
Abstract
PURPOSE The Canadian Primary Care Sentinel Surveillance Network (CPCSSN) is Canada’s first national chronic disease surveillance system based on electronic health record (EHR) data. The purpose of this study was to develop and validate case definitions and case-finding algorithms used to identify 8 common chronic conditions in primary care: chronic obstructive pulmonary disease (COPD), dementia, depression, diabetes, hypertension, osteoarthritis, parkinsonism, and epilepsy.
METHODS Using a cross-sectional data validation study design, regional and local CPCSSN networks from British Columbia, Alberta (2), Ontario, Nova Scotia, and Newfoundland participated in validating EHR case-finding algorithms. A random sample of EHR charts were reviewed, oversampling for patients older than 60 years and for those with epilepsy or parkinsonism. Charts were reviewed by trained research assistants and residents who were blinded to the algorithmic diagnosis. Sensitivity, specificity, and positive and negative predictive values (PPVs, NPVs) were calculated.
RESULTS We obtained data from 1,920 charts from 4 different EHR systems (Wolf, Med Access, Nightingale, and PS Suite). For the total sample, sensitivity ranged from 78% (osteoarthritis) to more than 95% (diabetes, epilepsy, and parkinsonism); specificity was greater than 94% for all diseases; PPV ranged from 72% (dementia) to 93% (hypertension); NPV ranged from 86% (hypertension) to greater than 99% (diabetes, dementia, epilepsy, and parkinsonism).
CONCLUSIONS The CPCSSN diagnostic algorithms showed excellent sensitivity and specificity for hypertension, diabetes, epilepsy, and parkinsonism and acceptable values for the other conditions. CPCSSN data are appropriate for use in public health surveillance, primary care, and health services research, as well as to inform policy for these diseases.
- primary health care
- chronic disease
- validation studies
- electronic health records
- sensitivity and specificity
INTRODUCTION
The continuing, worldwide use of electronic health records (EHRs) in primary care practices provides a potential source of clinical data. These data can improve our understanding of the epidemiology of disease and effectiveness of disease prevention and management through disease surveillance, primary care–focused health services research, practice evaluation, and quality improvement.1–4 EHRs provide clinical data not typically available from health administrative data sources or population surveys.5
The Canadian Primary Care Sentinel Surveillance Network (CPCSSN) has assembled Canada’s first national EHR data repository for primary care research and surveillance.1 Given the nature of EHR data, disease case definitions used in its analysis must accurately reflect diagnoses within the EHR before being used for either surveillance or research. The purpose of this study was to develop and validate EHR-based case definitions and case-finding algorithms used to identify 8 common chronic conditions found in primary care (chronic obstructive pulmonary disease [COPD], dementia, depression, diabetes, hypertension, osteoarthritis, parkinsonism, and epilepsy) against EHR-based diagnosis of these conditions by chart review.
METHODS
Study Sample
CPCSSN consists of 10 primary care research networks (PCRNs) across Canada with 475 participating primary care sentinel clinicians (family physicians and nurse practitioners) contributing quarterly data on more than 600,000 patients. All 10 PCRNs have received approval from their host institution research ethics boards, as well as Health Canada ethics approval for collecting this information. Our study included patient data extracted on June 30, 2012, from 6 of the 10 PCRNs. Four of the 10 networks were excluded for a variety of reasons, including being the pilot test site for this study and data collection problems. Each of the participating networks reviewed 400 patient charts, except in British Columbia, which had a smaller number of participating sentinel clinicians and accordingly reviewed 200 charts. Charts were randomly selected using an age-stratified method, with 90% of the charts drawn from those patients older than 60 years. In addition, 25 charts each for epilepsy and parkinsonism were chosen nonrandomly because of the lower prevalence rates of these diseases. The total sample of 2,200 charts from all the sites ensured a margin of error of less than 10% for all outcomes of interest, with the exception of epilepsy and parkinsonism.
