
Abstract
PURPOSE Variation in medical practice is associated with poorer health outcomes, increased costs, disparities in care, and increased burden on the public health system. In the present study, we sought to describe and assess inter- and intra-primary care physician variation, adjusted for patient and clinic characteristics, over a decade of practice and across a broad range of health services.
METHODS We assessed practice patterns of 251 primary care physicians in southern Israel. For each of 14 health services (imaging tests, cardiac tests, laboratory tests, and specialist visits) we described interphysician and intraphysician variation, adjusted for patient case mix and clinic characteristics, using the coefficient of variation. The adjusted rates were assessed by generalized linear negative-binomial mixed models.
RESULTS The variation between physicians was on average 3-fold greater than the variation of individual physician practice over the years. Services with low utilization were associated with greater inter- and intraphysician variation: rs = (−0.58), P = .03 and rs = (−0.39), P = .17, respectively. In addition, physician utilization ranks averaged over all health services were consistent across the 14 health services (intraclass correlation coefficient, 0.94; 95% CI, 0.93-0.95).
CONCLUSIONS Our results show greater variation in practice patterns between physicians than for individual physicians over the years. It appears that the variation remains high even after adjustment for patient and clinic characteristics and that the individual physician utilization patterns are stable across health services. We propose that personal behavioral characteristics of medical practitioners might explain this variation.
INTRODUCTION
Most experts consider the current level of health care spending to be unsustainable and identify the overuse of unnecessary health services as a primary driver of the cost.1-5 Medical practice variation is a terminology originated in the 1970s,6 which has important implications for both health care and health policy.7,8 Medical practice variation reflects practice differences among health care clinicians and includes overuse and underuse, both of which can have negative consequences for patients.9
Reduction of variation is a central theme of quality management, which started with industrial production and has recently been adopted with regard to medical practice.5,10,11 Greater medical practice variation is associated with poorer health outcomes, increased costs, disparities in care, and increased burden on the public medical system.5,12,13 Causes of medical practice variation can be categorized into 3 main domains: those associated with the patient population (eg, case mix, morbidity burden), those associated with health care system characteristics (eg, intensity of practice), and those associated with physician characteristics (eg, age, sex).14,15
Research on medical practice variation has frequently focused on the secondary and tertiary sectors of care, has been cross-sectional in design, and has usually analyzed the variation for a single service.6,16-22 In addition, owing to the limitations of the various administrative databases used for analysis, patient and health care system factors were neither analyzed within the same research frame nor adjusted for. Moreover, cross-sectional analysis precluded the comparison of interclinician variation (between clinicians) with intraclinician variation (change in individual clinician practice habits over time).
We sought to describe and assess inter- and intra-primary care physician variations, adjusted for patient and clinic characteristics, over a decade of practice and for a broad diversity of health services. Identifying the source of greater variation (inter vs intra) and health services with high variation might aid in devising intervention approaches aimed at reducing medical practice variation.
METHODS
Study Population
This was a retrospective cohort study of health services utilization by Clalit Health Services (CHS) primary care physicians in southern Israel. The National Health Insurance Law mandates that all citizens resident in the country join 1 of 4 official not-for-profit health insurance organizations that are prohibited by law from denying membership.23 The CHS divides Israel into a number of geographic regions, and residents within each region have similar access to health services. To eliminate supply-side heterogeneity,24 we included in our study patients and physicians residing and practicing in the southern region. The CHS is the largest health care provider in the area of southern Israel, covering approximately 67% of its 730,000 residents.
We included primary care physicians practicing for more than 1 year during the period 2003 to 2013 with more than 100 adult patients per practice. Primary care physicians in Israel have a fixed list of patients and comprise the principle source of referral to further health services such as specialist consultations, emergency department visits, medication dispensal, blood testing, imaging, etc. Primary care physicians can be either specialists in primary care medicine (4.5-year residency), specialists in internal medicine (4.5-year residency), or general practitioners. Physicians are paid by a capitation payment arrangement, that is, according to the monthly number of patients assigned to the practice. The fact that in the Israeli health care system there are limited direct financial incentives for physicians to request or withhold a given test allows us to study the behavioral phenomenon of practice pattern variation in a relatively closed environment.
