
Abstract
PURPOSE Metabolic, hormonal, and hemostatic changes associated with pregnancy loss (stillbirth and miscarriage) may contribute to the development of cardiovascular disease (CVD) in adulthood. This study evaluated prospectively the association between a history of pregnancy loss and CVD in a cohort of postmenopausal women.
METHODS Postmenopausal women (77,701) were evaluated from 1993–1998. Information on baseline reproductive history, sociodemographic, and CVD risk factors were collected. The associations between 1 or 2 or more miscarriages and 1 or more stillbirths with occurrence of CVD were evaluated using multiple logistic regression.
RESULTS Among 77,701 women in the study sample, 23,538 (30.3%) reported a history of miscarriage; 1,670 (2.2%) reported a history of stillbirth; and 1,673 (2.2%) reported a history of both miscarriage and stillbirth. Multivariable-adjusted odds ratio (OR) for coronary heart disease (CHD) for 1 or more stillbirths was 1.27 (95% CI, 1.07–1.51) compared with no stillbirth; for women with a history of 1 miscarriage, the OR = 1.19 (95% CI, 1.08–1.32); and for 2 or more miscarriages the OR = 1.18 (95% CI, 1.04–1.34) compared with no miscarriage. For ischemic stroke, the multivariable odds ratio for stillbirths and miscarriages was not significant.
CONCLUSIONS Pregnancy loss was associated with CHD but not ischemic stroke. Women with a history of 1 or more stillbirths or 1 or more miscarriages appear to be at increased risk of future CVD and should be considered candidates for closer surveillance and/or early intervention; research is needed into better understanding the pathophysiologic mechanisms behind the increased risk of CVD associated with pregnancy loss.
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of mortality for women in the United States, with 24% of female deaths attributed to CVD in 2009.1,2 Although traditional risk factors for CVD, are associated with increased CVD risk in both men and women, unique risk factors for women related to reproductive history have only recently been considered as potentially important.2 Growing evidence suggests that the metabolic, hormonal, and hemostatic pathway alterations that are associated with pregnancy loss may contribute to the development of coronary heart disease in adulthood.3–5 Women with adverse pregnancy outcomes, such as preeclampsia, preterm delivery, low birth weight, intrauterine growth restriction, and pregnancy loss (including miscarriage and stillbirth), may be at risk of metabolic and vascular diseases later in life.6,7 Additionally, genotypes and phenotypes underlying vascular disease may also underlie fetal programming.5
At present, the mechanisms underlying the association of miscarriage and stillbirth with CVD are unclear, although there appears to be a relationship between the metabolic syndrome, abnormal implantation, and endothelial dysfunction.8,9 Specifically, it has been suggested that the endothelial dysfunction resulting from systemic inflammatory processes may be involved.10 The resulting vascular pathology may thus contribute to both poor placentation during pregnancy (resulting in pregnancy loss) and an increased likelihood of CVD.10 Recently the 2011 American Heart Association guidelines have incorporated pregnancy complications as a risk factor for CVD in women based on the growing evidence suggesting an association.2 These guidelines, however, did not address the long-term cardiovascular implications of miscarriage.
A limited number of studies have evaluated pregnancy loss and risk of development of future CVD, but the findings have been inconsistent, with some finding no clear association11,12 and others suggesting an increased risk between pregnancy loss and CVD.3,10,13,14 The Women’s Health Initiative (WHI) population provides a unique opportunity to be able to examine the association of miscarriage and stillbirth in a diverse, geographically dispersed cohort of women with adjudicated cardiovascular events, including fatal and nonfatal myocardial infarctions and stroke outcomes.
METHODS
The Study Population
The study population has been described in detail previously.15 Briefly, WHI has both clinical trial and observational study arms.15,16 The observational study component was a prospective cohort study that enrolled 93,676 women aged 50 to 79 years from 1993 to 1998 at 40 clinical centers throughout the United States. Women were eligible if they were postmenopausal, unlikely to relocate or die within 3 years, were not enrolled in the WHI Clinical Trial, and were not participating in any other clinical trial. Women from the observational study were observed through August 2009 depending on when they enrolled in the study. Participants were excluded from the analyses for the following reasons: having had CVD at baseline, having never been pregnant, and having missing reproductive data.
