
Abstract
PURPOSE Based on the recognition that food insecurity (FI) is associated with poor health across the life course, many US health systems are actively exploring ways to help patients access food resources. This review synthesizes findings from studies examining the effects of health care–based interventions designed to reduce FI.
METHODS We conducted a systematic review of peer-reviewed literature published from January 2000 through September 2018 that described health care– based FI interventions. Standardized mean differences (SMD) were calculated and pooled when appropriate. Study quality was rated using Grading Recommendations Assessment Development and Evaluation criteria.
RESULTS Twenty-three studies met the inclusion criteria and examined a range of FI interventions and outcomes. Based on study design and sample size, 74% were rated low or very low quality. Studies of referral-based interventions reported moderate increases in patient food program referrals (SMD = 0.67, 95% CI, 0.36-0.98; SMD = 1.42, 95% CI, 0.76-2.08) and resource use (pooled SMD = 0.54, 95% CI, 0.31-0.78). Studies describing interventions providing food or vouchers reported mixed results for the actual change in fruit/vegetable intake, averaging to no impact when pooled (–0.03, 95% CI, –0.66 to 0.61). Few studies evaluated health or utilization outcomes; these generally reported small but positive effects.
CONCLUSIONS Although a growing base of literature explores health care–based FI interventions, the low number and low quality of studies limit inferences about their effectiveness. More rigorous evaluation of FI interventions that includes health and utilization outcomes is needed to better understand roles for the health care sector in addressing FI.
INTRODUCTION
Clear and convincing evidence demonstrates food insecurity (FI)— restricted access to adequate food due to a lack of money or other resources1—adversely impacts health and well-being across the life course.2–5 As of 2017, 11.8% of US households reported being food insecure at some point during the year, though rates varied by household demographics.6 For example, over 22% of households headed by non-His-panic Black individuals, 18% of households headed by Hispanic individuals, and 16% of households with children were food insecure.6
Reflecting the health care system’s growing interest in addressing patients’ social risk factors,7,8 several professional medical societies now recommend that health care systems integrate FI screening and referrals to food resources into care.9–11 For example, the American Academy of Family Physicians recently announced the EveryONE Project, which recommends family physicians’ use a social risk assessment tool that includes FI measures; they also provide an online resource platform that can be used to help patients find relevant services.12,13 Large, integrated health systems are similarly experimenting with interventions to address FI as a strategy to improve health.14
Despite this growing enthusiasm, there is little clarity about the impacts of FI interventions initiated in health care delivery settings. This systematic review evaluates the evidence on these programs with the aim of better understanding whether and how these health care–sponsored activities impact food security, patient health and health behaviors, and health care utilization and cost.
METHODS
Data Sources and Search Terms
We searched PubMed, Embase, Web of Science, and clinicaltrials.gov, for studies describing health care–based interventions published from January 2000 through September 2018. The search strategy was developed and refined by 2 study team members (E.H.D., J.M.T.), in consultation with an experienced medical research librarian (E.M.W.). The resulting 2-concept search strategy was adapted to work in each database searched. (Supplemental Appendix, available at http://www.AnnFamMed.org/content/17/5/436/suppl/DC1/.)
Food insecurity was defined as limited access to sufficient food due to lack of financial or other resources. We added search terms related to hunger, food-related stress, and social determinants of health to be comprehensive. Intervention terms were used to focus on interventions and exclude articles that only focused on social risk screening. We consulted experts in the field of health care FI research for additional article suggestions. Grey literature available within Web of Science and Embase was reviewed for inclusion. All search terms and other search details are available in Supplemental Table 1, available at http://www.AnnFamMed.org/content/17/5/436/suppl/DC1/.
Inclusion and Exclusion Criteria
To be included in this review, articles had to describe interventions addressing FI in health care settings. Interventions could address a wider range of adverse social determinants of health (eg, housing or financial insecurity), but were required to specifically describe food security or food access concerns and a description of food security-related outcomes, like food resource use or food security status. Due to the unique national context of health care financing systems, we restricted the review to studies conducted in the United States. Articles had to be published in an English-language, peer-reviewed journal from January 1, 2000 through September 1, 2018. Articles were excluded if they described activities related to FI screening without an associated intervention or did not include data on intervention outcomes.
