
Abstract
PURPOSE To address doubts regarding National Lung Screening Trial (NLST) generalizability, we analyzed over 6,000 lung cancer screenings (LCSs) within a community health system.
METHODS Our LCS program included 10 sites, 7 hospitals (2 non-university tertiary care, 5 community) and 3 free-standing imaging centers. Primary care clinicians referred patients. Standard criteria determined eligibility. Dedicated radiologists interpreted all LCSs, assigning Lung Imaging Reporting and Data System (Lung-RADS) categories. All category 4 Lung-RADS scans underwent multidisciplinary review and management recommendations. Data was prospectively collected from November 2013 through December 2018 and retrospectively analyzed.
RESULTS Of 4,666 referrals, 1,264 individuals were excluded or declined, and 3,402 individuals underwent initial LCS. Second through eighth LCSs were performed on 2,758 patients, for a total of 6,161 LCSs. Intervention rate after LCS was 14.6% (500 individuals) and was most often additional imaging. Invasive interventions (n = 226) were performed, including 141 diagnostic procedures and 85 surgeries in 176 individuals (procedure rate 6.6%). Ninety-five lung cancers were diagnosed: 84 non-small cell (stage 1: 60; stage 2: 7; stage 3: 9; stage 4: 8), and 11 small cell lung cancers. The procedural adverse event rate was 23/226 (10.1%) in 21 patients (0.6% of all screened individuals). Pneumothorax (n = 10) was the most frequent, 6 requiring pleural drainage. There were 2 deaths among 85 surgeries or 2.3% surgical mortality.
CONCLUSIONS Our LCS experience in a community setting demonstrated lung cancer diagnosis, stage shift, intervention frequency, and adverse event rate similar to the NLST. This study confirms that LCS can be performed successfully, safely, and with equivalence to the NLST in a community health care setting.
Since 2011, when the National Lung Screening Trial (NLST) results showed a 20% decrease in lung cancer–specific mortality in a high risk population,1 lung cancer screening (LCS), using low-dose computed tomography, has been recommended as the standard of care by most professional and patient advocacy organizations.2-5 Guidelines for LCS programs have been published6,7 and LCS implementation has been described.8 The NLST listed as one of the study weaknesses the recognized expertise of the participating medical centers “in radiology and in the diagnosis and treatment of cancer” which raised the question of the generalizability of their results to community facilities.1 This concern was amplified by the American Academy of Family Physicians and contributed to the organization not endorsing LCS.9,10 To evaluate these concerns, we aim to describe our LCS program experience within a large metropolitan non-university, non-NLST, community, tertiary care system.
METHODS
Providence St Joseph Health (PSJH) system is one of the largest integrated systems in the United States and includes multiple outpatient care facilities, an insurance product, and 50 hospitals in Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington. Integrated systems have internal operational accountability, allowing for comprehensive review of clinical care. Our LCS program operated in the Portland, Oregon region of the PSJH system. The program was implemented by the cancer services group rather than the diagnostic imaging group due to clinical leadership, program novelty, and lack of a template. The LSC program began operations in November 2013 incorporating 7 hospitals (2 non-university tertiary and 5 community medical centers) and 3 freestanding imaging centers, in coordination with our interdisciplinary thoracic oncology program.
Patients were referred by primary care clinicians within and outside of PSJH. The program process is illustrated in Figure 1. Initially, shared decision making was provided by the LCS team, but in 2015, this transitioned to the primary care clinicians at their request due to their established patient-clincian relationship leveraging more intimate knowledge of patient-specific values in shared decision making. Lung cancer screening was carried out using NLST eligibility criteria, and after February 2015, the Centers for Medicare & Medicaid Services eligibility criteria (age 55-77 years, at least 30 packs per year smoking, smoking cessation less than 15 years, no cancer symptoms, no concomitant life threatening illness, medically fit and willing to undergo additional indicated medical management and future LCS).11 Patients not meeting eligibility were not screened. The required program components6,7 of smoking cessation and patient education were provided by the program coordinator, and after 2015, by primary care clinicians. Additional patient and clinician education was provided by a website12 that incorporated risk calculators and shared decision making tools. Primary care clinicians employed by PSJH ordered LCS via the electronic health record after eligibility determination and shared decision making. Non-PSJH clinicians faxed standardized order forms. A second eligibility check was carried out by a coordinator or by a diagnostic radiology team member before the scan. Lung cancer screening was carried out annually.2 Automated notification of follow-up LCS and patient reminder letters were initiated in 2017.
