


Primary care is essential to the functioning of a high-value health system. It helps achieve the Triple Aim: improved health care experience, improved health of the population, at decreased overall cost. However, primary care practice is challenging. Many residents and medical students see overburdened, high-stress practices and decide not to continue to care for patients in a primary care setting. We’ve proposed that in fact the goal in our health system is the Quadruple Aim, which is the Triple Aim plus joy in practice, that is, satisfaction for clinicians and staff.1
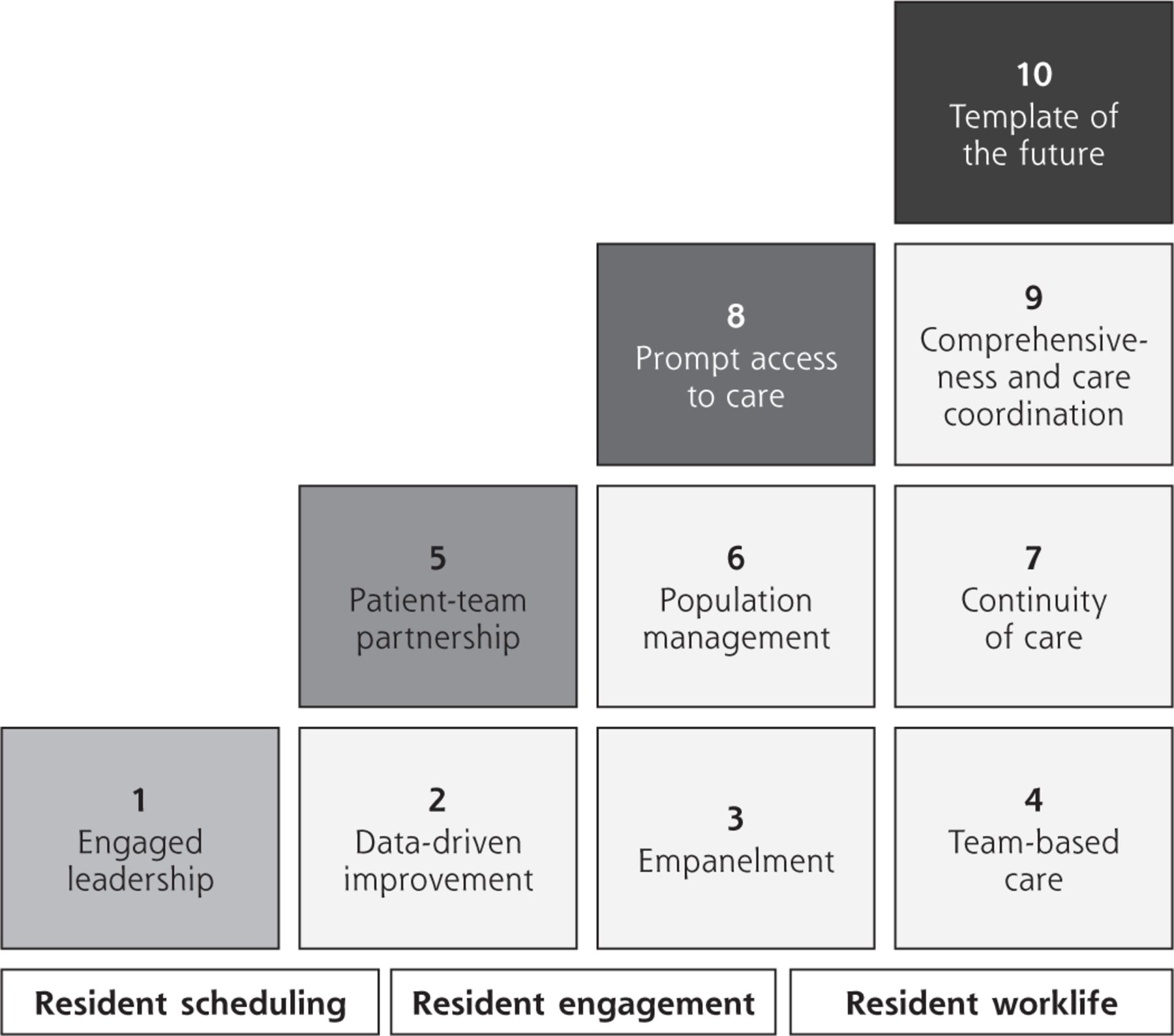
But how do we achieve the Quadruple Aim in our residency practices? How do we build excellent practices where residents are happy to work and provide excellent care for diverse patients? Two of us (M.K., T.B.) have visited a number of effective primary care practices over the last few years, practices we call “bright spots.” Based on our findings from these visits we’ve described “The 10 Building Blocks of High-Performing Primary Care”2 and after studying residency clinics, we added 3 more building blocks pertinent to residents: resident scheduling, engagement, and work life3 (Figure 1).