Chart Review Procedures
Research assistants who were blinded to the algorithmic diagnosis of cases reviewed the charts. All reviewers were trained using a standard manual. A standardized electronic data abstraction tool was developed to extract anonymous information from patients’ charts and record the reviewers’ assessments in a consistent way. The manual, training procedures, and abstraction tool were based on those developed for a previous study on data validation in primary care practices.6 A pilot study conducted at one PCRN verified the feasibility of the method, refined the data collection tool, and identified issues with case definitions or audit procedures.4 Reviewers examined the entire electronic chart for evidence of the presence or absence of each of the 8 conditions under study. In circumstances where the reviewer was uncertain about the diagnosis, the study epidemiologist and a physician from the study team reviewed the chart. All chart review data were entered into an electronic database built using FileMaker Pro 11 (FileMaker, Inc).
Case Definitions
The CPCSSN case definitions were specifically developed for use in primary care contexts. The definitions use a combination of International Classification of Diseases, Ninth Revision (ICD-9) codes (used by primary care physicians for service billing purposes in Canada) and numeric and textual data (including spelling variants, etc) drawn from a number of sections within the EHR, including the problem and encounter diagnoses, billing, laboratory test results, and prescribed medications (Supplemental Appendix). The case definitions were constructed with guidance from published evidence and both general and specialist physicians, and required several revisions before validation and implementation using computerized case finding algorithms. Table 1 provides a description of the case definitions. Each is unique to the respective chronic condition and includes varying EHR data elements. The detailed case definitions are available from CPCSSN at http://www.cpcssn.ca/research-resources/case-definitions.
Summary of CPCSSN Case Definitions for 8 Index Conditions
Statistical Analysis
Sensitivity, specificity, and positive and negative predictive values (PPVs and NPVs) for each case definition were calculated. The data were summarized using 2 × 2 tables comparing the CPCSSN case definition diagnosis (either a case or noncase) with the chart review diagnosis (either a case or noncase) for each condition. Generalized estimating equations quantified the effect of clustering at the physician, site, or network level. The estimated intracluster correlation was then used to more accurately estimate the appropriate 95% confidence intervals for sensitivity, specificity, PPV, and NPV. For all metrics, the lower limit of the 95% confidence interval was considered the lower limit of the plausible range and was compared with standard cutoffs. Because acceptable limits for individual metrics need to be suited to the question of interest, we considered all measures above 70% acceptable, with any falling into the 70% to 80% range meriting additional investigation. All data were analyzed using the SAS 9.3 statistical platform (SAS Institute).
RESULTS
Overall Study Sample
In total, 1,920 patient charts were reviewed from regional PCRNs from the provinces of British Columbia, Alberta (2 PCRNs), Ontario, Nova Scotia, and Newfoundland. Collectively, these PCRNs included 126 sentinel clinicians from 33 practice sites, using 4 different EHR systems (Nightingale On Demand [Nightingale Informatix Corporation], PS Suite EMR [TELUS Health], Wolf EHR [TELUS Health], and Med Access [TELUS Health]). A description of the patients selected for the study is displayed in Table 2. This sample was age stratified with oversampling in older age-groups; we expected higher prevalence rates for the 8 chronic conditions.