Data Screening
Search results were stored and organized and duplicates removed in a reference manager. Title, abstract, and full-text screening were completed sequentially using Excel by 2 independent reviewers (E.H.D., J.M.T). After full-text screening, any study recommended by either reviewer was reviewed by an additional author (T.B.). Differences of opinion (n = 4) between reviewers were resolved by discussion at both screening levels. Cited reference searches of the final set of articles were performed in Web of Science.
Data Extraction and Quality Assessment
Extraction tables were constructed to catalog a consistent set of data from each retained article. These data included study design, setting, type of intervention (eg, category of resources/assistance provided), and outcomes evaluated (eg, process measures; social, health, or behavioral outcomes). To compare results from experimental intervention studies, standardized mean differences (SMDs) were calculated using 2-by-2 frequency tables of outcome frequencies, mean or mean gain scores, and t-test or P values of χ2 tests from 2-by-2 tables (depending on available data). The SMD was calculated either pre- or post-intervention (for single-group studies) or between intervention and control group at follow-up (for comparative trials).15 In cases where data were not included in the original manuscript (n = 3), we contacted study authors to request information for SMD calculations.16–18 Only 1 study team was able to provide additional information.18 Where SMDs were not calculated and for studies reporting descriptive outcomes, results are presented as described in the original publication. Given the heterogeneity of interventions and outcomes across the reviewed studies, SMDs were pooled using random effects models only when outcomes of at least 3 studies overlapped. All data pooling was conducted using Stata SE version 15.0 (StataCorp, LLC).
Included studies were assigned quality ratings based on the Grading Recommendations Assessment Development and Evaluation approach, which considers study design, bias, precision, and consistency of results.19,20 Disagreements between the 3 reviewers regarding quality (n = 6) were discussed until consensus was reached. The review was registered with the International Prospective Register of Systematic Reviews (#CRD42018082622).
RESULTS
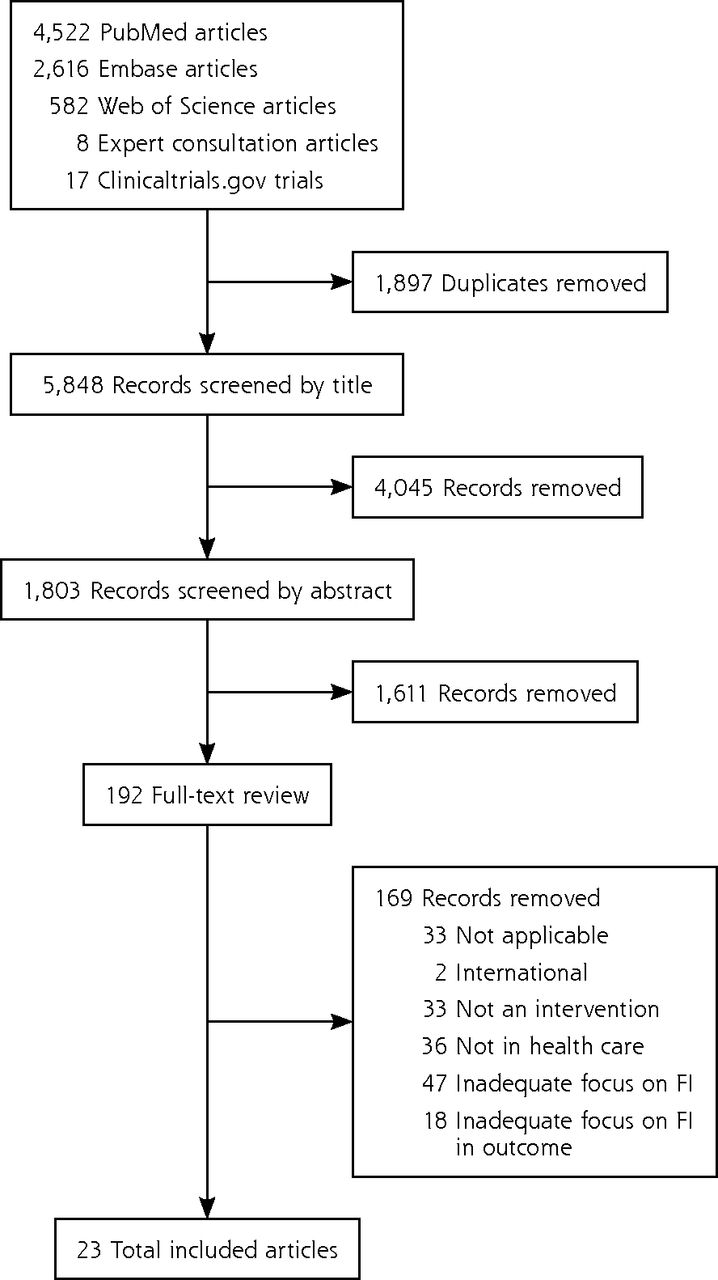
The initial database extraction yielded 5,848 unique articles; 192 underwent full-text review. Twenty-three unique articles met all inclusion criteria (Figure 1). There were 2 randomized control trials (RCT) (9%),16,21 1 cluster RCT (4%),22 2 quasi-experimental studies (9%),17,18 3 matched cohort studies (13%),23–25 and 8 single group, pre-/post- studies (35%).26–33 The remainder of the studies had descriptive, mixed methods, or qualitative designs (n = 7, 30%). Some articles focused on specific patient populations: 9 studies evaluated interventions targeting adult caregivers of pediatric patients (39%),16,21,22,28,29,31,34–36 1 targeted adolescents (4%),37 2 focused on pregnant women (9%),18,24 5 focused on patients with diabetes27,30,32,33,39 or another chronic condition25 (22%), and 1 focused on patients with cancer (4%).38 Seventeen studies (74%) were considered low17,26,28,30,31,32,37 or very low quality18,27,29,33–36,38–40 and 6 (26%) studies were rated moderate quality.16,21–25