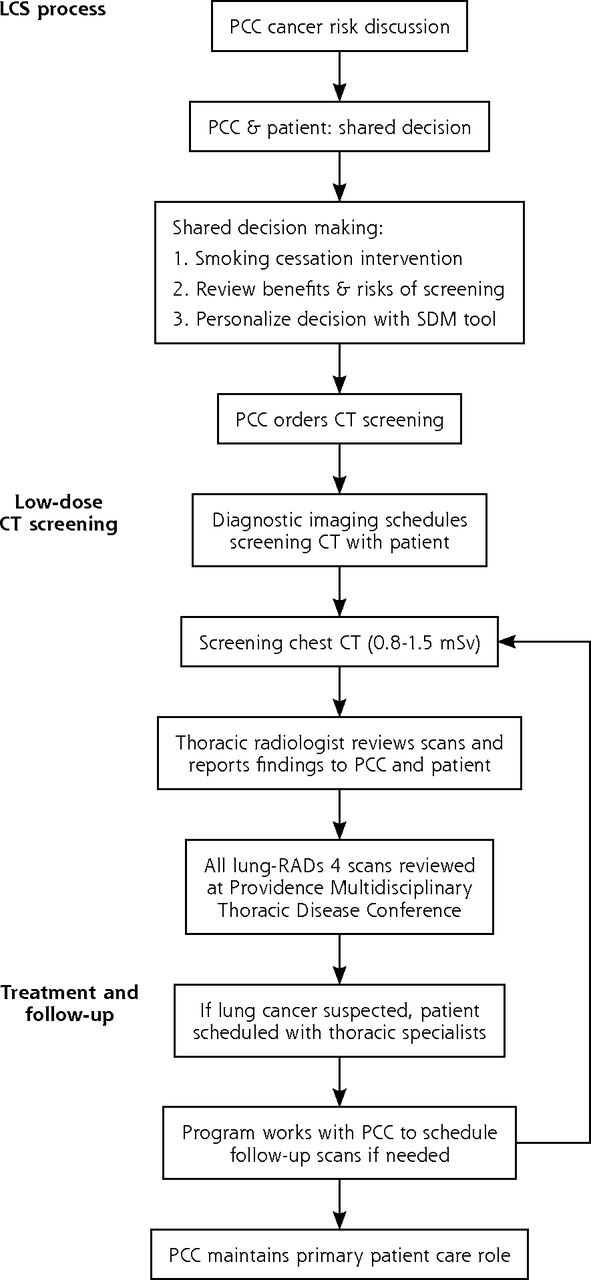
Lung cancer screening process.
CT = computed tomography; LCS = lung cancer screening; lung-RADS = Lung Imaging Reporting and Data System; PCC = primary care clinician; SDM = shared decision making.
All LCS examination techniques were standardized and performed in accordance with the American College of Radiology standard protocol specifying acceptable characteristics of the imaging machine and acquisition variables.6,7 Designated radiologists at the tertiary centers interpreted all the LCS results using algorithms for lung nodule identification and imaged lung nodule management. Interpretation utilized structured reporting, interpreting via an internally designed system (normal, suspicious-probably benign, suspicious-probably malignant, incidental finding-urgent/non-urgent). In 2014, this system was replaced by the Lung Imaging Reporting and Data System (Lung-RADS) categories. Briefly, Lung-RADS 1, 2, and 3 are negative (no nodules), benign, and probably benign, respectively. Category 4 is suspicious, requires further evaluation, and carries a ≥15% probability of malignancy.13 Every Lung-RADS 4 LCS result underwent review by a multidisciplinary thoracic disease conference (MTDC) consisting of physicians from pulmonology, thoracic surgery, medical oncology, radiation oncology, thoracic pathology, and thoracic radiology services. The MTDC generated guideline-compliant management recommendations to the referring primary care clinician, but where ambiguous, with an intentional program bias towards minimizing interventions. The primary care clinician managed all subsequent activity until referral to specialists.