Data Collection
Women completed screening and enrollment questionnaires by interview and self-report. Baseline personal information, medical history, medication use, and health-related behaviors were assessed. Women underwent a physical examination and provided blood specimens and anthropometric and blood pressure measurements. Participants were asked whether a physician had ever told them that they had high blood pressure, diabetes, high blood glucose (nonpregnant), or high cholesterol that required taking medication. Baseline characteristics have been described in detail previously.15–18 Variables examined included smoking, alcohol consumption, family history of early coronary heart disease (CHD), depression, recreational physical activity, and metabolic equivalent task scores (computed as the product of days per week, minutes per day, and the metabolic equivalent task (MET) value for each activity in MET-hours per week).19 Women were considered to have CVD if they self-reported a history of myocardial infarction, stroke, angina, congestive heart failure, coronary revascularization, or peripheral arterial disease. Early hypertension was defined as self-reported hypertension that occurred in women aged less than 40 years, because information on gestational hypertension was not obtained. Hypertension was defined as hypertension that developed in women after the age of 39 years and was based on self-report and medication use. White blood cell count was dichotomized as ≤6,700/μL and >6,700/μL.20 Regarding the women’s reproductive history, women were first asked about gravidity, which was defined as the number of times the woman was pregnant. The women were asked about the number of “live births, miscarriages, tubal (ectopic) and abortions.” Parity was based on the question, “Have you had a pregnancy lasting 6 months or more?” Pregnancy loss was based on the reported number of spontaneous miscarriages and still births. Nulligravida women reported no pregnancies.
Follow-up
Follow-up activities consisted of mailings sent annually from the Clinical Coordinating Center and a clinical center visit at 3 years after enrollment to update selected baseline data, obtain additional risk factor data, and collect a blood specimen. Up to 2 additional mailings and telephone contacts as necessary with participants or proxies were conducted by the clinical center staff for nonresponders. The annual follow-up response rate was greater than 94% each year for those who were due for a follow-up contact. A participant was considered lost to follow-up if there was no outcomes information from the participant for 24 months.
Outcome Ascertainment
All outcomes were physician adjudicated; they were initially identified through annual follow-up contacts and subsequently verified through medical records and death certificates.21 Newly diagnosed cardiovascular events were identified on the basis of annual mailed follow-up questionnaires and medical records review. Study physicians with no knowledge of the self-reported risk-factor status reviewed the records. The diagnosis of myocardial infarction was confirmed if data in the hospital record met standardized criteria of chest pain or equivalent, diagnostic electrocardiographic changes, and/or elevated cardiac enzyme levels. Angina was confirmed by hospitalization and confirmatory evidence on angiography, diagnostic stress test, or diagnosis by a physician and medical treatment. Fatal CHD was considered confirmed if there was documentation in the hospital or autopsy records or if CHD was listed as the cause of death on the death certificate and evidence of previous CHD was available. Total CHD was defined as myocardial infarction, definite CHD death, revascularization, or hospitalized for angina. Treatment with coronary revascularization or percutaneous interventions was confirmed by documentation of the procedure in the medical record. Ischemic stroke was confirmed by medical record documentation of rapid onset of a neurologic deficit consistent with stroke and lasting at least 24 hours or until death.
Statistical Analysis
All analyses were conducted using SAS 9.2 (SAS Institute, Inc).22 Descriptive statistics were used to summarize variables, as well as detect outliers and missing values. Normality of the distribution was examined with a normal probability plot, when applicable. The association of participants’ baseline characteristics and pregnancy loss was evaluated using χ2 tests, 2-sample t tests, or non-parametric tests, when applicable. Multivariable logistic regression models were used to calculate adjusted odds ratios (ORs) to assess the independent associations of pregnancy loss (stillbirth, miscarriage) with CHD and stroke after controlling for sociodemographic variables, traditional risk factors for CVD, and other potential confounders. Confounders included age, race, education, smoking status, gravidity, family history of myocardial infarction, history and duration of hypertension, diabetes, hyperlipidemia, body mass index, waist-to-hip ratio, aspirin use, depression, and white blood cell count. We also adjusted for other covariates (marital status, diuretic use, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use, calcium channel blocker use, alcohol use, and physical activity). Models were adjusted for stillbirths and miscarriages in the analyses to be able to evaluate the independent effects.
