
Abstract
PURPOSE The influence of multimorbidity on the clinical encounter is poorly understood, especially in areas of high socioeconomic deprivation where burdensome multimorbidity is concentrated. The aim of the current study was to examine the effect of multimorbidity on general practice consultations, in areas of high and low deprivation.
METHODS We conducted secondary analyses of 659 video-recorded routine consultations involving 25 general practitioners (GPs) in deprived areas and 22 in affluent areas of Scotland. Patients rated the GP’s empathy using the Consultation and Relational Empathy (CARE) measure immediately after the consultation. Videos were analyzed using the Measure of Patient-Centered Communication. Multilevel, multi-regression analysis identified differences between the groups.
RESULTS In affluent areas, patients with multimorbidity received longer consultations than patients without multimorbidity (mean 12.8 minutes vs 9.3, respectively; P = .015), but this was not so in deprived areas (mean 9.9 minutes vs 10.0 respectively; P = .774). In affluent areas, patients with multimorbidity perceived their GP as more empathic (P = .009) than patients without multimorbidity; this difference was not found in deprived areas (P = .344). Video analysis showed that GPs in affluent areas were more attentive to the disease and illness experience in patients with multimorbidity (P < .031) compared with patients without multimorbidity. This was not the case in deprived areas (P = .727).
CONCLUSIONS In deprived areas, the greater need of patients with multimorbidity is not reflected in the longer consultation length, higher GP patient centeredness, and higher perceived GP empathy found in affluent areas. Action is required to redress this mismatch of need and service provision for patients with multimorbidity if health inequalities are to be narrowed rather than widened by primary care.
INTRODUCTION
Multimorbidity—defined as the coexistence of 2 or more long-term conditions within an individual—is now the norm rather than the exception in high-income countries.1 Although related to aging, multimorbidity is also socially patterned, being more common and occurring at a younger age in those of lower socioeconomic status.1,2 People with multimorbidity living in areas of high socioeconomic deprivation struggle to cope with everyday life tasks,3 and have lower quality of life compared with more affluent patients with multimorbidity.4 The effect of multimorbidity on unplanned hospital admissions is also exacerbated by deprivation, including ambulatory care–sensitive conditions which could in principle be managed in the community if primary care was working more effectively.5
The clinical encounter lies at the heart of primary care, yet there has been surprisingly little research on how multimorbidity influences the consultation,6 and how or whether patients with multimorbidity needs are met within routine clinical encounters in affluent and deprived areas.7 Qualitative research shows that GPs working in deprived areas find it hard to manage patients with multimorbidity.8 This is exacerbated by the inverse care law (which states that “the availability of good medical care tends to vary inversely with the need for it in the population served”) which continues to blight health care, even in countries such as the United Kingdom with its universal coverage and national health service (NHS) free at the point of care.9–11 Reflecting the inverse care law, patients living in areas of high deprivation have poorer access to primary care, shorter consultation length, less enablement, and doctors who are more stressed compared with those working in more affluent areas.12 Empathic, patient-centered care is a prerequisite for patient enablement and improves health outcomes in both affluent and deprived areas.13–15
In the present study, we examined the influence of multimorbidity on general practice consultations, in areas of high and low socioeconomic deprivation. We hypothesized that in affluent areas, where workforce pressures are less severe,11 the greater needs and complexity of patients with multimorbidity would result in longer consultations, and more empathic, patient-centered care than in less complex patients without multimorbidity, but that in deprived areas, due to the ongoing inverse care law,11 these effects of multimorbidity on the consultation would not be possible.
METHODS
Study Design
This study was a secondary cross-sectional analysis of a previous study of 659 consultations in primary care settings in Glasgow, Scotland, United Kingdom.15 The study comprised patient-administered questionnaires and videotaping of consultations. The study protocol and recruitment procedures have been previously reported.15 Ethical approval of the study was obtained from the local research ethics committee (approval number: REC/06/SO701/43) and informed consent was obtained from all participating GPs and patients.