Physicians involved in the program were from several medical settings, including some PSJH-employed groups (medical oncology, pathology, and thoracic surgery) and some fee-for-service groups (radiology, pulmonology, radiation oncology, and thoracic surgery). A PSJH full-time employee program coordinator recorded all imaging, procedures, adverse events, pathology, staging, and ensured follow-up LCS. The coordinator utilized a clinical research database that included registration (demographics, smoking history), schedule (all screening computed tomography scans, next due date), and post visit (scan information, LCS-generated procedures, or cancer diagnosis). Monthly, the coordinator generated a list of patients due for LCS. Each patient was sent 3 reminder letters. The referring clinician was notified that the patient was due for follow-up scan. The coordinator tracked the patients undergoing (or declining) LCS.
In 2014, our program was designated a Screening Center of Excellence by the Lung Cancer Alliance patient advocacy group.14
We retrospectively analyzed prospectively collected clinical data on individuals referred to our LCS program. Data was collected over 62 months (November 2013-December 2018) and analyzed. This study was approved by the Institutional Review Board (IRB 2018000035).
RESULTS
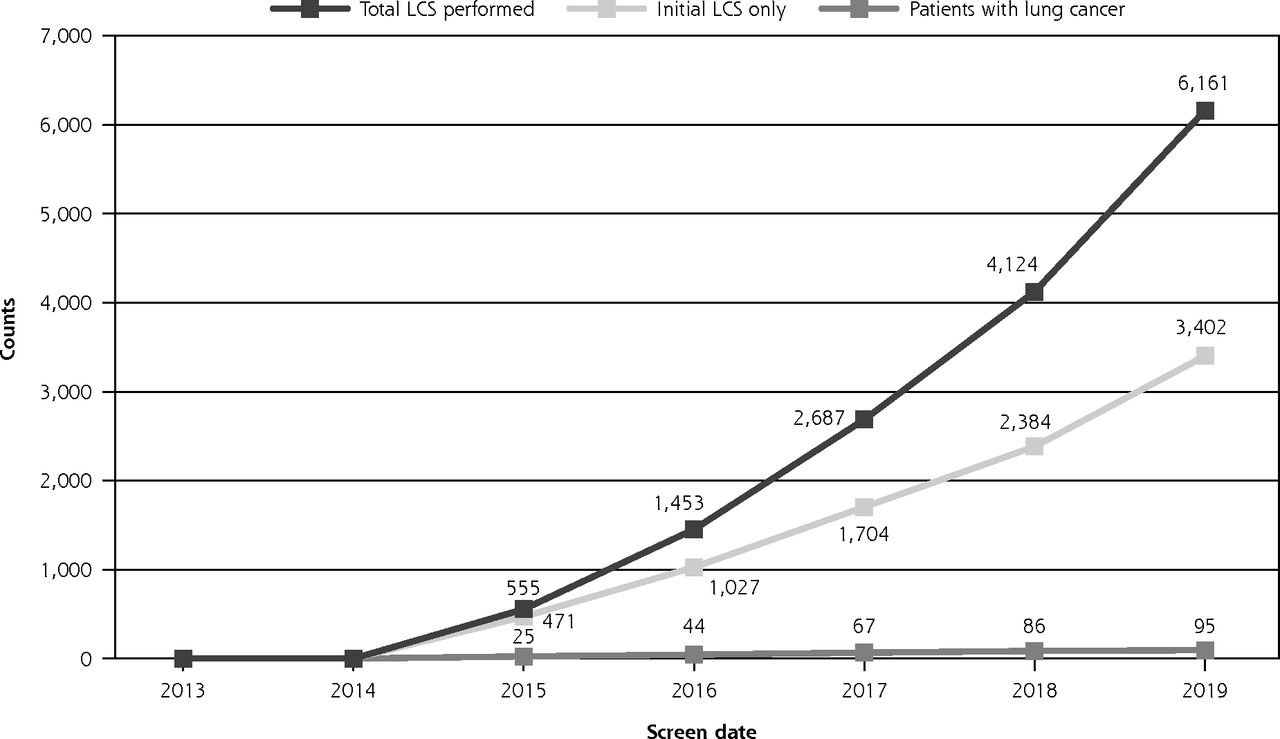
Of 4,666 referrals, 1,264 individuals were excluded or declined, and 3,402 individuals underwent initial LCS. Approximately 30% of LCS referrals originated from outside PSJH. Three of 3,402 LCS individuals were lost to follow-up (0.08%). Second through eighth LCSs were performed on 2,758 patients, for a total of 6,161 LCSs. Table 1 displays demographic information on the 2,513 people enrolled in the program at time of data review. The baseline scan total of 3,402 individuals was an accumulation of LCSs since 2013. At the time of data capture some of these patients had completed the program or had declined further participation, and they are not represented in Table 1. The details of LCSs after the initial screening is shown in Table 2. Figure 2 displays our LCS volume over the study period. Lung cancer screening Lung-RADs 4 presentations to the MTDC were not tracked until late 2015 and numbered: 48 in 2015, 94 in 2016, 92 in 2017, and 122 in 2018 for a total of 356.