Study selection flow diagram.
FI = food insecurity.
Interventions fell into 2 categories based on the food-related resources or assistance provided. One group included 12 studies (52%) that described education and/or referral interventions. These provided information for patients about food resources16,22,27,30,35,40 or more actively connected them to referral services through a navigator or other lay staff person.21,24,28,29,34,37 We combined passive (resource information provided) and active (assistance contacting resource) referral interventions into 1 category as results were too heterogenous to make meaningful comparisons between the 2 referral types. A second group included 10 studies (43%) examining interventions that provided food or food vouchers in addition to resource referrals17,18,25,26,31–33,36,38,39 and 1 study that provided food without referrals to community food resources.23
Included studies examined outcomes ranging from: (1) process outcomes (eg, number of patients referred), (2) food security status, (3) health, (4) health behaviors and self-efficacy, (5) health care utilization and/or cost, and (6) patient/caregiver perception of intervention acceptability. No studies reported provider outcomes (eg, provider attitudes or behavior change) related to interventions. Results are summarized below. Tables 1–3 include additional details.
Types of Food Insecurity Interventions and Quality Scores for Included Studies (N = 23)
Process Outcomes of Interventions to Address Food Insecurity in Health Care Settings (N = 17)
Non-Process Outcomes of Interventions to Address Food Insecurity in Health Care Settings (n = 11)
Process Outcomes
All of the referral-based studies included process outcomes (n = 12, 52%). Some described rates of food resource referrals; others described either program enrollment or use of resources. Rates of patients receiving referrals as a result of the intervention ranged from 30% to 75% (Table 2).16,22,27,29,35,40 In 2 RCTs, medical providers were more likely to provide food referrals to families who were asked about social needs (by a research assistant16 or self-completed form22), compared with families who were not (SMD = 1.42, 95% CI, 0.76-2.0816 and SMD = 0.67, 95% CI, 0.36-0.9822). A separate RCT showed no difference in food resource interest or use between control group participants (patients who received as needed social work referrals) compared with intervention group participants (patients who received additional navigation support with referrals, including to food resources) (SMD = 0.18, 95% CI, –0.08 to 0.43).21
Other studies reported on rates of food program enrollment or utilization.* One study found only modest effects of a waiting room–based intervention on patient enrollment in food-related resources (Table 2).22 Three other studies (13%) reported on change in patients’ use of food resources and described moderate increases in food resource use (pooled SMD = 0.54, 95% CI, 0.31-0.78; Table 2 & Figure 2).26,28,30 These studies were particularly vulnerable to selection bias, given study design.
