
Article Figures & Data
Figures
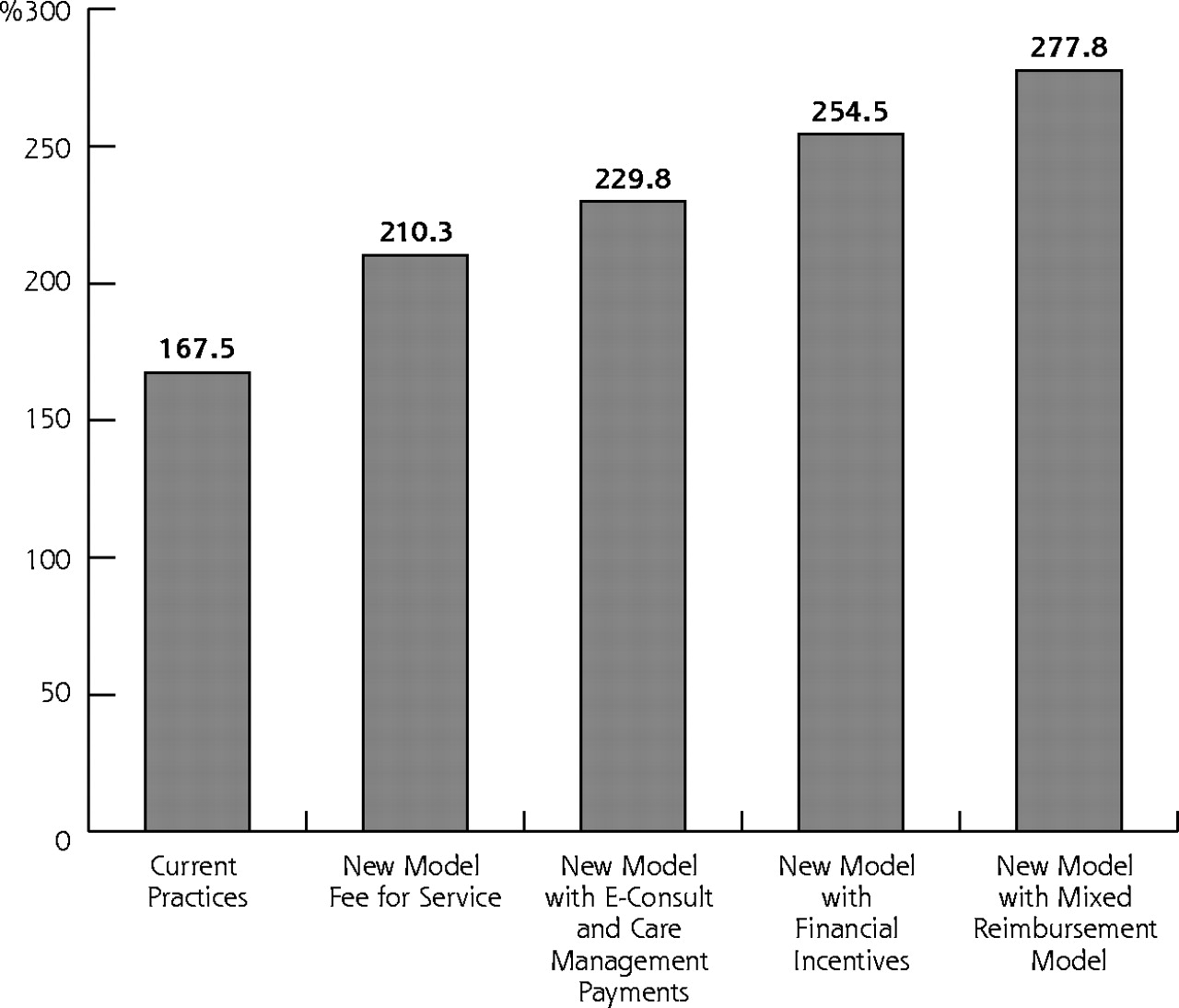
- Figure 1.