Demographics of Enrolled Lung Cancer Screening Patients (N = 2,513)
Subsequent Patient Screening After Initial LCS (N = 3,402)
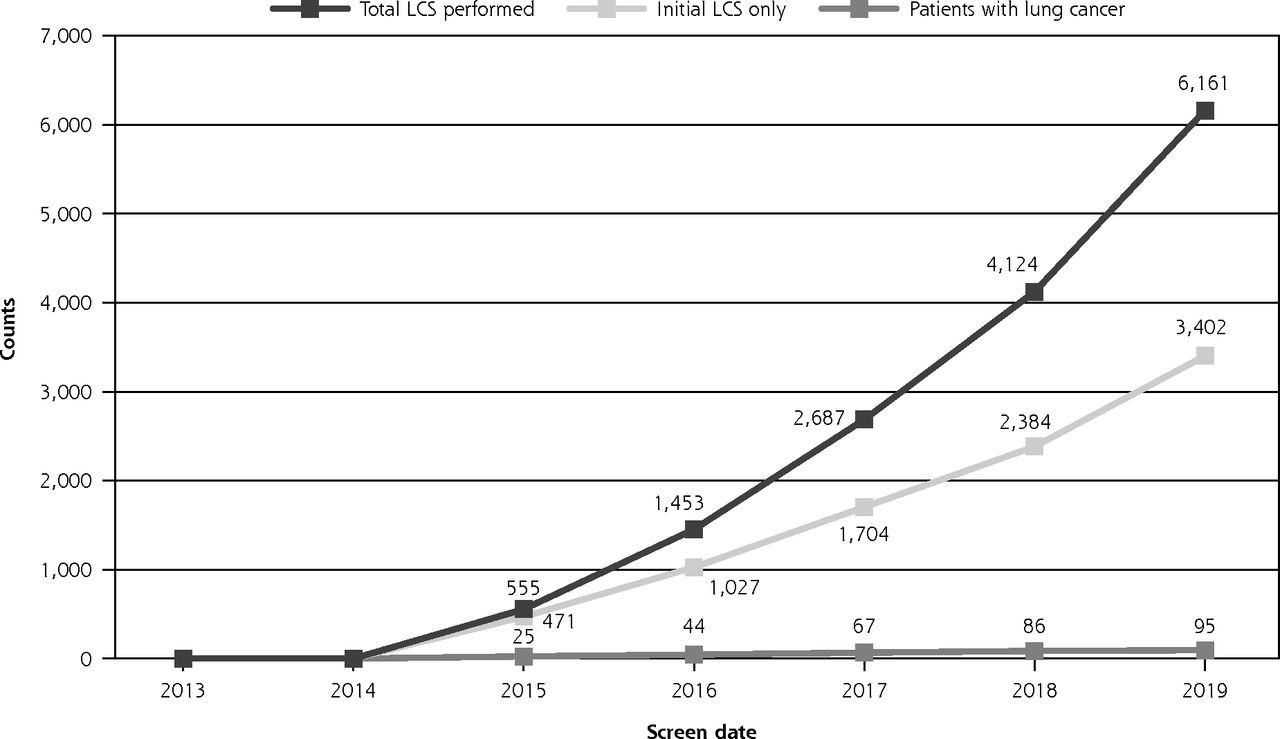
Cumulative number of lung cancer screens, initial LCS only, and patients diagnosed with lung cancer.