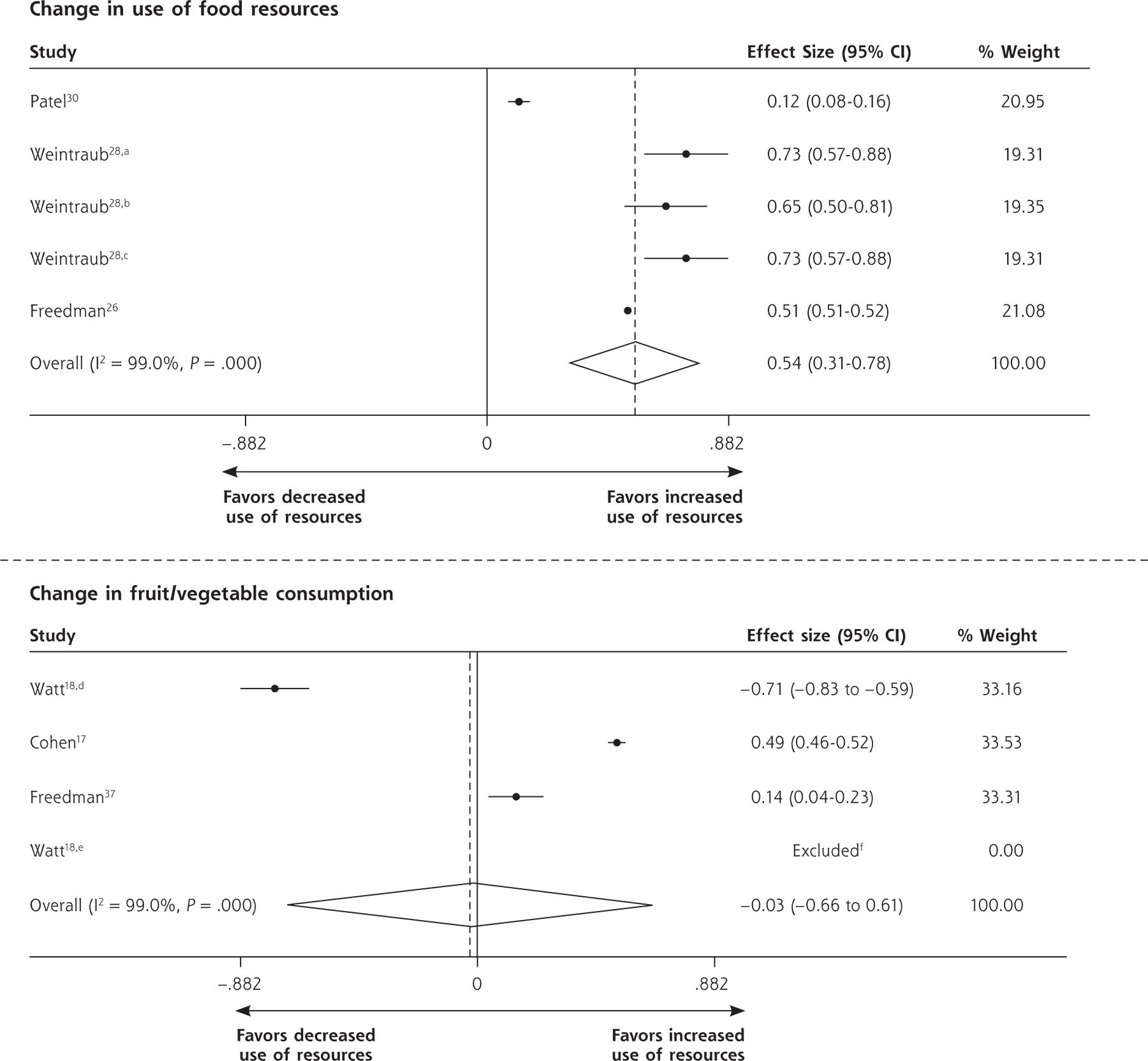
Forest plots for individual and pooled SMDs by study outcomes using random effects models.
CalWORKS = Californial work opportunities and responsibilities to kids program; SMD = standard mean difference; WIC = women, infants, and children supplemental nutrition assistance program.
aChange in receipt of WIC.
bChange in receipt of CalWORKS.
cChange in receipt of food stamps.
dChange in vegetable consumption.
eChange in fruit consumption.
f95% CI and variance not calculable as mean gain for control group was zero. Note: Weights are from random effects analysis.