Physician compensation under alternative reimbursement models (in thousands of dollars).
Source: Lewin Group estimates.13
Note: Assumes physicians use savings in time worked to increase patient volume to maintain total hours worked per week.
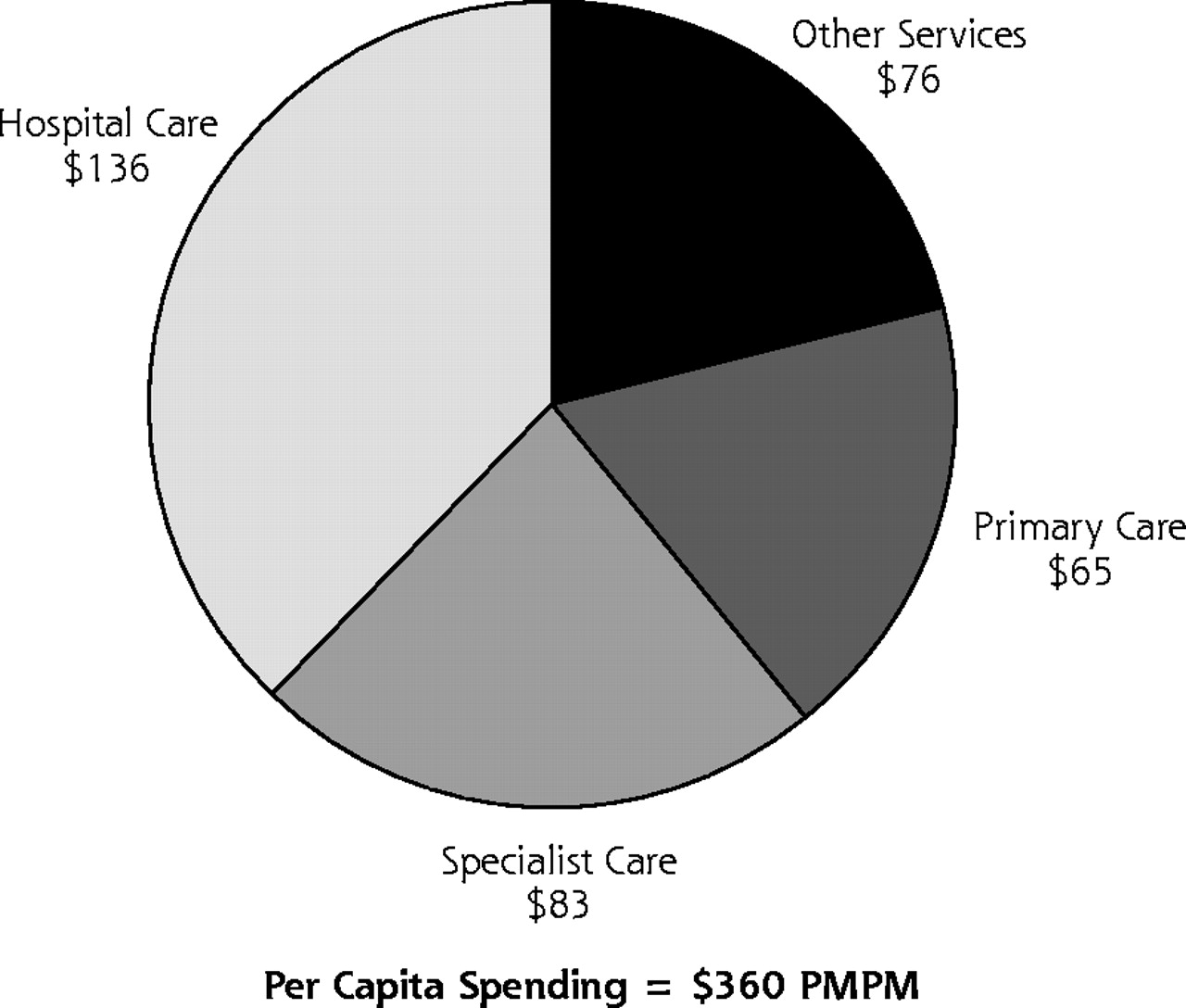
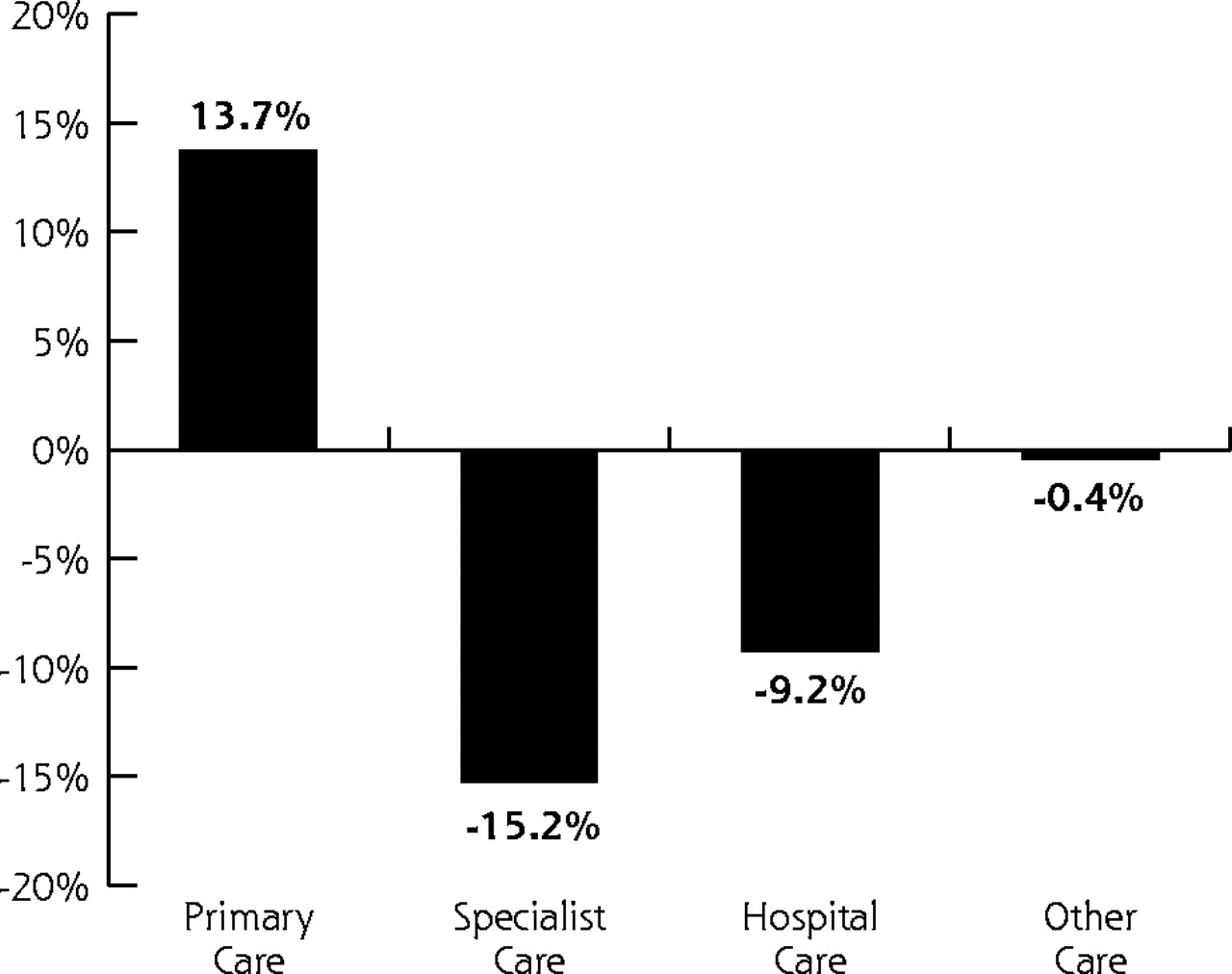
- Figure 2.
