behavioral health care remains limited for private insurance holders. Our data suggest that a patient in the Denver area would need to call 7 to 10 psychiatrists, depending on the insurance company, to find an available appointment. In addition, the directories had numerous inaccuracies including incorrect contact information for providers and listings of providers who had left the networks covered by the directories.
Our findings build on those from similar studies conducted in other regions. The Mental Health Association of Maryland found in 2013 that only 13.5% of outpatient psychiatrists on private insurance panels surveyed could offer an appointment.4 The Mental Health Association in New Jersey found that 33% of psychiatrists had incorrect contact information in the insurance directories and that although 51% of psychiatrists were taking new patients, nearly one-half of them were booked more than 1 month out.5 Additionally, our results mirror findings from a 2015 California study of access to primary care that found numerous errors in network directories and reported an appointment rate of 31% for calls to Marketplace plan providers, indicating that network inadequacy extends beyond the realm of behavioral health care.
To our knowledge, this study provides the first quantitative look at access to behavioral health care in Colorado since implementation of the Affordable Care Act. Insured patients continue to face multiple challenges when attempting to use behavioral health services due to network inadequacy as well as other factors, including the low percentage of psychiatrists accepting insurance (55%) and the decline in number of practicing psychiatrists in the United States.8 Given the stigma and fatigue associated with mental illness, the lengths patients must go to obtain an appointment are particularly concerning.
Since we conducted our study, federal guidelines were added that require monthly directory updates,9 which we hope will reduce the number of directory inaccuracies. Despite this, we believe that the nonspecific requirements outlined in the Affordable Care Act regarding network adequacy remain insufficient and require further delineation and regulation with longitudinal monitoring of progress to ensure that the 1 in 6 Americans suffering from mental illness each year can access appropriate and timely care.
Limitations of the study include our using 3 different secret shoppers, although any differences in approach were mitigated by using a uniform, IRB-approved script, and our surveying carriers at different times (Carrier C in 2014 and Carriers A and B in 2015). Given that the network adequacy legislation changed little during this time, we believe the data are comparable.
Acknowledgments
We appreciate the guidance of Larry A. Green, MD, in our preparation of this manuscript and the assistance of the University of Colorado Department of Family Medicine, William LeBlanc, PhD, and Lynn VanderWielen, PhD, in conducting this study and analyzing the results.
Footnotes
Conflicts of interest: authors report none.
Previous presentations: Poster presented at the Shared Networks of Colorado Ambulatory Practices and Partners Conference; September 25–26, 2015; Colorado; and the Collaborative Family Healthcare Association National Conference; October 15–17, 2015; Portland, Oregon.
Funding support: Funding for this study was provided by the Department of Family Medicine, University of Colorado School of Medicine.
- Received for publication November 1, 2016.
- Revision received January 30, 2017.
- Accepted for publication February 19, 2017.
- © 2017 Annals of Family Medicine, Inc.




{kind=link}