A full model was initially developed using all of the available exploratory variables identified based on clinical judgment, previous literature, and univariate analyses. The final models were subsequently developed using a backward selection algorithm and included each clinical relevant predictor and covariates with a P value of ≤.10. In addition, we examined whether the associations between total CHD and stroke with pregnancy loss were explained by or mediated through development of diabetes, hypertension, increased waist-to-hip ratio, or a marker of inflammation (white blood cell count). Separate models with and without adjustment for these covariates were developed and compared.
RESULTS
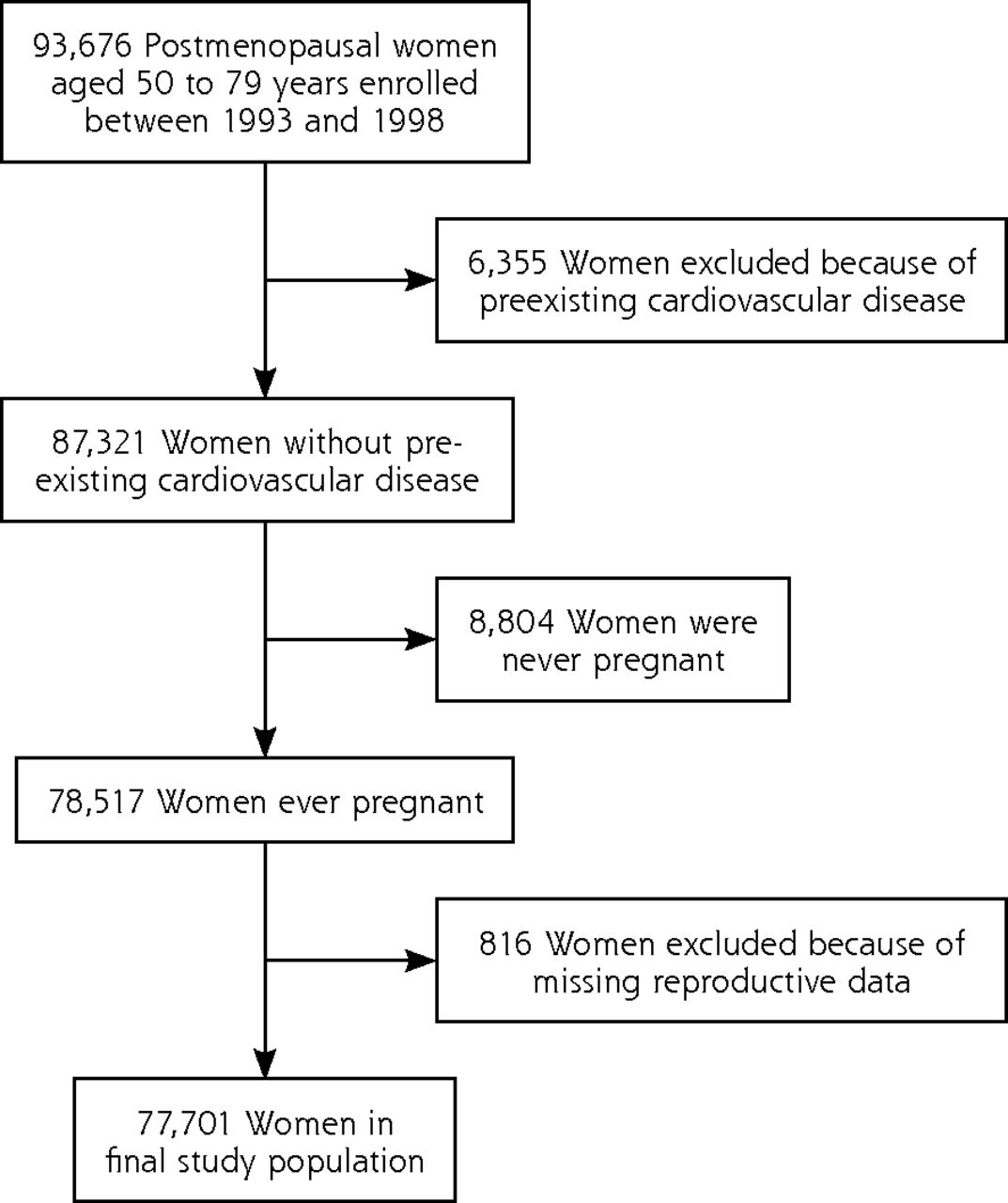
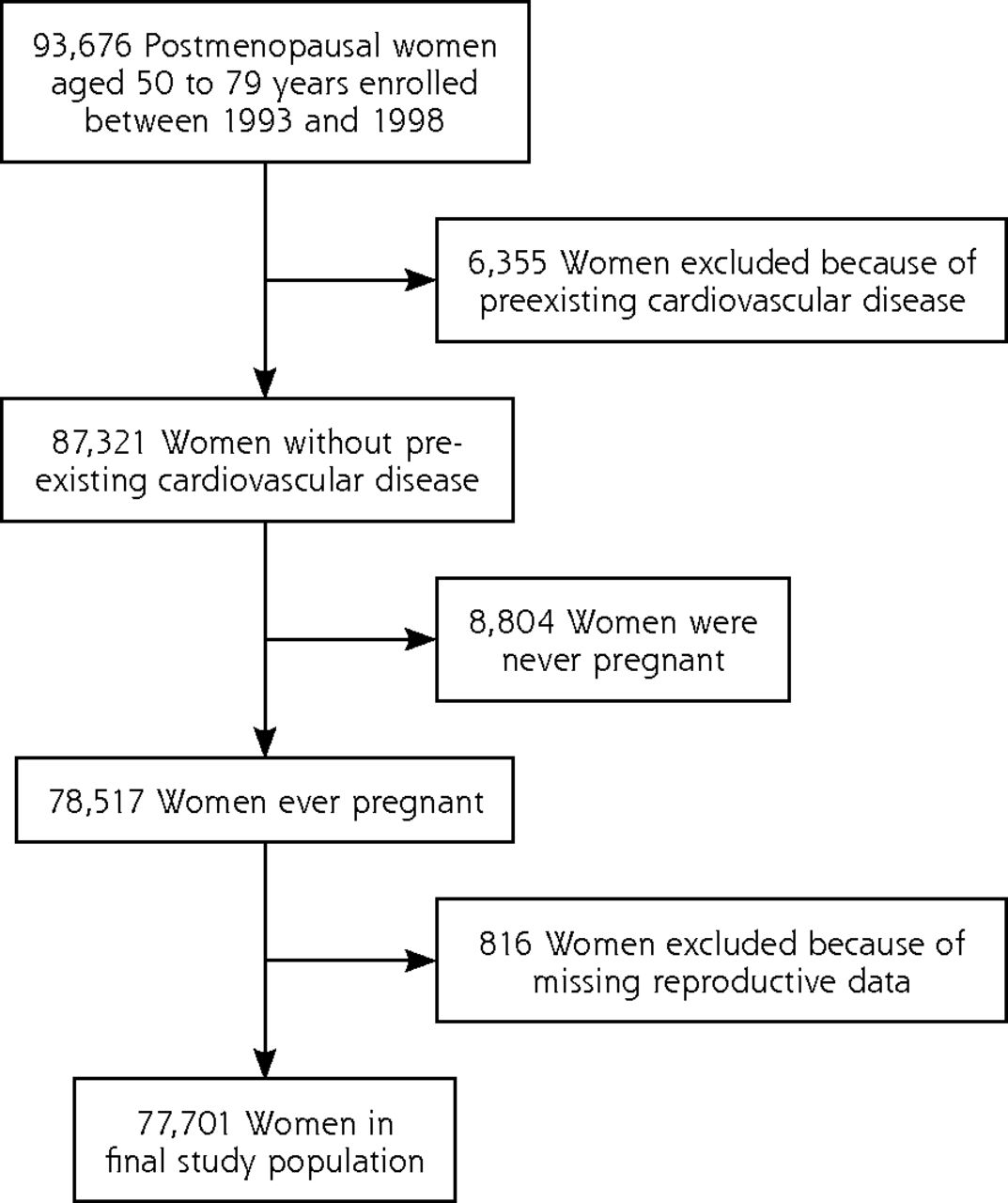
Of the 93,676 postmenopausal women, 50 to 79 years of age, who were enrolled between 1993 and 1998, 6,355 women had CVD, 8,804 women were never pregnant, and 816 women had missing reproductive data. Some women had more than 1 exclusion criterion, yielding a final sample of 77,701 (Figure 1). Among the 77,701 women in the study sample, 23,538 (30.3%) reported a history of miscarriage; 1,670 (2.2%) reported a history of stillbirth; and 1,673 (2.2%) reported a history of both miscarriage and stillbirth. The follow-up period ranged from 0.2 years to 10.6 years with a mean of 7.7 years. There were 1,966 (2.5%) clinical myocardial infarction events, 2,439 (3.1%) CHD events, and 1,503 (1.9%) ischemic stroke events. Of the 2,439 patients with CHD, 925 had revascularization (37.9%), and 139 had angina (5.7%).