Changes in health care spending according to service type with expanded primary care, 2004.
Source: Lewin Group estimates.13
PMPM = per member per month. Notes: Estimates of health spending are for privately insured persons excluding dental coverage. Distribution estimated by the Lewin Group using the Medical Expenditures Panel Survey data (MEPS). Changes in health spending assume an increase in primary care physician utilization in proportion to the number of persons using a primary care provider as their primary source of care. Assumes a corresponding reduction in specialist utilization at the higher levels of reimbursement received by specialists. Assumes reduction in hospital and other care corresponding to the estimated savings in health care of $67 billion.



Tables
Practice Outcome New Model Feature Up-Front Training Costs Number of Services RVUs per Service Physician Time per Service RVU = relative value unit; MD/DO = medical doctor or osteopathic physician; CPT = Current Procedural Terminology; RN = registered nurse. * Substitutes for CPT 99212. Open-access scheduling None −6.5% 10% None Online appointment 1 d × 2 administrative staff None None None Electronic health records 3 d × number of users None 1% −5% Group visit 2 d for 1 MD/DO + 2 d per clinical staff person None None −50% E-visits None None* None Half of CPT 99212 Chronic disease management None None None None Web-based information Part of office expenses None None None Team approach (leveraging staff) $2,000 + 5 d for 1 MD/DO + 5 d per clinical staff person None None −5% Clinical practice guideline software $2,000 + 3 d for 1 MD/DO +3 d per clinical staff person None None −3% Outcomes analysis 5 d for 1 MD/DO and clinical staff person None None 5 d/y Practice Outcome New Model Feature Clinical Staff Time per Service Office Expense Administrative Staff Malpractice Premium RVU = relative value unit; MD/DO = medical doctor or osteopathic physician; CPT = Current Procedural Terminology; RN = registered nurse. * Substitutes for CPT 99212. Open-access scheduling None None None None Online appointment None $1,920/y −10% in reception time and cost None Electronic health records −5% $35,000 per MD/DO, amortized over 5 y −10% −5% Group visit −50% $250 per group visit None None E−visits Half of CPT 99212 $3,000 None None Chronic disease management 1 RN per 200 patients None None None Web-based information None $10,000/y Part of office expenses None Team approach (leveraging staff) +5% None None None Clinical practice guideline software +3% None None None Outcomes analysis 5 d/y None None None Financial Model Component Inputs to Model Data Sources RBRVS = Resource Based Relative Value System; RVU = relative value units; AMA = American Medical Association; MGMA = Medical Group Management Association; CMS = Centers for Medicare and Medicaid Services; Revenue Reimbursement levels (ie, price) Physcape (service mix) Quantity (ie, mix and number of services) Medicare RBRVS (RVUs) AMA Physician Socioeconomic Statistics (payer mix) Expenses Medical supply expenses AMA/MGMA data (overall direct and indirect practice expenses, physician salary, medical liability) Medical equip expenses CMS Clinical Practice Expense Panels data Clinical staff expenses CMS physician time data Medical liability Bureau of Labor Statistics (salaries) Office expenses Administrative staff expenses and other indirect expenses Physician hours worked Patient care hours AAFP Practice Profile Survey Total hours AMA physician socioeconomic statistics Source: 2003 AAFP Member Profile Survey. Physician Socioeconomic Status: 2000-2002 Edition. American Medical Association, Center for Health Policy Research, 2001 also reports 50.6 h/wk (patient care), 4.4 h/wk (other)21,22 Weeks worked per year 47 Total hours worked per week 51 Patient care hours per week 40 Other professional activities per week 11 Total patient care hours per physician per year 1,880 Total hours per physician per year 2,397 Payer Payment Levels Relative to Commercial Payers Percent of Revenues Source: Lewin Group,13 Wassenaar & Thran,22 Direct Research23 and Norton.24 Commercial 1.00 45 Medicare 0.83 27 Medicaid 0.53 13 Self-pay 1.20 16 Services Number of Services Total RVUs Source: Lewin Group estimates.13 RVU = relative value unit. Services Evaluation and management 