LCS = lung cancer screening.
Of the entire screened population, 500 patients (14.6%) had a result that triggered further investigation at some point during screening. Of those, 324 underwent additional imaging only. Table 3 depicts imaging activity in all patients requiring additional investigation (imaging and/or invasive procedures), with 31% performed outside of PSJH. There were 226 invasive procedures were performed in 176 patients, with or without imaging (Table 4), with 17% performed outside PSJH. Invasive diagnostic procedures were performed in 121 patients, the majority being bronchoscopy. Surgery was performed in 81 patients, the majority for a diagnosed malignancy (thoracic or extra-thoracic). Among 56 pulmonary resections for anticipated malignancy, 7 (12%) ultimately proved to be benign. None of the 7 patients experienced an adverse event. All lung resections were thoracoscopic.
Additional Imaging in 500 Patients Requiring Further Investigation (N = 1,179)
Invasive Interventions in 176 Patientsa (N = 226)
A total of 111 malignancies were diagnosed in 3,402 screened individuals. There were 95 lung cancers detected and 16 other malignancies (Table 5). Of note, early stage non-small cell cancer was detected in 67 patients (70% of diagnosed lung cancer) where surgical resection is the preferred treatment. Among early clinical stage lung cancer patients, 25 did not undergo resection: 1 refused any further evaluation, 18 were poor surgical candidates and underwent ablative radiation, 6 refused surgery, opting for ablative radiation. Of lung cancers diagnosed, 49% were detected on the initial LCS and the remaining 51% were detected during follow-up LCS.
Cancers Diagnosed After Lung Cancer Screening of 3,402 Individuals (N = 111)
Table 6 shows 23 procedure-related adverse events in 21 patients (0.6% of screened population), including 2 deaths (1 after thoracopic lobectomy and 1 after repair of ascending aortic aneurysm with concomitant aortic valve replacement and coronary artery bypass). The most common diagnostic complication was pneumothorax as the majority of procedures were either bronchoscopy or percutaneous lung biopsy. Of 10 patients with pneumothorax, 6 required a chest tube. Total procedure-related complication rate was 23/226 (10.1%). Surgery overall complication rate was 11/85 (12.9%) and 30 day or surgery hospitalization mortality 2/84 (2.3%). Examining only thoracic surgery, the complication rate was 8/64 (12.5%) with 1/64 (1.5%) thoracic surgery 30 day or surgery hospitalization mortality.
Procedure-Related Adverse Events in 21 Patients (N = 23)
DISCUSSION
Given the endorsement of LCS by most patient advocacy and professional organizations,2-5 health care delivery systems have been striving to implement LCS programs.8,15 Lung cancer screening provides for a stage shift to potentially curable lung cancer.1 Indeed, stage shift is the fundamental tenet of cancer screening. The utility of cancer screening in a well but at-risk population, however, is predicated upon disease-specific survival improvement in the setting of minimal harm.16
The concern expressed regarding the generalizability of the outcomes reported by the National Lung Screening Trial1 was amplified by the American Academy of Family Physicians (AAFP), representing 175,300 physicians and medical students nationwide.17
The AAFP stated, “The NLST… favorable results were conducted in major medical centers with strict follow-up protocols for nodules, have not been replicated in a community setting… The harms of these follow-up interventions in a setting with a less strict follow-up protocol in the community is not known… Much of the success of this trial is based on the low mortality associated with surgical resection of tumors, which may not be reproducible in all settings.”9,10 As such, the AAFP issued: “Grade I recommendation: The AAFP concludes that the evidence is insufficient to recommend for or against screening for lung cancer with low-dose computed tomography in persons at high risk for lung cancer based on age and smoking history.”9 Further, Huo et al18 used claims-based administrative data to create study cohorts with characteristics reflecting LCS eligibility and lung abnormalities on CT requiring interventions reported in the NLST (biopsy/cytology, bronchoscopy, thoracic surgery, other). They created a matched-control cohort to model costs of care and reported overall complications in greater than 20% of interventions, or double that reported by the NLST, specifically biopsy 18%, bronchoscopy 36%, and thoracic surgery 51%. Thirteen percent of complications were major. Modeled complication costs were high. They posited their results to be representative of community practice outcomes, advised use of this information in LCS shared decision making, and cautioned that community-based LCS would not be equivalent to the NLST. Finally, Pham et al reported very low LCS utilization (1.9%) in those eligible,19 perhaps due to the above and/or to the logistics of implementing a LCS program.