Recruitment of Practices and Patients
The details of the original study protocol and recruitment procedures are already reported in full.15 In brief, 20 practices, 47 GPs, and 659 patients (339 with multimorbidity) participated (13 practices, 25 GPs, 356 patients in high-deprivation areas including 207 patients with multimorbidity; 7 practices, 22 GPs, 303 patients in low-deprivation areas with 132 patients with multimorbidity). Practices were recruited from the upper and lower quartile of deprivation (Scottish Index of Multiple Deprivation, SIMD 2006)16 in the Greater Glasgow and Clyde health board area, Scotland, United Kingdom. The mean deprivation scores of the participating practices and patients were comparable to those of all practices in the high- and low-deprivation areas. Consecutive, unselected patients (aged >17 years) from the participating practices received an information sheet from reception staff when they checked in, and a researcher then gained informed consent.
Patient Questionnaire at Consultation and Follow Up
Before the consultation, patients completed a questionnaire that included questions on their demographics, number of problems they wished to discuss, and the extent to which their daily activities were limited by their conditions.15 Immediately after consultation, patients reported their perceptions of the GP’s empathy using the Consultation and Relational Empathy (CARE)17 measure.
Consultation Video Rating
Consultation videos were coded for GP behaviors with the Measure of Patient-Centered Communication (MPCC), as reported previously.15 The MPCC consists of 3 components: exploring both the disease and illness experience, understanding of the whole person, and finding common ground.18
Statistical Analysis
We carried out descriptive unadjusted analysis of the patients’ demographic details, health status, and health care needs, comparing patients with multimorbidity with patients without multimorbidity, in both affluent and deprived settings. Differences between patients with multimorbidity and patients without multimorbidity in both groups were analyzed by the appropriate parametric and nonparametric tests (unpaired t-test and Mann-Whitney tests) depending on the distribution of the variables and data type (continuous or non-continuous data).
We then compared the key consultation characteristics of interest (consultation length, GP empathy, patient-centered care) in patients with multimorbidity vs patients without multimorbidity, consulting GPs in high or low deprivation areas. In this analysis, we controlled for patients’ age, sex, and clustering effects of patients within individual GPs, using multilevel regression models (SAS version 9.2, SAS Institute) adjusting for GP as a random effect with fixed effects for patient age and sex. Our rationale was that age and sex could both feasibly influence consultation characteristics independent of multimorbidity, and the nature of our data was that patients were clustered within GPs and GPs within practices.15 In our previous analysis of the same data set, we found evidence of clustering effects at the GP level (patients within GPs) but not at practice level (GPs within practices).15 Thus in the current analysis we adjusted for the former but not the latter.