5,281 8,305 Medicine 729 389 Radiology 263 315 Surgery 1,026 808 Other 73 54 Total services per physician 7,371 9,872 Other services Drugs 263 — Medicine (non RVU) 383 — Pathology/laboratory testing 2,577 — Other 203 — Total other services per physician 3,426 — All services per physician 10,797 9,872 Source Revenue ($) Costs ($) Compensation ($) Source: Lewin Group estimates, based on a 5-physician practice.13 Payer Commercial 1,003,213 529,965 473,248 Medicare 609,576 322,019 287,557 Medicaid 287,918 152,098 135,820 Self-pay 348,650 184,181 164,470 Total for practice 2,249,357 1,188,262 1,061,095 Bad debt 43,862 — — Charity care 179,949 — — Net for practice 2,025,546 1,188,262 837,284 Total compensation per physician 405,109 237,652 167,457 Income per physician — — 142,338 Benefits per physician — — 25,119 Change in Compensation Per Physician Feature of New Model With Reduction in Hours Worked ($) With Current Work Hours ($) Source: Lewin Group estimates.13 Note: numbers in parentheses indicate loss. Open access scheduling 9,133 9,133 Online appointment 5,752 5,752 Electronic health records 3,398 15,573 Group visits (8,769) 15,411 E-visits (7,649) (3,786) Chronic disease management (8,591) Web-based information (2,000) (2,000) Leverage clinical staff (6,121) 9,699 Clinical practice guideline software (3,877) 5,664 Outcomes analysis (2,180) (2,180) Change in compensation with new model (20,904) 42,831 Average compensation per physician 167,457 Total compensation per physician 146,553 Change, % −12 26 Hours Worked Weekly Total Compensation ($) Income ($) Source: Lewin Group estimates.13 Note: Income was derived from total compensation by assuming that income is 85% of total physician compensation. The result likely understates income at more than 51 work hours and overstates income at less than 51 hours, because income will rise as a percentage of total compensation as compensation increases. 40 132,104 112,288 41 139,184 118,306 42 146,272 124,331 43 153,366 130,361 44 160,465 136,395 45 167,570 142,435 46 174,679 148,477 47 181,793 154,524 48 188,911 160,574 49 196,033 166,628 50 203,159 172,685 51 210,288 178,745 52 217,420 184,807 53 224,555 190,872 54 231,694 196,940 55 238,835 203,010 Physicians in the Practice Practice Characteristic 1* 3 5 7 9 Source: Lewin Group estimates.13 *Solo practice that provides pathology and laboratory testing. Results are similar for a solo practice that does not provide pathology and laboratory testing in office. Income per physician (current baseline) ($) 131,949 138,199 142,338 144,112 145,097 Income per physician under New Model ($) 143,316 170,600 178,744 182,265 184,229 Percent change 9 23 26 26 27 New Model Characteristics Capital, $ New Staff, $ Lost Productivity Staff, $ (%) Physician, $ (%) Totals, $ (%) Totals per MD/DO, $ (%) MD/DO = medical doctor/doctor of osteopathy. * Assumes the practice subscribes to a Web-based service that does not involve new software or hardware in the practice. † Electronic health record (EHR) capital costs of $35,000 per MD/DO (Table 1) are already accounted for in the financial model. ‡ Sensitivity analysis measures loss in productivity at different percentages from 5% (minimum) to 20% (maximum) for 1 year (Source: Stello B, Charlton EM. Avoiding common pitfalls in selecting an EMR system. Fam Pract Manag. 1999;6:47–48); ($214,708 × indicated percentages) (rounded to nearest dollar). § Sensitivity analysis for loss in productivity for 1 year (as above) ($405,109 × indicated percentage × 5). II $3,000 in capital costs (Table 1) for e-visits is already accounted for in the financial model. ¶ Table 1 indicates 1 registered nurse (RN) would be needed per 200 patients and that 2% of a practice’s patients would benefit from chronic disease management. It is fair to assume a 5-physician practice would have at least 10,000 patients (200 is 2% of 10,000) and could thus employ an RN for this purpose. The practice would have to recruit 1 new RN. The cost of recruiting is approximately 10% of base pay for position; annual compensation for RN is approximately $52,000, according to US Bureau of Labor Statistics data. # Assumes practice uses AAFP service that provides Web site for free. ** Assumes that the EHR will contain embedded clinical decision support tools (guidelines) and therefore