Summary of Patient Characteristics (n=1,920)
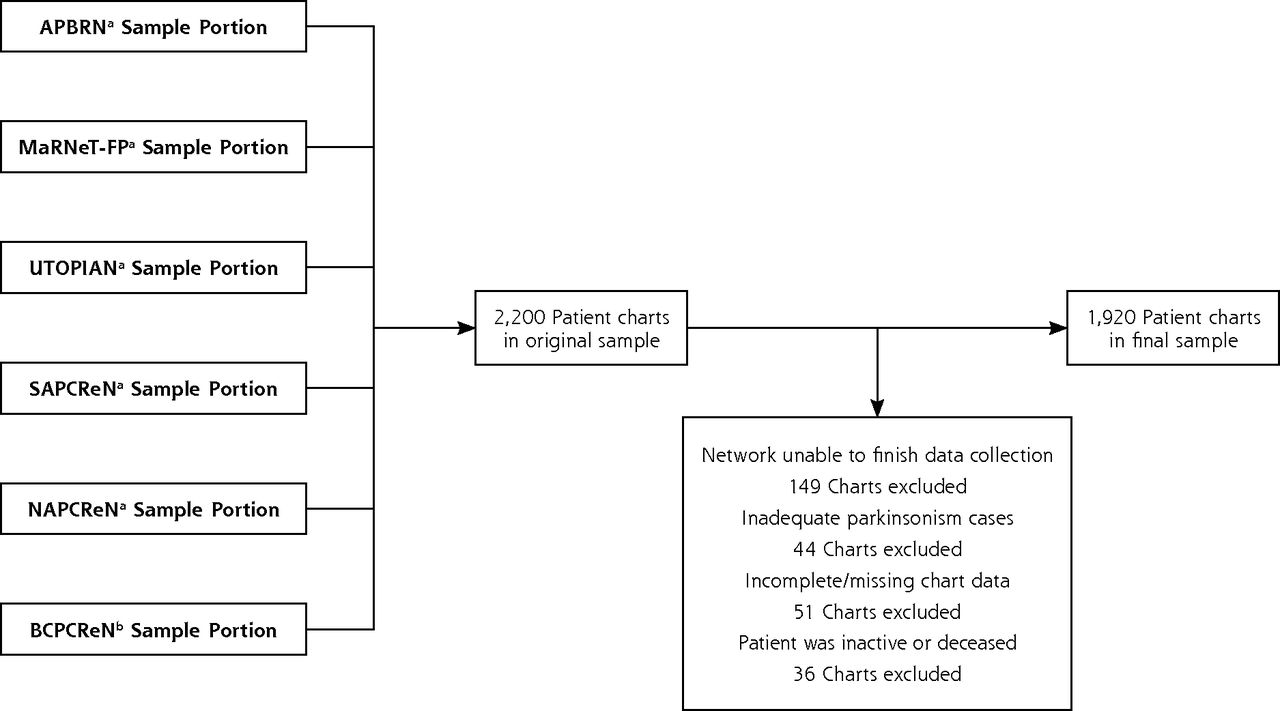
There was a shortfall of 280 charts from the planned sample of 2,200. One hundred forty-nine charts were excluded because of EHR access challenges. Forty-four charts were excluded because of an insufficient number of patients with parkinsonism to satisfy the additional 25 per network. Eighty-seven charts were excluded because the EHR record was incomplete (n = 51), the patient had left the practice (n = 12), or was deceased (n = 24) (Figure 1).

Sample inclusion and exclusion flow chart.
APBRN = Atlantic Practice Based Research Network; BCPCReN = British Columbia Primary Research Care Network; MaRNet-FP = Maritme Family Practice Research Network; NAPCPReN = Northern Alberta Primary Care Research Network; SAPCReN = Southern Alberta Primary Care Research Network; UTOPIAN = University of Toronto Practice Based Research Network.
a 350 Patients chosen at random, 25 patients case positive for epilepsy, 25 patients case positive for parkinsonism.
b 175 Patients chosen at random, 13 patients case positive for epilepsy, 12 patients case positive for parkinsonism.
Validation
Table 3 summarizes the validation metrics of sensitivity, specificity, PPV, and NPV for each of the 8 case definitions. Overall, sensitivity ranged from 77.8% (osteoarthritis) to 98.8% (parkinsonism). Specificity was high for all 8 conditions, with the lowest being observed for hypertension (93.5%). COPD had the lowest PPV (72.1%) and hypertension the highest (92.9%). Hypertension had the lowest NPV (86.0%) with values greater than 90% for all other conditions and many above 99%.
Summary of Validation Results
DISCUSSION
CPCSSN provides the first pan-Canadian primary care EHR data repository. This work shows that CPCSSN has developed valid primary care EHR case definitions for identifying patients with hypertension, diabetes, depression, COPD, osteoarthritis, dementia, epilepsy, and parkinsonism. These case definitions could be used for a variety of data-driven activities in primary care, including surveillance, routine practice evaluation, feedback and quality improvement, and research.