Women’s Health Initiative (WHI) participants included in the current study
The baseline characteristics of the women who had a pregnancy loss (miscarriage or stillbirth) were compared with women who did not have any pregnancy loss in Table 1. Women with a history of stillbirth were more likely to be older, more likely to have a higher gravidity, and less likely to consume alcohol. Women who had a history of both miscarriage and stillbirth were more likely to be a current smoker, have a higher body mass index and waist-to-hip ratio, and have a higher systolic blood pressure. These women were also more likely to have a history of early hypertension, diabetes, and depression, as well as a history of baseline antihypertensive, lipid-lowering, and diabetic medication use. In addition, more African-American (14.8%) and Hispanic (7.9%) women reported a history of stillbirth or a history of both stillbirth and miscarriage (15.4% for African-American and 9.2% for Hispanic women) compared with all other women.
Baseline Characteristics of Observational Study Women from the Women’s Health Initiative
To test for interactions with adequate power, we examined the association between pregnancy loss and risk of total CHD, as shown in Table 2. The multivariable-adjusted odds ratio (OR) was OR = 1.19 (95% CI, 1.08–1.32) for 1 miscarriage and OR = 1.18 (95% CI, 1.04–1.34) for 2 or more miscarriages compared with none. For stillbirth, the multivariable-adjusted OR = 1.27 (95% CI, 1.07–1.51). For the multivariable models, interactions between pregnancy loss (separate models for miscarriage and stillbirth) and diabetes, hypertension, lipid levels, and race were also examined but were not significant and were therefore not included in the final models.
Unadjusted, Age-Adjusted, and Multivariable-Adjusted Odds Ratios of the Association Between Pregnancy Loss and Risk of Total Coronary Heart Disease
Unadjusted, age-adjusted, and multivariable-adjusted odds ratios of the association between pregnancy loss and risk of ischemic stroke are displayed in Table 3. For 1 miscarriage, the age-adjusted OR = 1.09 (95% CI, 0.97–1.24), and for 2 or more miscarriages OR = 1.14 (95% CI, 0.97–1.33) compared with none. For 1 miscarriage the multivariable-adjusted OR = 1.05 (95% CI, 0.91–1.19), and 2 or more miscarriages OR = 0.93 (95% CI, 0.77–1.19) compared with none. For stillbirth, the age-adjusted OR = 1.29 (95% CI, 1.03–1.60) and the multivariable-adjusted OR = 1.13 (95% CI, 0.89–1.43).
Unadjusted, Age-Adjusted, and Multivariable-Adjusted Odds Ratios of the Association Between Pregnancy Loss and Risk of Ischemic Stroke
DISCUSSION
This study suggests that women with a history of pregnancy loss (miscarriage or stillbirth) have an increased risk of total CHD after adjusting for traditional cardiovascular risk factors and the number of pregnancies. The association between pregnancy loss and CHD appears to be independent of hypertension, body mass index, waist-to-hip ratio, and white blood cell count. Moreover, the risk appears greater among women with a history of stillbirth than among women with a history of miscarriage. Among women with a history of miscarriage, risk of CHD death was similar for women who had 1 or more miscarriages. In this study, we did not find a significant association of ischemic stroke with pregnancy loss.
Despite research interest in the relationships between pregnancy-related factors (ie, birth weight, preeclampsia, gestational diabetes, preterm birth) and risk of CVD,5,6,23,24 limited studies have examined the association of pregnancy loss and subsequent risk of CVD.3,11,14,25–27 Several early studies reported an association of miscarriage and/or stillbirth and risk of future CVD.13,25,26 Although suggestive, these studies were not conclusive, because they were either descriptive, case-control, or cross-sectional studies, or they did not adjust for potential confounders. In a nationally representative cross-sectional sample of 3,937 Finnish women aged 30 to 99 years, investigators examined the association of miscarriage with risk of CHD.13 They reported that after adjusting for number of previous pregnancies, age, education, smoking, body mass index, waist-to-hip ratio, physical activity, systolic and diastolic blood pressure, fasting blood glucose, and total and low-density lipoprotein cholesterol, women with a history of miscarriage had a higher, although not significant, risk of myocardial infarction (OR = 1.3; 95% CI, 0.6–2.4) than other women. They reported that after stratifying by age-groups, women aged 50 to 74 years had a stronger association of miscarriage with myocardial infarction (OR = 1.5; 95% CI, 1.1–4.2), findings similar to ours in postmenopausal women.