Food Security Status Outcome
Two studies (9%) indirectly reported post-intervention patient food security status; neither used a validated screening tool to assess FI. One referral-based study found that post-intervention, 58% of patients (n = 7) reported their food-related concerns had resolved.37 In a qualitative study, caregivers of pediatric patients (n = 32) reported improved access to fresh fruits/vegetables after the clinic introduced an on-site farmers market and began distributing food/vouchers.36
Health Behavior and Self-Efficacy Outcomes
Four studies (17%) examined changes in fruit/vegetable intake.17,18,33,36 Pooling effect sizes for the 3 quantitative studies showed no intervention effect (pooled SMD = –0.03, 95% CI, –0.66 to 0.61; Figure 2),17,18,33 though in qualitative interviews, caregivers of pediatric patients reported increased consumption of fresh fruits/vegetables after participating in a food/voucher program.36
One referral-based study examined intervention impacts on diabetes self-efficacy scores in diabetic patients aged 60 years or older.27 There were no significant effects of the intervention on self-efficacy scores at 3-month follow-up (Table 3).
Health Outcomes
Five studies (22%) reported on patient health outcomes. Each study examined different metrics. One referral program in pregnant women attending an obstetrics clinic found a small improvement in blood pressure control during pregnancy.24 A separate prenatal nutrition intervention included general nutritional information, cooking classes, and distribution of vouchers for fruits/vegetables at a local farmers market.18 The evaluation showed no significant effect on infant or maternal outcomes18 (Table 3).
In another study, families with infants aged 12 months or younger that screened positive for FI (or met other eligibility criteria such as clinician concern for FI risk or failure-to-thrive) were provided supplemental formula, educational materials, and as-needed referrals to social work, medical-legal partnerships, or food pantries.31 Infant recipients of these resources were compared with non-recipients whom the authors did not identify as being eligible for the program and who were statistically significantly less likely to be publicly ensured, African American, or male. The intervention showed small but significant effects on health indicators including weight-for-length percentile, blood lead level, and developmental screening scores on the Ages & Stages Questionnaire.31
Two studies evaluated an intervention that provided vouchers for an onsite farmers market.25,32 In 1, adults with uncontrolled type 2 diabetes were offered health education and nutrition counseling.32 The authors found no effect on weight or blood pressure, but a small effect on lowering hemoglobin A1c. The second study in this group provided vouchers through a nutritionist to patients with obesity, hypertension, and/or type 2 diabetes and found a small but significant effect of the intervention on lowering body mass index compared with matched controls25 (Table 3). None of the studies that described health effects also examined FI outcomes, so we could not assess whether changes in food security mediated changes in health outcomes.
Health Care Utilization and Cost Outcomes
Two studies (9%) reported on health care utilization, 1 of which also examined cost. In 1 of these studies, infants enrolled in a nutrition support program showed small but statistically significant changes in emergency department use and receipt of preventive care services/visits compared with infants not in the program (that also had fewer social risk factors at baseline).31 A study of direct food provision was the only included study to examine health care costs.23 In that intervention, Medicaid/Medicare dual eligible patients were provided either medically tailored or nontailored meal deliveries. Health care utilization outcomes in each intervention group were compared with matched controls. Patients who received medically tailored or nontailored meals had fewer ED visits and less use of emergency transportation, while only those receiving medically tailored meals had fewer inpatient admissions. Both meal program groups had lower medical spending than the control group, with highest savings in the medically tailored meal group (Table 3).
Caregiver Acceptability
One study reported on acceptability of a food/voucher intervention to adult caregivers of pediatric patients.36 This qualitative work explored families’ experiences after a clinic relocated to the same building as an urban farmers market. The authors reported that caregivers appreciated the food/voucher program and preferred vouchers over preprepared bags of food.
DISCUSSION
Despite the rapid increase in health care–based FI interventions,11,41,42 this is the first systematic evidence review of health care delivery–based FI interventions. Of the 23 studies that met inclusion criteria, the majority exclusively described process metrics. These studies reported a wide range in food program referral and enrollment rates. When studies reported the effects of FI interventions on actual use of resources (not just enrollment), pooled analyses revealed moderate size positive effects. These studies rarely explored reasons that referrals did not consistently result in program use.