Comparison With Other Studies
The validation metrics for the CPCSSN case definitions are comparable to, or better than, similar international databases. CPCSSN’s sensitivity rate for diabetes (95.6%) compares favorably with the United Kingdom’s Clinical Practice Research Datalink (formerly General Practice Research Database) (90.6%),7 as well as with a sample of EHR data from 17 physicians in 1 Canadian province (83.1%)8 and a general practice in Yorkshire, United Kingdom (98.3%).9 With respect to hypertension, the CPCSSN algorithm was both reasonably accurate (PPV of 92.9%) and comprehensive (sensitivity of 84.9%). Our findings are comparable to those observed in an EHR-based surveillance system in Sweden,10 while performing better than algorithms based exclusively on Canadian administrative data.11 The case definition for depression has validity properties that are comparable to EHR-based algorithms in the United States12 and better than algorithms based exclusively on billing and pharmacy data.13 A diagnostic algorithm for COPD used in a UK Clinical Practice Research Datalink study was less sensitive and specific,14 and algorithms derived from administrative data had lower sensitivity and PPV than those observed in our study.15–17 Little is known about diagnostic algorithms for osteoarthritis, though validation results from a predictive algorithm used in a computerized, diagnostic database in the United States had outcomes similar to those of this study.18
The CPCSSN case definition for dementia performed better than those constructed from Quebec billing data (sensitivity of 12.9%–39.7%)19 and Canadian administrative hospital discharge data (sensitivity of 32.3%–66.9%, specificity of 100.0%).20 The epilepsy results were similar to definitions using administrative databases for various Canadian provinces (PPV of 75.5%–98.9%, NPV of 94.0%–97.4%),21 and for definitions combining diagnoses and medications to identify epilepsy cases in a US managed care organization data system (PPV of 79.2%–84.1%).22 Lastly, cases of parkinsonism validated in an American Veteran’s Health Administration database showed strong PPV (81%) when using ICD-9 codes alone but had poor sensitivity (18.7%); sensitivity improved when ICD-9 codes and medications were combined (42.5%), but PPV suffered (53.3%).23
Strengths and Weaknesses
Previous validation studies using EHR data have been highly variable in their methodology; diagnostic algorithms and reference standard sources have varied across studies, and as a result, establishing acceptable and comparable values for the conventional epidemiological measures of validity (sensitivity, specificity, PPV, NPV) was a complicated task.24 For our study, randomly selecting charts enabled estimation of sensitivity and specificity, as well as positive and negative predictive value. Other studies have selected patients who were case positive, permitting only an assessment of the positive predictive value of the definition. 25 Further, our study is unique in that the validation of case definitions took place across multiple regional networks involving multiple EHRs. Last, this study has a relatively large total sample size compared with similar studies involving primary care chart abstraction.25 There were some limitations to our study. Using chart abstraction as the reference standard implies that the study is limited to information in the EHR. Missing diagnoses and incomplete documentation will limit the accuracy of the algorithms. Further, each case definition is currently limited to lifetime prevalence and for depression does not distinguish between chronic and episodic depression. The relatively low prevalence of epilepsy and parkinsonism in the general practice population necessitated oversampling with patients who were flagged as having the condition according to the algorithm. If the entire sample was selected this way, it would be inappropriate to speak about the sensitivity and specificity of these 2 case definitions. Given that the chart abstractors were completely blinded to the CPCSSN algorithmic diagnosis and that all charts were reviewed, however, we believe the calculated sensitivity and specificity are reasonable estimates. Another limitation is that interrater reliability was not measured; nevertheless, the standardized training manual and rigorous oversight during the review process promoted consistency. Although there were nonrandom exclusions from the study sample, it is unlikely that this would change the conclusions of the study. The largest exclusion was related to 1 network being unable to finish data collection because of technical problems. Other exclusions, such as insufficient number of parkinsonism cases and charts being incomplete or for deceased patients, are likely to have negligible impact on the overall study results. Including different EHRs is both a strength and a limitation, as doing so replicates reality; however, the study was not powered to detect differences between EHRs.