Six action steps to fix primary care residency training are:
Design resident schedules that prioritize continuity of care and eliminate tension between inpatient and outpatient duties
Develop a small core of clinic faculty
Create operationally excellent clinics
Build stable clinic teams that give residents, staff, and patients a sense of belonging
Increase resident time spent in primary care clinics to enhance ambulatory learning and patient access
Engage residents as coleaders of practice transformation4
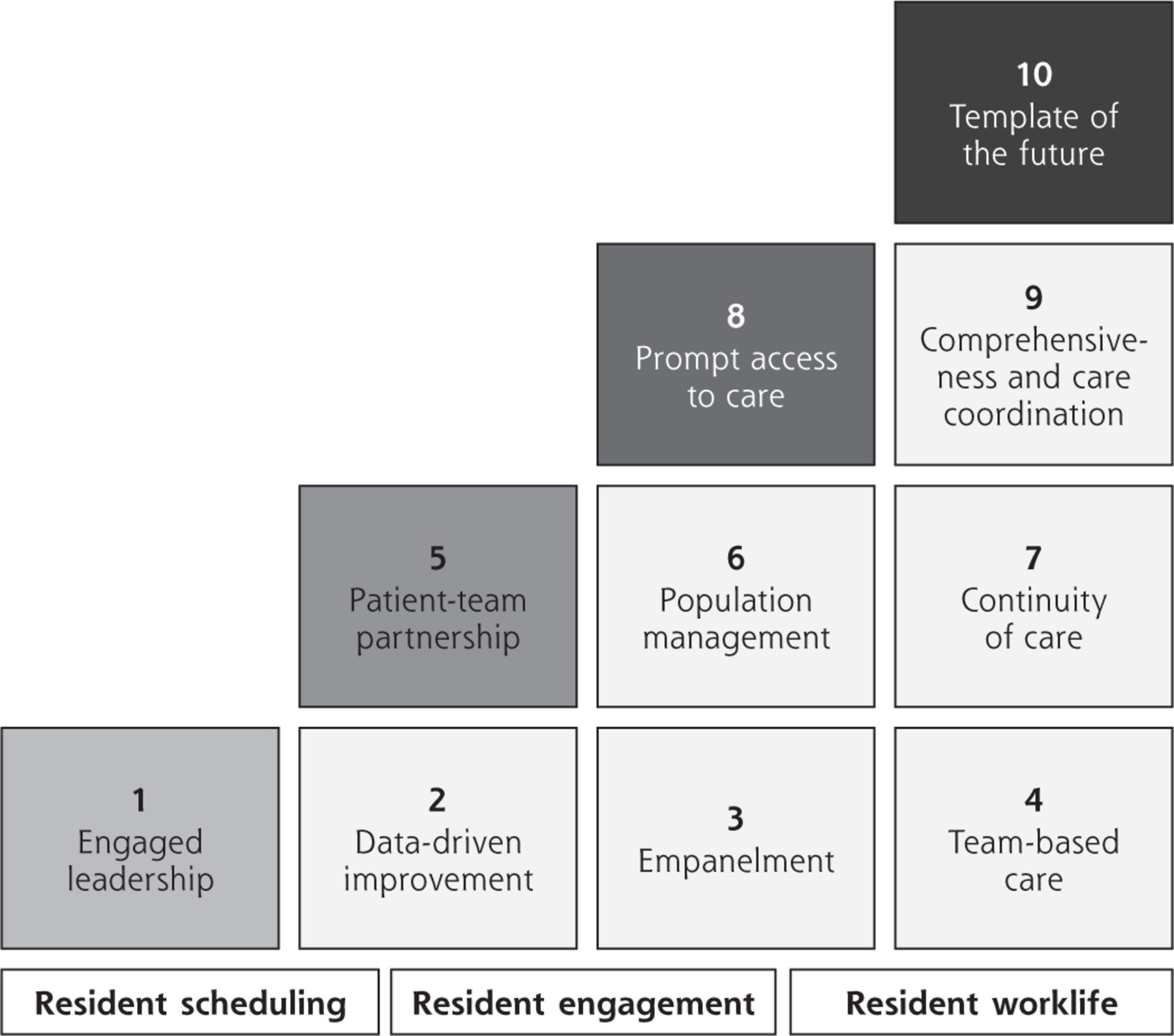
Building Blocks of High-Performing Primary Care model for residency teaching clinics.
The Association of Family Medicine Residency Directors (AFMRD) (S.B.) partnering with the University of California San Francisco Center for Excellence in Primary Care (M.K., T.B.) embarked on a project of coaching and collaboration to help apply the 10+3 building blocks to our members’ programs. In November 2017 we sent out the first call to programs to participate and selected 18 programs. In February 2018 with travel funding from AFMRD we held our first in-person meeting with these programs for a day and a half in Kansas City, Missouri. The collaboration continued with 6 interactive webinars over the next 8 months. Topics covered in the meeting and webinars included: prompt access to care, scheduling, advanced team-based care, continuity of care, access with continuity, interprofessional education and care, and resident engagement.
Participating programs rated the sessions highly. Eighty-nine percent of the programs rated the overall experience “excellent” (56%) or “good” (33%) at the midpoint evaluation. Comments from involved programs include: “an outstanding experience,” “it has been wonderful to collaborate with other programs,” “the collective passion in the room excited our group and provided the much needed impetus for new ideas and brainstorming…it’s an exciting new wave for primary care and we are eager to be a part of it.” Another participating group said: “We hope this initiative will continue to grow as we strive to continuously improve the ambulatory experience for our patients and our residents.”
Based on the success of the first cohort, the board of AFMRD continued with another year of funding and 15 programs were selected from a competitive application pool for the second cohort which commenced February 2019.
Participating programs have shared their experiences in blog posts which can be found at: https://www.afmrd.org/p/bl/et/blogid=1014.
Across the country, family medicine residency programs are addressing the fundamental dilemma of a teaching clinic: harmonizing (1) the teaching mission which requires residents to be in many different rotations in order to learn the skills of a primary care physician, and (2) the patient care mission for which patients would like their physician to be available all the time. While it is not possible to perfectly accomplish both missions, many family medicine programs are making great progress for their residents and their patients.
- © 2019 Annals of Family Medicine, Inc.





{kind=link}