To inform the broad medical trend of LCS implementation and specifically address the NLST generalizability concerns outlined above, we evaluated LCS results in 3,402 people undergoing a total of 6,161 LCSs within a community, non-NLST, non-university, metropolitan, large tertiary care system. Compared with NLST, our population was less white (86% vs 91%), more female (50% vs 41%), older (age >65 years: 56% vs 27%), and had more current smokers (60% vs 48%). Our true positive or lung cancer diagnosis (95 of 3,402 individuals), stage shift (79% non-small cell lung cancer diagnosed stage 1 or 2), intervention rate (14.6%), further evaluation after positive LCS dominated by additional imaging vs procedures (CT was the most common additional imaging modality), procedure rate (6.6%), procedural adverse events (10.1%), surgical complications (12.9%), and 30-day or surgery-admission mortality (2.3%) are very similar to the NLST and the Veterans Health Administration reports.1,8
Care provided outside of study was not commented upon in the NLST. Although only 2% of our LCSs were performed outside PSJH, a substantial minority of our patients received indicated subsequent care outside of PSJH (additional imaging 31%, procedures 17%). This reality of community care is not reflected in our results, as our LCS coordinator tracked all clinical activity, providing 99.9% follow-up of the 3,402 screened individuals.
A possible weakness of our study nevertheless pertains to generalizability. Despite Portland PSJH being a community, non-university health system, our thoracic oncology program is staffed by chest specialists with local, regional, or national recognition. This expertise is reflected in our overall results, which we attribute to long-standing high clinical volume, multidisciplinary and specialized care,20 and is further manifest by our use of thoracoscopy for all pulmonary resections, and our low resection rate for benign disease, none of which suffered complications. Our LCS construct required resources, including medical leadership, and importantly, a full-time LCS coordinator. Without these, we could not have effectively followed and maintained timely interventions, or provided thorough results tracking, especially with care rendered outside of PSJH. Lack of availability of such resources could be a major limiting factor in the success of an LCS program.
Strengths of our study include the uniform application of our programmatic and clinical practice with complete catchment of clinical data across a single large metropolitan health system within a large clinical experience. We report 99.9% complete clinical follow-up. Additionally, our program complied with subsequently published program construct guidelines.6,7 Another strength was our high LCS adherence rate of 82% (Table 2), which was, however, somewhat lower than the 93-95% rate of the NLST. Finally, a hidden strength of this study is the rapid adoption and eager participation in LCS by the primary care clinician community in the Portland metropolitan area (Oregon). The primary care clinicians recognized in the NLST high-level clinical information and rapidly translated it into practice, prior even to their regional leadership‘s endorsement. The high rate of primary care clinician acceptance of our LCS program accounts for the high volume and upward trajectory (Figure 2) of patients evaluated. In fact, we did not market our LCS program due to the capacity limitation of having only a single program coordinator.
CONCLUSIONS
Low-dose computed tomography lung cancer screening can be done with low intervention and complication rates in a community non-university setting using, or more accurately stated, requiring a systematic multidisciplinary approach. This large cohort of screened patients demonstrates lung cancer diagnosis, stage shift, intervention frequency, and adverse event rate similar to the NLST. Our experience demonstrates that LCS can be done successfully and safely in a community setting.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/18/3/243.
- Received for publication October 11, 2019.
- Accepted for publication November 11, 2019.
- © 2020 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}