Data Collection
The unit of analysis was physician/year/clinic (to address physicians working simultaneously in more than 1 clinic). The physician data included age, sex, seniority (length of time practicing, in years), number of years employed by the CHS, specialty, birth country, and practice size. The annual patient data (age >18 years) for each physician per clinic included age, sex, and socioeconomic status (SES), assessed by Israel's Central Bureau of Statistics metrics, as a neighborhood-level measure on a 20-point scale (national median is 10). The SES scale accounts for median age, average number of persons per household, average years of education, average number of persons per household employed, average income, average numbers of rooms and vehicles per household, Internet access, etc.25 Socioeconomic status scores < 6 points are considered to signify low socioeconomic status and are associated with morbidity, mortality, and greater costs for the health care system.26
The utilization data included 14 primary care health services that involve clinical scenarios with discretionary decisions,27 that is, situations in which the physician has the freedom to decide whether to utilize them.28 For these health services, different choices carry different benefits and risks, and therefore physicians differ in their decisions.29,30 In addition, for these selected health services, there is a universal requirement for referral to be issued by the primary care specialist.
The 14 health services can be categorized into the following 4 domains:
Imaging tests (4): bone scintigraphy, brain and spine computed tomography (CT), chest radiography, magnetic resonance imaging (MRI)
A composite of cardiac tests: 24-hour Holter electrocardiography, stress test, echocardiography
Laboratory tests (6): vitamin B12, vitamin D, thyroid-stimulating hormone (TSH), hemoglobin (Hb), carcinoembryonic antigen (CEA), prostate-specific antigen (PSA)
Specialist consultation visits (3): rheumatology, pulmonary, neurology
Statistical Analysis
To standardize the utilization levels between physicians, we calculated adjusted utilization rates per 1,000 patients: (adjusted utilization levels/total ensured patients affiliated with the physician) × 1,000 patients.
Calculation of Adjusted Utilization Rates
To derive adjusted utilization rates, we used generalized linear negative-binomial mixed models with an unstructured correlation matrix. The annual number of utilizations per physician in each service was defined as the dependent variable and the annual patient volume as the offset variable. Physicians, clinics, and years were included as random clusters and patient characteristics (age, sex, SES, patient volume) as fixed covariates. We chose negative binomial rather than Poisson distribution because of the overdispersion of outcomes (deviance substantially greater than 1). We obtained adjusted utilization levels from the regression models and calculated the annual adjusted utilization rate for each physician in each health service as described above. We used the glmmTMB R package, version 1.0.136 (the R Foundation) and IBM SPSS, version 24 (IBM Corp).
Descriptive Analysis
The analysis focused on 2 types of variations: interphysician (between physicians) and intraphysician (changes in practice pattern of individual physicians over the years). For each health service, we described 2 variations by the coefficient of variation (CV) calculated as,
where for interphysician we calculated CV based on physicians’ averaged adjusted utilization rates, and for intraphysician we first calculated a CV for each physician and averaged them as the health service’s overall intraphysician CV. The adjusted utilization rates are presented as mean (SD) and CVs as percent (95% CI). We used the Spearman test to assess the association between the average adjusted utilization level of a given health service and its variation.
We further examined whether the utilization level for an individual physician was consistent across all 14 health services. We ranked physicians from 1 to 251 for each health service according to their adjusted utilization rates and then assessed the stability of the ranks by calculating the intraclass correlation coefficient.
Sensitivity Analysis
Because we used utilization rates instead of referrals, we performed a sensitivity analysis comparing between- and within-physician CVs for referrals and utilizations from 2011 to 2013. The analysis included 4 health services for which both referral and utilization data were available (MRI, chest radiography, and neurology and rheumatology specialist consultation visits).
RESULTS
Study Population
Table 1 summarizes physician characteristics. Of 251 primary care physicians, 141 (56%) were board-certified specialists in primary care medicine, 96 (38%) were general practitioners, and the remaining 14 (6%) were board-certified internal medicine specialists. Fifty-two percent were female, mean age was 51.3 (8.5) years, and median (interquartile range [IQR]) time in practice (seniority) was 26 (18-35) years.
Demographic Characteristics of Physician Population as of 2013 (N = 251)
The overall number of patient-years was 3,238,498, with a median annual total patient population of 289,726. The median number of patients per practice was 1,252.5 (994.3-1,497.4), with a mean age of 44.8 (10.8) years and a median SES of 7.3 (2.5-9.1).