In a recent prospective cohort study of 11,518 women, aged 35 to 66 years, who participated in the European Prospective Investigation into Cancer and Nutrition (EPIC), investigators examined the association of pregnancy loss (miscarriage and stillbirth) with risk of myocardial infarction and stroke.3 Among women with recurrent miscarriages (more than 3), the fully-adjusted HR for risk of myocardial infarction was significant (5.06; 95% CI, 1.26–20.29). Similarly, the risk of myocardial infarction was also significant (fully adjusted hazard ratio was 2.32; 95% CI, 1.19–4.50) for women with a history of stillbirth, although the risks of myocardial infarction were higher for women in the EPIC study compared with our findings. Moreover, the higher risk of CHD for women with a history of miscarriage and stillbirth in the EPIC study may be related to our having eliminated women with preexisting CVD, which may have eliminated those with premature coronary heart disease and therefore those in whom the association would be the greatest. Additionally, both our findings and those of the EPIC study did not find an association between history of pregnancy loss and ischemic stroke. Of interest was that the stillbirth rate for our cohort was similar (2.2%) to the rate for the EPIC study (2%).3
More recently, 2 additional studies have reported an association of pregnancy loss as a risk factor for future cardiovascular disease. Oliver-Williams et al14 performed a meta-analysis that examined the association between miscarriage and future CVD in healthy women. The meta-analysis included 10 studies (517,504 women in the CHD meta-analysis and 134,461 women in the CVD meta-analysis). They reported that women with a history of miscarriage had a greater odds of developing CHD (OR = 1.45; 95% CI, 1.18–1.78) but not with CVD (OR = 1.11; 95% 0.72–1.69). In a large population-based cohort study of more than 1 million women,10 women with a history of miscarriage and stillbirth had increased rates of myocardial infarction, cerebral infarction, and renovascular hypertension compared with women with no history of miscarriage or stillbirth. Similar to our findings, the risks of myocardial infarction were greater for stillbirths than for miscarriages. Ranthe et al, however, also reported a significant association of pregnancy loss and stroke, which may be due to the greater number of stroke events (4,053 vs 1,503 for WHI) and ascertainment of history of pregnancy loss based on Medical Birth Register data rather than self-reports used in most other studies.14,28,29
There are several limitations that should be mentioned. Pregnancy loss was based on self-report, and self-reports of miscarriage and stillbirth could be subject to misclassification bias. Additionally, self-reports of miscarriage may be underestimated, because women may be unaware of spontaneous early miscarriages. In one study of 754 women that assessed self-reported reproductive histories vs medical records, however, Olson et al reported high reliability between the 2 data sources in terms of number of live births (κ= 1.0), number of previous pregnancies (κ = 0.9), and number of miscarriages (κ=0.7).30 Additionally, our rates of miscarriage (30%) and stillbirth (2.2%) were similar to those of Kharazmi and colleagues,3 who reported rates of 25% for miscarriages and 2% for stillbirths. Another potential concern was the lack of biomarker data. Although high-sensitivity C-reactive protein findings were not available at the time of our analyses, the white blood cell count, another measure of systemic inflammation that has been reported to independently predict CHD and all-cause mortality in postmenopausal women, was assessed in this study.20 The white blood cell count was dichotomized to >6.7 × 109/L and ≤6.7 × 109/L, which has been found to identify high-risk individuals who were not identified by traditional CHD risk factors.20 Additionally, although depression in postmenopausal women was more prevalent in those with a history of stillbirth and miscarriage, prospective data would be required to discern whether depression is part of a causal pathway. Information on weeks of gestation and age at pregnancy loss was not available. We were therefore unable to examine the association with early or late pregnancy loss separately, nor were we able to examine the association based on age of the women at time of pregnancy loss. We chose to control for the number of pregnancies each woman had experienced, but doing so may not fully elucidate whether there is an association of pregnancy itself with the risk for cardiovascular disease. Finally, given the observational nature of the study, we cannot prove that the observed associations are causal; residual confounding could affect the observed associations.