In pooled results from studies that provided food or food vouchers, we found no effects on fruit and vegetable consumption. It is possible that dose or duration of intervention was insufficient to impact consumption or that follow-up periods were either too short or long to observe changes. Challenges in using dietary recall to capture fruit/vegetable intake also may have biased to the null.43 Few studies evaluated health impacts of FI-related interventions. The studies examining either health or utilization outcomes had small effect sizes. Variability in health or utilization measures across studies prevented pooling.
The majority of studies in the review (17/23) were of low or very low quality. Lower quality studies either had no comparison group or compared outcomes to a group significantly different from the intervention group. Many studies had low enrollment and follow-up, limiting statistical power and generalizability. In general, moderate quality studies reported less positive outcomes than lower quality studies. Higher quality studies examining health and utilization/cost outcomes are needed to inform future FI investments.
Findings from this review of health care–based FI interventions should be interpreted with caution. First, both the overall low quality of studies in this review and wide range of populations and settings make it difficult to draw generalizable conclusions. Second, heterogeneity of interventions and outcomes hindered comparisons across studies. Pooling was done when appropriate. Different metrics were used across studies, even when similar outcome categories were included (eg, process, health, or cost outcomes), making it impossible to compare overall impacts of these programs.
Third, we restricted our review to peer-reviewed publications and US health care–based studies; we may have excluded gray literature or international findings that could have important implications for this rapidly growing area of research. Health systems like ProMed-ica44 and Geisinger45 both have robust programs to screen for FI and provide healthy food to patients, but have not published peer-reviewed studies on program impacts. Restricting our review to health care–based studies also excluded potentially informative FI interventions that examine health outcomes but take place in non–health care settings.46,47
Finally, we included studies of interventions that in some cases targeted food in addition to other social determinants of health, making it difficult to directly link multi-faceted interventions with food outcomes. Food insecurity often exists alongside other material deficits related to poverty; it may be artificial to isolate the effects of addressing FI from the effects of addressing other social factors (eg, housing instability).
Despite these limitations, this review offers a timely and relevant summary of evidence in this field across diverse patient populations, health care settings, and types of interventions. It also highlights critical evidence gaps that should guide future research. Though many health care settings are actively exploring ways to reduce patient FI to improve patient health and well-being, there is currently little rigorously conducted research in this area. Early evidence suggests that these programs may help patients better connect with food resources, but more research is needed to better explore impacts on health, health care utilization, and cost.
Acknowledgments
We gratefully acknowledge Seth Berkowitz, MD, Alicia Cohen, MD, MSc, Stephanie Ettinger de Cuba, MPH, Megan Sandel, MD, MPH, Rich Sheward, MPP, and John Steiner, MD, MPH, for reading earlier drafts of this manuscript and Holly Wing, MA, for assistance developing the search protocol.
Footnotes
Conflicts of interest: authors report none.
↵* References 22, 24, 26, 28, 30, 34, 37-40.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/17/5/436.
Funding support: J.M.T., C.F., and L.M.G. were supported by the Kaiser Foundation Health Plan, Inc. Kaiser Foundation Health Plan, Inc had no role in study design; collection, analysis, or interpretation of data; writing the report; or the decision to submit the report for publication. E.H.D. was supported by a fellowship training grant, National Research Service Award (NRSA) T32HP19025. The manuscript’s contents are solely the responsibility of the authors and do not represent the official views of the Kaiser Foundation Health Plan, Inc, or the NRSA.
Supplemental materials: Available at http://www.AnnFamMed.org/content/17/5/436/suppl/DC1/.
- Received for publication November 30, 2018.
- Revision received March 7, 2019.
- Accepted for publication April 4, 2019.
- © 2019 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clusters of Health-Related Social Needs Among Adult Primary Care Patients
- Doctors have an ethical obligation to ask patients about food insecurity: what is stopping us?
- Mise en {oelig}uvre dinterventions sociales en soins de sante primaires
- Implementing social interventions in primary care
- Utilization Patterns of a Food Referral Program: Findings from the Mid-Ohio Farmacy
- Food Insecurity Is an Independent Risk Factor for Depressive Symptoms in Survivors of Digestive Cancers
- Does the effect of lifestyle intervention for individuals with diabetes vary by food insecurity status? A preplanned subgroup analysis of the REAL HEALTH randomized clinical trial
- Do Patients Want Help Addressing Social Risks?