RESULTS
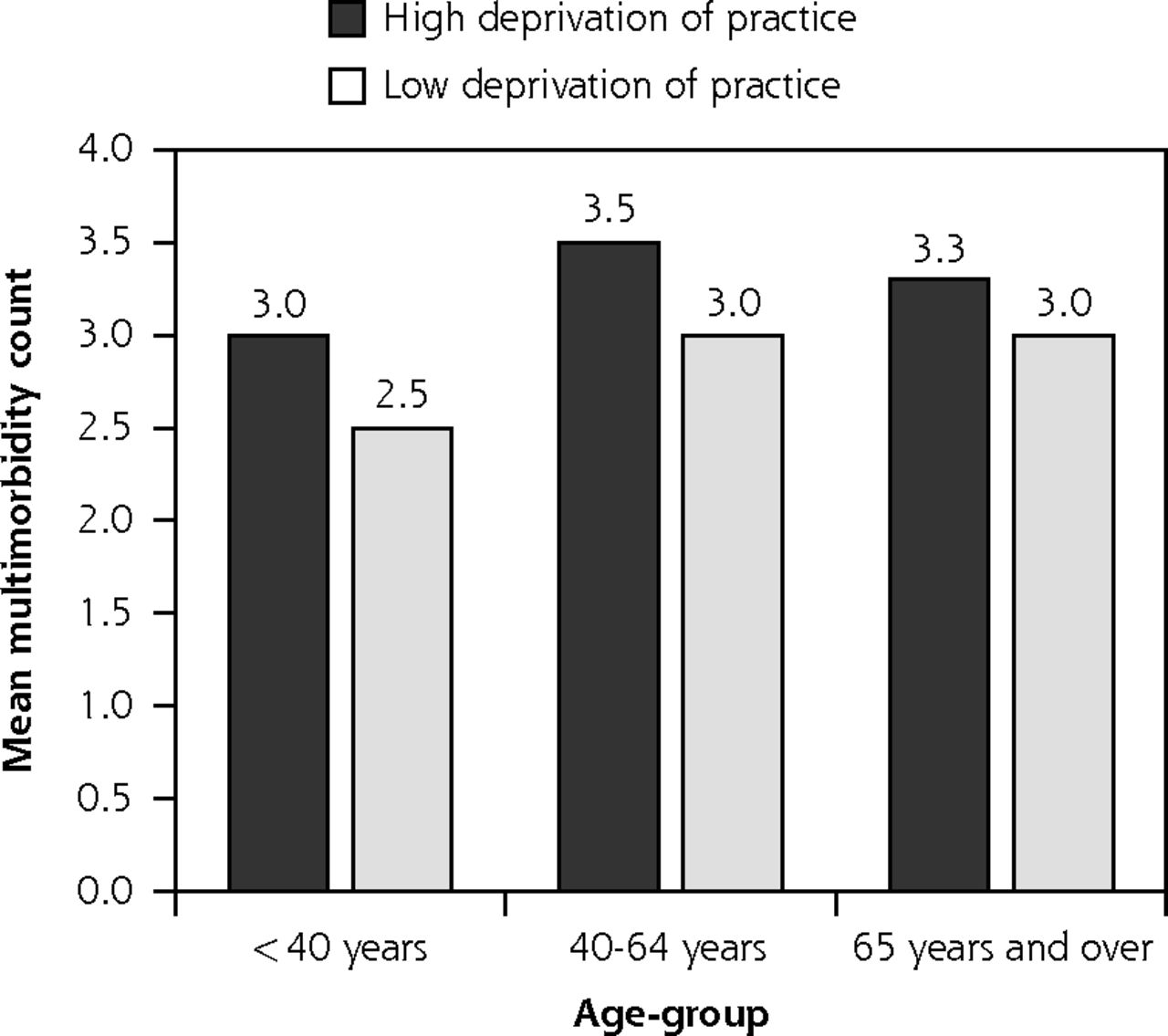
The age, sex, and ethnicity of the participating GPs did not differ between the high- and low-deprivation areas; patient ethnicity also did not differ significantly between groups with over 95% speaking English as their first language (results not shown). As expected, more patients had multimorbidity (2 or more conditions) in deprived areas (207/356; 58%) compared with affluent areas (132/303; 44%) (P <.001). The average number of conditions per patient with multimorbidity was 3.4 (SD = 1.64) in the deprived compared with 2.9 (SD = 1.13) in the affluent area (P <.01). This difference was apparent across age-groups (Figure 1).

Mean number of conditions by age-group in multimorbid patients consulting GPs in areas of high and low socioeconomic deprivation.
GP = general practitioner
Patients with multimorbidity were older, had poorer health, were more disabled, consulted more often, and wanted to discuss more problems than patients without multimorbidity (Table 1). Illness burden (poor general health; disability) and demand (frequency of consulting; number of problems to discuss) was significantly higher in the patients with multimorbidity in deprived areas than in the affluent areas (P <.01).
Patient Demographic, Baseline Characteristics and Effects of Multimorbidity
Characteristics of the Consultations
The effect of multimorbidity on the key consultation measures is shown in Table 2. Consultation length was 37% longer (an average of 3 minutes) in patients with multimorbidity compared with those without multimorbidity in the affluent areas, whereas consultation length did not differ in the deprived areas between patients with or without multimorbidity. Patients’ perception of the GPs’ empathy was significantly higher in the affluent patients with multimorbidity compared with the deprived patients with multimorbidity (P <.01) and significantly higher in the affluent patients with multimorbidity vs the affluent patients without multimorbidity (P <.01). In the affluent areas, video analysis showed that the GPs were significantly more interested in exploring the disease and illness experience of patients with multimorbidity, compared with patients without multimorbidity (component 1 of the MPCC; P <.05). This was not apparent in the deprived area. The other 2 components of the MPCC (understanding the whole person and finding common ground) and hence overall rating did not differ significantly between the 2 groups.