Utilization Rates
Table 2 summarizes the annual utilization rates per 1,000 patients, adjusted for patient characteristics and clinics, and the adjusted inter- and intraphysician CVs for each service. Of a total of 6,112,632 health service utilization events assessed, the greatest annual utilization rates were laboratory tests such as Hb, TSH, and vitamin B12, and the least were specialist visits, MRI, and CT. We calculated physician rank according to the adjusted utilization rate for each service, from the lowest to the highest utilizer. We assessed the interclass correlation coefficient for the ranks to be 0.94 (95% CI, 0.93-0.95).
Adjusted Utilization Rates per 1,000 Patients and Inter- and Intraphysician Variation Expressed as Coefficient of Variation (CV)
Inter- and Intraphysician Variations
The adjusted CV between physicians ranged from 48.0% to 135.7% (Table 2), with a mean of 75.2% (23.2%). The adjusted CV for individual physicians over 10 years was less, ranging from 14.0% to 81.0%, with a mean of 25.7% (17.2%). The ratio between inter- and intraphysician CVs ranged from 1.1 to 4.7, with a mean of 3.3 (0.9). The health services with both the greatest inter- and intraphysician variation were pulmonary specialist visits and vitamin D tests, and those with the least were Hb, bone scintigraphy, and TSH. In addition, health services with both high utilization and high variation were PSA, CEA, vitamin B12, and vitamin D laboratory tests.
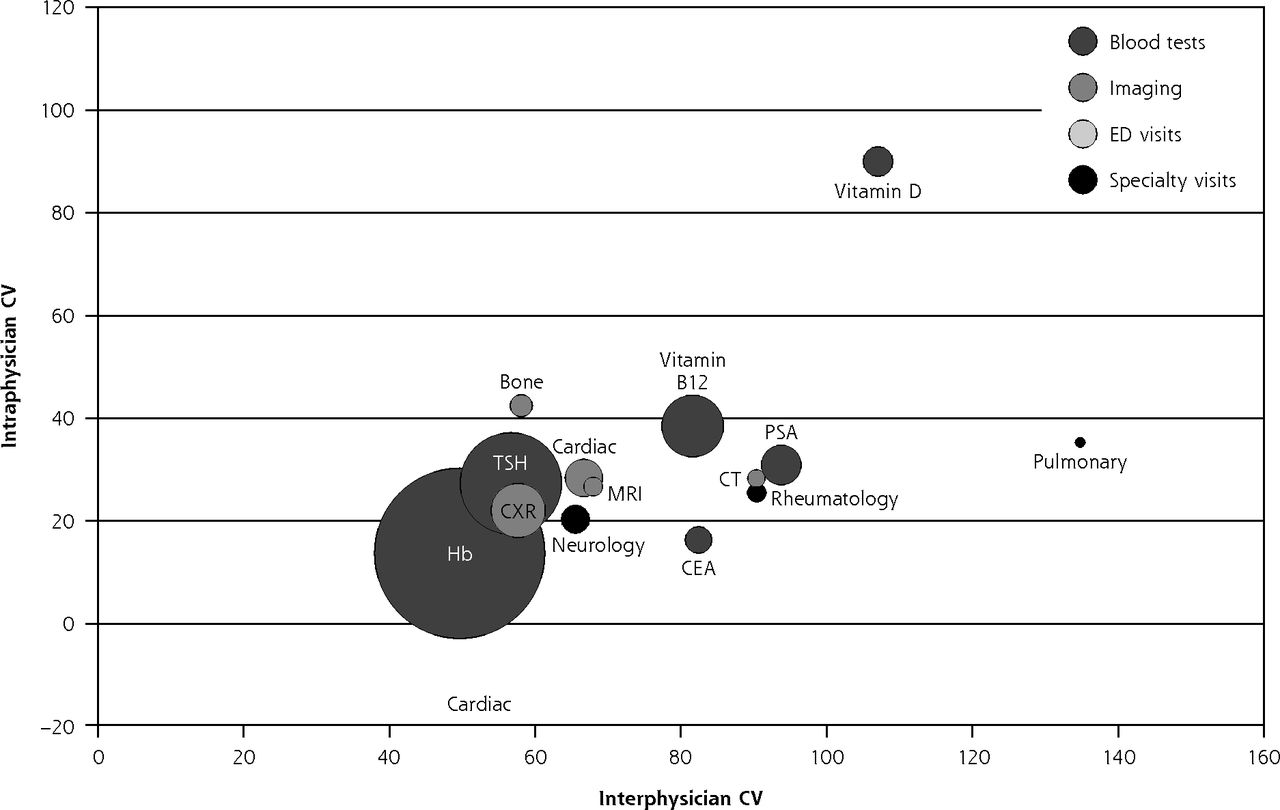
Figure 1 illustrates the association between utilization levels and inter- and intraphysician variation. We found negative correlations between utilization levels and interphysician variation: rs = (−0.58), P = .03 and between utilization levels and intraphysician variation: rs = (−0.39), P = .17. In addition, we found a positive correlation between inter and intraphysician variations: rs = 0.79, P = .001.