In conclusion, the CPCSSN case definitions show excellent sensitivity and specificity for hypertension, diabetes, epilepsy, dementia, and parkinsonism, and the validity in general for all 8 conditions was very good. CPCSSN has set precedence for systematically validating the case definitions used within our primary care database by way of an explicit, consistent, and robust methodology. The use of validated EHR-based clinical data from community-based primary care settings is essential to understand, inform, and evaluate disease epidemiology, as well as to improve primary care clinical practice, organizational development, and health system policy and planning.
Acknowledgments
Nathalie Jetté, Ron Postuma, and Frank Molnar contributed to the development of the neurological case definitions. Karim Keshavjee, Marshall Godwin, Wayne Putnam, and Michelle Greiver contributed to the development of the other 5 case definitions. Nathan Coleman assisted in the development of chart review criteria. The Neurological Health Charities Canada, as well as the research assistants and residents, contributed to the success of this initiative.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: Funding for CPCSSN is provided by the Public Health Agency of Canada through a contribution agreement with the College of Family Physicians of Canada. This study was also funded in part by the National Population Health Study of Neurological Conditions.
-
Disclaimer: The opinions expressed in this publication are those of the authors/researchers, and do not necessarily reflect the official views of the Public Health Agency of Canada. The author retained full academic control of this work including the right to publish.
-
Previous presentations: Portions of this work have been presented at the following conferences: Canadian Association of Health Services and Policy Research Conference, May 28–30, 2013, Vancouver, British Columbia; Canadian Society of Epidemiology and Biostatistics Biennial Conference, June 24–27, 2013, St. John’s, Newfoundland; Trillium Primary Health Care Research Day, June 19, 2013, Toronto, Ontario; North American Primary Care Research Group Annual Meeting, November 9–13, 2013, Ottawa, Ontario.
-
Supplementary materials: Available at http://www.AnnFamMed.org/content/12/4/367/suppl/DC1/
- Received for publication September 17, 2013.
- Revision received January 30, 2014.
- Accepted for publication February 22, 2014.
- © 2014 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Predicting Depression in Canadians with or at Risk of Diabetes: A Cross-Sectional Machine Learning Analysis
- Describing primary care patterns before and during the COVID-19 pandemic across Canada: a quasi-experimental pre-post design cohort study using national practice-based research network data
- Prevalence and management of dyslipidemia in primary care practices in Canada
- Predicting Diabetes in Canadian Adults Using Machine Learning
- Exploring the reliability of inpatient EMR algorithms for diabetes identification
- Using machine learning to standardize medication records in a pan-Canadian electronic medical record database: a data-driven algorithm study focused on antibiotics prescribed in primary care
- Atteinte des cibles therapeutiques pour le diabete de type 2 en 2015 et 2020 en medecine de soins primaires au Canada
- Older persons living with dementia and their use of acute care services over 2 years in Alberta
- Achievement of treatment targets among patients with type 2 diabetes in 2015 and 2020 in Canadian primary care
- Comprehensiveness of care for women with depression: Association between primary care use and cervical cancer screening
- Primary medication nonadherence in a large primary care population: Observational study from Manitoba
- A Review of 50 Years of International Literature on the External Environment of Building Practice-Based Research Networks (PBRNs)
- Increasing likelihood of prescribing recommended lipid management: Primary care providers participation in cardiology continuing medical education
- Development of a case definition for hearing loss in community-based older adults: a cross-sectional validation study
- Identifying heart failure in patients with chronic obstructive lung disease through the Canadian Primary Care Sentinel Surveillance Network in British Columbia: a case derivation study
- Trends in diabetes medication use in Australia, Canada, England, and Scotland: a repeated cross-sectional analysis in primary care
- Patients eligible and referred for bariatric surgery in southeastern Ontario: Retrospective cohort study
- Assessing the quality of clinical and administrative data extracted from hospitals: The General Medicine Inpatient Initiative (GEMINI) experience