Characteristics of Clinical Encounters
DISCUSSION
Summary of Findings
We hypothesized that the greater complexity and clinical needs of patients with multimorbidity would result in longer consultations and more empathic, patient-centered care (compared with patients without multimorbidity) in affluent areas, but that these effects would not be apparent in deprived areas (due to the inverse care law). Our findings are entirely consistent with this hypothesis. Despite the fact that multimorbidity was more common and more burdensome in deprived areas, consultations did not differ significantly from those of patients without multimorbidity.
Comparison With Published Literature
The higher prevalence and severity of multimorbidity in patients consulting GPs in deprived areas found in the present study is in line with our understanding of multimorbidity in Scotland from our previous large scale epidemiological research.2 The fact that multimorbidity is more common in those of lower socioeconomic status has been widely reported now in many other countries.1 In terms of the benefits of longer consultation length, systematic reviews are equivocal but suggest beneficial effects in patients with psychosocial problems.19,20 We have previously found that even modest increases in consultation length improves enablement in patients with complex needs in deprived areas,21 and our randomized controlled trial of a primary care–based complex intervention (CARE Plus) for patients with multimorbidity living in deprived areas based on longer consultations showed evidence of improvements in quality of life and cost-effectiveness over a 12-month period.22
The higher empathy and patient centeredness regarding disease and illness experience in the affluent multimorbid group is also an important finding, since GP empathy and patient-centered approaches have previously been shown to improve patient enablement and health outcomes.13–15 GP empathy and patient centeredness are generally lower in deprived areas compared with affluent,15,23 and a systematic review has recently indicated that this is true generally of doctors dealing with patients of low educational status.24
Policy Implications
The findings of the current study need to be understood in the context of the “inverse care law” which has existed in the UK NHS for over 40 years.9–12 Despite the higher levels of unmet need in deprived areas, the distribution of funding and of GPs in Scotland is flat across deprivation deciles11 resulting in high GP stress, shorter consultations, and worse consultation outcomes in deprived areas.12,15 Tackling this inequity remains essential if health inequalities are to be narrowed rather than widened through the availability of effective health care. In Scotland, ambitious policy changes are afoot regarding integrated primary care and a new GP contract25; it will be important that such changes embrace the inverse care law, which research has suggested can be changed cost effectively with benefit to patients with multimorbidity.22
Strengths and Limitations
A strength of this study was the large sample size of video-taped routine consultations with a comprehensive analysis of observed GP communication, plus patients’ views. The use of multilevel regression analysis in which we adjusted for cluster effects from GP level cluster, and patient age and sex also add to the robustness of the findings. The study was a secondary data analysis, however, and the sample size was thus not powered on the basis of the present analysis, but on the aims of our original work.15
Acknowledgments
The authors would like to thank all the GPs and patients who participated in the study. We also acknowledge the input of Glen Gourlay in data collection and early analysis of the videos.
Footnotes
Conflicts of interest: authors report none.
Funding support: The original study was funded by the Chief Scientist Office, Scottish Government, grant number CZH/4/267.
- Received for publication June 26, 2017.
- Revision received October 27, 2017.
- Accepted for publication November 30, 2017.
- © 2018 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Patients' views on primary care multidisciplinary teams in Scotland: a mixed-methods evaluation
- A model-based approach to estimating the prevalence of disease combinations in South Africa
- Patients experiences of GP consultations following the introduction of the new GP contract in Scotland: a cross-sectional survey
- Is Scotland's new GP contract addressing the inverse care law?
- A mixed-methods evaluation of patients views on primary care multi-disciplinary teams in Scotland
- Ethnic differences in early onset multimorbidity and associations with health service use, long-term prescribing, years of life lost, and mortality: an observational study using person-level clustering in the UK Clinical Practice Research Datalink
- Association between frailty, chronic conditions and socioeconomic status in community-dwelling older adults attending primary care: a cross-sectional study using practice-based research network data
- Prevalence, pattern and determinants of chronic disease multimorbidity in Nepal: secondary analysis of a national survey
- Primary care consultation length by deprivation and multimorbidity in England: an observational study using electronic patient records
- Primary care consultation length by deprivation and multimorbidity in England
- Characteristics of consistently high primary health care users in the DELPHI database: Retrospective study of electronic medical records
- Multimorbidity of chronic non-communicable diseases and its models of care in low- and middle-income countries: a scoping review protocol
- The inverse care law revisited: a continuing blot on the record of the National Health Service
- In This Issue: Refining Care and its Frameworks