Inter- vs intraphysician variation and utilization rates.
CEA = carcinoembryonic antigen; CT = computed tomography; CV = coefficient of variation; CXR = chest radiography; ED = emergency department; Hb = hemoglobin; MRI = magnetic resonance imaging; PSA = prostate-specific antigen; TSH = thyroid-stimulating hormone.
Note: Health services are shown by inter- and intraphysician variation (x and y axis, respectively) and utilization rates (circle size). High inter- and intraphysician variation health services are positioned at the upper right, and low inter- and intraphysician variation health services are at lower left. Larger circle size indicates higher utilization rate.
Sensitivity Analysis
The results of the sensitivity analysis are presented in the Supplemental Appendix (https://www.AnnFamMed.org/content/19/1/30/suppl/DC1/) and show that the utilization CVs and referral CVs were similar. The differences ranged from 7% to 14.4% for interphysician CVs and 1.8% to 3.5% for intraphysician CVs. This finding suggests that the utilizations are comparable to the referrals.
DISCUSSION
In this study of 251 primary care physicians’ utilization patterns for a variety of different health services, we found a large variation both between physicians and for individual physician practice over the years. The variation was adjusted for patient case mix and clinic characteristics and was greater for inter- than intraphysician utilization patterns. In addition, services with low utilization were associated with greater adjusted variation. Laboratory tests showed both high utilization and high variation. Furthermore, physician practice patterns appeared to be stable, with little variability in utilization rates among the 14 health services assessed, that is, physicians with high utilization or low utilization showed similar patterns across all services analyzed. This might imply that practice patterns are intrinsic characteristics of each individual physician and are less related to specific health service characteristics.
Medical practice variation is not commonly researched on an individual physician-level across a number of different health services and over a long period of time. We believe that medical practice variation is an important measure because it reflects both overuse and underuse. The latter can have negative consequences for health care for patients not receiving optimal care.9,31 In our study, the adjustment of utilization patterns for patient case mix makes possible direct comparison between different clinics, physicians, and time periods.
Analyzing utilization patterns over a period of 10 years allowed us to assess intraphysician variation over time. This type of variation is important because it might reflect volatility, inconsistency, or learning curves of the physician. In addition, separating intra-from interphysician variation as opposed to assessing total variation allows for a better understanding of the variation source and hence for developing more precise interventions to reduce medical practice variation. Our finding that interphysician variation was 3 times greater than intraphysician variation might provide a useful metric for assessing the true degree of variation in cross-sectional studies of medical practice variation. Yet, while we can now identify the level of variation, we are still unable to pinpoint the actual cause.
Assessing variation in practice patterns is challenging, owing to a lack of agreed-upon metric and cut-off points to define high/low or acceptable variation. In the present study, we used CV, a standardized measure of frequency distribution. However, there are no well-defined cut-off points for grading of CVs in decision making. For other scientific fields, such as agriculture, acceptable levels of dispersion are characterized by CVs in the range of 10% to 20%.32
We found a negative correlation between the level of utilization of a given health service and interphysician variation, consistent with findings of a recent study of 44 health services in the United Kingdom.33 This negative correlation can be explained by CV mathematical properties for which distributions close to 0 are characterized by a greater CV.34-37 This finding has direct practical implications for medical practice variation research, showing that comparison between services requires adjustment for the level of utilization. For both the present study and the UK study,33 services with both high utilization and high variation were laboratory tests: PSA, CEA, vitamin B12, and vitamin D in the present study and blood clotting, vitamin D, urine albumin, PSA, bone profile, C-reactive protein, and urine microscopy, culture, and sensitivities in the UK study.33 A potential explanation for this finding might be that practitioners perceive simple laboratory tests as not economically harmful to the health care system and use them as a tool for patient reassurance.38 We suggest that health policymakers should focus on these types of health services for planning cost-effective interventions to decrease medical practice variation.