The strengths of the present study include the prospective study design and the large diverse cohort of women, which provided adequate power to assess risk of relatively rare events, stillbirths, the ability to evaluate the “dose” response for multiple miscarriages, and the large number of ischemic stroke cases (1,503). Another notable strength was that we had a valid assessment of CVD outcomes, as well as a wide range of potential confounders available to evaluate.
These data, derived from a large diverse cohort of initially healthy postmenopausal women, showed that women with a history of pregnancy loss appear to be at increased risk of future CHD but not ischemic stroke. Although we cannot determine the mechanism of these associations, findings from this study, and more recently the study by Ranthe et al,10 suggests a shared cause for pregnancy loss and CHD that requires further investigation into better understanding the pathophysiologic mechanisms behind the increased risk (ie, changes in endothelial function, insulin resistance, inflammation, and hypercoagulable states). Additionally, biomarker data are also needed so that we can examine potential biologic pathways for homocysteine, antiphospholipid antibodies, VEGF-A (vascular endothelial growth factor-A), PAI-1 (plasminogen activator inhibitor-1), high-sensitivity C-reactive protein, glucose, insulin, and flow-mediated dilation to help us further understand this association. Furthermore, future studies need to address whether the association of pregnancy loss and CHD is independent of potential confounders.
Until recently, prenatal loss was not routinely considered to be a risk factor for development of future CVD. The American Heart Association recently recommended2 adding reproductive history of pregnancy loss as a risk factor for CHD. Given that 15% of CVD events in women occur in the absence of conventional risk factors, reproductive history of pregnancy loss may be a potentially clinically useful predictive marker of CVD risk.31 Our findings, although not conclusive, suggest that women with a history of miscarriage or a single stillbirth may be at increased CVD risk and should be considered candidates for closer surveillance and/or early intervention by their primary care physician so that risk factors can be carefully monitored and controlled (including monitoring of CVD risk factors—diabetes, hypertension, cholesterol, obesity, smoking, and diet).
Acknowledgments
We thank the Women’s Health Initiative investigators, staff, and study participants for their outstanding dedication and commitment. A full listing of Women’s Health Initiative investigators can be found at https://cleo.whi.org/researchers/Documents%20%20Write%20a%20Paper/WHI%20Investigator%20Long%20List.pdf.
Footnotes
-
Conflicts of interest: authors report none.
-
Financial support: The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, US Department of Health and Human Services, through contracts N01WH22110, 24152, 32100–2, 32105–6, 32108–9, 32111–13, 32115, 32118–32119, 32122, 42107–26, 42129–32, and 44221.
-
Previous presentations: Parker DR, Lu B, Sands-Lincoln M, Eaton BB. History of pregnancy loss predicts coronary heart disease and peripheral vascular disease in postmenopausal women in the Women’s Health Initiative. American Heart Association, Scientific Sessions, Orlando, Florida, 2011.
- Received for publication June 25, 2013.
- Revision received February 12, 2014.
- Accepted for publication March 12, 2014.
- © 2014 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Infertility, recurrent pregnancy loss, and risk of stroke: pooled analysis of individual patient data of 618 851 women
- Elevated cardiovascular disease risk in low-income women with a history of pregnancy loss
- Pregnancy Loss and Cardiovascular Disease: A Nationwide Cohort Study
- Pregnancy-Related Risk Factors Are Associated With a Significant Burden of Treated Hypertension Within 10 Years of Delivery: Findings From a Population-Based Norwegian Cohort
- Preconception Blood Pressure Levels and Reproductive Outcomes in a Prospective Cohort of Women Attempting Pregnancy
- Pregnancy Loss and Carotid Intima-Media Thickness in Mexican Women
- History of Adverse Pregnancy Outcomes, Blood Pressure, and Subclinical Vascular Measures in Late Midlife: SWAN (Study of Women's Health Across the Nation)
- Reproductive Factors and Incidence of Heart Failure Hospitalization in the Womens Health Initiative
- Harnessing the Power of Pregnancy and Pregnancy-Related Events to Predict Cardiovascular Disease in Women
- Reproductive Risk Factors and Coronary Heart Disease in the Womens Health Initiative Observational Study
- In This Issue: Technical and Personal Systems, and Novel Risk Factors