that clinical practice guidelines software is not a separate capital cost. Open-access scheduling 0 0 0 0 0 0 Online appointment 0* 0 0 0 0 0 Electronic health records 0† 0 10,735 ( 5)‡ 101,277 (5)§ 112,012 (5) 22,402 (5) 21,471 (10) 202,555 (10) 224,026 (10) 44,805 (10) 32,206 (15) 303,832 (15) 336,038 (15) 67,208 (15) 42,942 (20) 405,109 (20) 448,051 (20) 89,610 (20) Group visits 0 0 0 0 0 0 E-visits 0II 0 0 0 0 0 Chronic disease management 0 5,200¶ 0 0 5,200 1,040 Web-based information 0# 0 0 0 0 0 Team approach (leveraging staff) 0 0 0 0 0 0 Clinical practice guideline software 0** 0 0 0 0 0 Outcomes analysis 0 0 0 0 0 0 Totals 0 5,200 10,735 (5) 101,277 (5) $117,212 (5) 23,442 (5) 21,471 (10) 202,555 (10) $229,226 (10) 45,845 (10) 32,206 (15) 303,832 (15) $341,238 (15) 68,248 (15) 42,942 (20) 405,109 (20) $453,251 (20) 90,650 (20) - Table 11.
Change in Physician Compensation Under New Model, by Payment Category With Payments for E-visits and Chronic Disease Management in 2004
Payment Category With 18% Reduction in Hours Worked, $ With Current Work Hours,* $ Source: Lewin Group estimates using illustrated assumptions.13 Note: numbers in parentheses indicate loss. FTE = full-time-equivalent; FFS = fee-for-service. * Assumes physicians use savings in time worked to increase patient volume to maintain total hours worked per week. † Assumes all patients are enrolled in participating health plans. Assumes average panel of 2,030 patients per FTE physician. ‡ Assumes that e-visits are reimbursed at $25 per consultation up to a maximum of 25 consultations per patient per year. § Assumes chronic disease management is reimbursed at $15 per month for people with chronic illnesses. As in the micromodel section, the model assumes that a practice care manages only 2% of its patients. Because chronic disease management is expensive, this assumption is maintained throughout where chronic disease management is not directly reimbursed. If chronic disease management is directly reimbursed, it is assumed that 10% of patients are care managed. In addition, 2% of the population that can most benefit from intense chronic disease management is managed by 1 registered nurse for every 200 patients. For the remainder of the care-managed patients, the assumption is that each registered nurse manages 280 patients. Current average compensation Mean compensation per FTE physician† 167,500 167,500 Changes in compensation per FTE physician New Model within current FFS model (from microanalysis) (20,900) 42,800 With e-visit reimbursement‡ 4,631 4,715 Chronic disease management reimbursement§ 12,213 14,834 Total change in compensation (4,056) 62,349 Total compensation under policy Total physician compensation 163,444 229,849 Payment Category With 18% Reduction in Hours Worked, $ With Current Work Hours,* $ Source: Lewin Group estimates using illustrated assumptions.13 FTE = full-time-equivalent; FFS = fee-for-service; EHR = electronic health record. Note: numbers in parentheses indicate loss. * Assumes physicians use savings in time worked to increase the number of patients served. † Assumes all patients are enrolled in participating health plans. Assumes average panel of about 2,030 patients per FTE physician. ‡ Bonus amounts capped at $20,000 per physician. § Bonus of up to $80 per diabetes patient for high scores on diabetes care. Assumes 7% of patients have diabetes. II Bonus of up to $160 per cardiac patient for high scores in providing cardiac care. Assumes 3% of patients have cardiac conditions. Current average compensation Mean compensation per FTE physician† 167,500 167,500 Changes in physician compensation per physician New model under current FFS system (taken from previous microanalysis) (20,900) 42,800 Physician office link potential bonus‡ With EHR bonus ($25 per patient per year) 0 – 12,500 0 – 12,500 Patient education bonus ($5 per patient per year) 0 – 2,500 0 – 2,500 With care management bonus ($10 per patient per year) 0 – 5,000 0 – 5,000 Diabetes care link potential bonus§ Diabetes care link 0 – 11,400 0 – 13,000 Cardiac care link potential bonusII Cardiac care link 0 – 9,750 0 – 11,200 Total change in compensation (20,900) – 20,250 42,800 – 87,000 Total compensation under policy Total net physician compensation 146,600 – 187,750 210,300 – 254,500 - Table 13.