What are the practical implications of medical practice variation research? We believe that the next step should be toward decreasing variation.39 Given that the present and prior studies40 have shown that variation remains high even after adjustment for many patient- and physician-level characteristics, we believe that future research should focus on unexplained variation. Before designing and implementing appropriate interventions, further understanding is needed regarding potential physician personal behavioral characteristics that influence variation and the referral threshold.41 This could aid in designing more appropriate interventions to address exact personal behavioral causes.42 Therefore, it is worthwhile to examine the contribution of personal behavioral characteristics, such as knowledge, skills, attitudes, and personality, to unexplained variation.43,44 We suggest 2 approaches to address personal behavioral characteristics associated with variation: (1) training and coaching regarding the personal characteristic that gives rise to an unwarranted behavior;44-48 this might include training/coaching on positive psychology,49 mindfulness,50-53 and self-determination,47,54 and (2) changing the behavior itself by clinical decision support, performance feedback, and targeted reminders of appropriate indications.55,56
The present study has several important limitations. First, the study was limited to southern Israel, which has the lowest life expectancy in the country (79.6 years), the fewest doctors per 1,000 patients (2.8), and the fewest hospital beds per 1,000 patients (1.4).57 These characteristics might influence utilization and variation patterns, and therefore our findings can only be generalized to other regions and countries after accounting for these characteristics. Second, given the limitations of administrative databases, we assessed utilization rates rather than physician intent (referral). Therefore, it is possible that in some instances, referrals were not executed by patients, or patients were referred to health services not by their primary care physician. However, as part of the sensitivity analysis (Supplemental Appendix), we found that the variation in referral and utilization rates of 4 selected health services was similar, suggesting that variation in the latter is a valid approximation of that in the former. Third, we used physician as a unit of analysis, and therefore we cannot assess the effect of the individual patient pattern of health service utilization, that is, the analysis did not account for the existence of high-utilization patients. Fourth, it is possible that some instances of health service use were not discretionary (eg, head CTs for elderly patients after head trauma). However, the inclusion of these types of utilization decreases variation and thus results in a bias toward 0 (acceptance of the null hypothesis). Fifth, adjustment only for sex, age, and SES might have resulted in residual confounding by, for example, the differing health status of the clinics’ populations. It has been reported, however, that this type of adjustment can indirectly address the question of health status differences between practices.58 Finally, we did not assess patient-oriented health outcomes, such as mortality, hospitalizations, and life-threatening events, that might be associated with over- or underutilization. Therefore, we cannot estimate the association between practice patterns and health outcomes. However, given that medical practice variation has been shown to be associated with poorer health outcomes,5,9,12,13,59 we believe that describing the variation itself can aid in the development of approaches to reduce it.
Conclusion
In this study, we showed high variation in practice patterns among primary care physicians over a long time period and across a broad range of health services. Future research should focus on unexplained variation by case mix and health system characteristics and also on the personal behavioral characteristics of medical practitioners.
Footnotes
↵* These authors contributed equally to this work.
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at https://www.AnnFamMed.org/content/19/1/30.
Funding support: Supported by a research grant from Israel Health Policy Institute (grant number 2014/134/r).
Ethics approval and consent to participate: This study was approved by the Soroka University Medical Center Institutional Ethics Committee (0063-14-SOR).
Supplemental materials: Available at https://www.AnnFamMed.org/content/19/1/30/suppl/DC1/.
- Received for publication May 24, 2019.
- Revision received July 14, 2020.
- Accepted for publication July 24, 2020.
- © 2021 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Unravelling the determinants of medical practice variation in referrals among primary care physicians: insights from a retrospective cohort study in Southern Israel
- Methodology paper for the General Medicine Inpatient Initiative Medical Education Database (GEMINI MedED): a retrospective cohort study of internal medicine resident case-mix, clinical care and patient outcomes
- BNT162b2 mRNA COVID-19 vaccine and booster in patients with autoimmune rheumatic diseases: a national cohort study