- Cardiovascular risk factor documentation and management in primary care electronic medical records among people with schizophrenia in Ontario, Canada: retrospective cohort study
- Primary care EMR and administrative data linkage in Alberta, Canada: describing the suitability for hypertension surveillance
- Pelvic floor disorders in women who consult primary care clinics: development and validation of case definitions using primary care electronic medical records
- Validation of a case definition for speech and language disorders: In community-dwelling older adults in Alberta
- Prevalence of chronic kidney disease and cardiovascular comorbidities in adults in First Nations communities in northwest Ontario: a retrospective observational study
- A Clinical Phenotyping Algorithm to Identify Cases of Chronic Obstructive Pulmonary Disease in Electronic Health Records
- Quality of warfarin management in primary care: Determining the stability of international normalized ratios using a nationally representative prospective cohort
- Developing a case definition for type 1 diabetes mellitus in a primary care electronic medical record database: an exploratory study
- Trends in end digit preference for blood pressure and associations with cardiovascular outcomes in Canadian and UK primary care: a retrospective observational study
- Impact of the Diabetes Canada Guideline Dissemination Strategy on the Prescription of Vascular Protective Medications: A Retrospective Cohort Study, 2010-2015
- Antidepressant and antipsychotic prescribing in primary care for people with dementia
- Team-based comanagement of diabetes in rural primary care
- Use of Direct Oral Anticoagulants in Canadian Primary Care Practice 2010-2015: A Cohort Study From the Canadian Primary Care Sentinel Surveillance Network
- Manual review of electronic medical records as a reference standard for case definition development: a validation study
- Methods to describe referral patterns in a Canadian primary care electronic medical record database: modelling multi-level count data
- Clinical Population Medicine: Integrating Clinical Medicine and Population Health in Practice
- A national surveillance project on chronic kidney disease management in Canadian primary care: a study protocol
- Hospital admission rates and emergency department use in relation to glycated hemoglobin in people with diabetes mellitus: a linkage study using electronic medical record and administrative data in Ontario
- Is glycemia control in Canadians with diabetes individualized? A cross-sectional observational study
- The Cardiovascular Health in Ambulatory Care Research Team performance indicators for the primary prevention of cardiovascular disease: a modified Delphi panel study
- Association between neighbourhood walkability and metabolic risk factors influenced by physical activity: a cross-sectional study of adults in Toronto, Canada
- Automatic identification of type 2 diabetes, hypertension, ischaemic heart disease, heart failure and their levels of severity from Italian General Practitioners' electronic medical records: a validation study
- Update from CPCSSN
- Mise a jour sur le RCSSSP
- Using Canadian Primary Care Sentinel Surveillance Network data to examine depression in patients with a diagnosis of Parkinson disease: a retrospective cohort study
- Implementation of data management and effect on chronic disease coding in a primary care organisation: A parallel cohort observational study
- Association between registered nurse staffing and management outcomes of patients with type 2 diabetes within primary care: a cross-sectional linkage study
- Guiding the reporting of studies that use routinely collected health data
- Prevalence and management of dementia in primary care practices with electronic medical records: a report from the Canadian Primary Care Sentinel Surveillance Network
- Harnessing the power of longitudinal data
- Representativeness of patients and providers in the Canadian Primary Care Sentinel Surveillance Network: a cross-sectional study
- Comprendre la multimorbidite dans le contexte des soins primaires
- Understanding multimorbidity in primary health care
- Prevalence and management of osteoarthritis in primary care: an epidemiologic cohort study from the Canadian Primary Care Sentinel Surveillance Network
- Horses and buggies have some advantages over cars, but no one is turning back
- Prevalence and management of hypertension in primary care practices with electronic medical records: a report from the Canadian Primary Care Sentinel Surveillance Network
- Chronic obstructive pulmonary disease in primary care: an epidemiologic cohort study from the Canadian Primary Care Sentinel Surveillance Network
- The diagnosis of depression and its treatment in Canadian primary care practices: an epidemiological study
- In This Issue: Technical and Personal Systems, and Novel Risk Factors