Change in Compensation per Physician Under New Model With Mixed Reimbursement Model
Payment Category With 18% Reduction in Hours Worked, $ With Current Work Hours, $* Source: Lewin Group estimates using illustrated assumptions.13 FTE = full-time-equivalent; HEDIS = Health Plan Employer Data and Information Set. Note: numbers in parentheses indicate loss. *Assumes physicians use savings in time worked to increase patient volume to maintain total hours worked per week. † Assumes all patients are enrolled in participating health plans. Assumes average panel of about 2,030 patients per FTE physician. ‡ Annual fee based upon the net cost of implementing the New Model (estimated net cost of $18,123 at current patient volume, rounded to $10 per patient). § Bonus of up to $80 per diabetes patient for high scores in providing diabetes care. Assumes 7% of patients are diabetic. II Bonus of up to $160 per cardiac patient for high scores in providing cardiac care. Assumes 3% of patients have cardiac conditions. ¶ Annual bonus amount based upon performance indicators up to $20,000 per physician. Current average compensation Mean compensation per FTE physician† 167,500 167,500 Changes in physician compensation per physician New Model under current fee-for-service model (taken from microanalysis) (20,900) 42,800 Annual New Model fee per patient‡ New Model fee per patient ($10 per patient per year) 20,300 23,300 Diabetes care link potential bonus§ Diabetes care link bonus 0 – 11,400 0 – 13,000 Cardiac care link potential bonus II Cardiac care link bonus 0 – 9,750 0 – 11,200 Annual performance reward¶ Performance award scored on: 0 – 20,000 0 – 20,000 Use of generic drugs Patient satisfaction survey HEDIS performance measures Total change in compensation (600) – 40,550 66,100 – 110,300 Total compensation under policy Total net physician compensation§ 166,900 – 208,050 235,500 – 277,800
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Health Is Primary: Family Medicine for America's Health
- Practice Transformation? Opportunities and Costs for Primary Care Practices
- Group Visits Hold Great Potential For Improving Diabetes Care And Outcomes, But Best Practices Must Be Developed
- Measuring Primary Care Expenses
- Effect of Facilitation on Practice Outcomes in the National Demonstration Project Model of the Patient-Centered Medical Home
- Implementing the Patient-Centered Medical Home: Observation and Description of the National Demonstration Project
- Cost to Primary Care Practices of Responding to Payer Requests for Quality and Performance Data
- Group Visits: A Qualitative Review of Current Research
- In This Issue: Glimpses of a Transformed Model of Care
- Time Spent in Face-to-Face Patient Care and Work Outside the Examination Room
- Physician Activities During Time Out of the Examination Room
- Prescription for Health: Round 1 Initial Results
- Stimulus, Response, Interpretation
- In This Issue: New Model Finances, Systematic Reviews, Patients and Health Care
- On TRACK