
Abstract
PURPOSE Gender-affirming hormone therapy (GAHT) is safe overall, with few adverse effects. One potential effect from using testosterone for GAHT is an increase in hemoglobin and/or hematocrit, known as secondary erythrocytosis. Current guidelines recommend monitoring hemoglobin or hematocrit routinely in the first year, some as frequently as every 3 months, which can create barriers to care. Our study explored the incidence of erythrocytosis in the first 20 months of testosterone therapy among people receiving gender-affirming care.
METHODS This is a descriptive fixed cohort study of hematocrit and hemoglobin data from the charts of 282 people taking testosterone for GAHT.
RESULTS During the first 20 months of testosterone therapy, the cumulative incidence of hematocrit >50.4% was 12.6%, hematocrit >52% was 1.0%, and hematocrit >54% was 0.6%. All people were taking injectable testosterone cypionate, with a median dose of 100 mg weekly.
CONCLUSION Severe erythrocytosis (hematocrit >54%) is a rare outcome of gender-affirming testosterone therapy. Clinical recommendations should reconsider the need for routine frequent erythrocytosis screening within the first year of testosterone therapy for patients who prefer to minimize laboratory draws.
INTRODUCTION
Gender-affirming health care includes hormone therapy, surgery, voice training, and additional inclusive medical and social services provided to transgender and gender diverse (TGD) individuals, including people who identify as nonbinary or gender nonconforming. These services have been linked to improved mental health outcomes and quality of life and reduced suicidal ideation.1-3 Family medicine physicians are well positioned to provide gender-affirming hormone therapy (GAHT) in their scope of practice and either report willingness to, or already do, provide routine care to transgender people.4-7
The use of testosterone for therapeutic purposes is considered safe overall, with relatively few identified adverse effects.8,9 Studies mostly among cisgender men with hypogonadism have demonstrated an increase in hemoglobin and hematocrit in the setting of testosterone therapy.9,10 Data linking elevated hemoglobin and/or hematocrit to arterial or venous thromboses has been correlational rather than causal, and the effect of erythrocytosis was no longer significant when factors such as smoking, blood pressure, or obesity were accounted for.11,12 Even so, given the correlation, current GAHT guidelines from leading organizations recommend monitoring hematocrit or hemoglobin levels at baseline and every 3 months during the first year of therapy.2,3 Secondary erythrocytosis from testosterone therapy has not specifically been implicated as a cause of thromboembolic events,13-16 however, and there is a dearth of longitudinal outcomes in this generally healthy TGD population receiving testosterone therapy. Moreover, there are no trials assessing outcomes for risk reduction in those identified to have secondary erythrocytosis. A growing body of research has investigated the incidence of secondary erythrocytosis in people taking testosterone specifically for the indication of GAHT. These studies show that while hemoglobin and/or hematocrit concentrations increase during the first year of testosterone therapy, values largely remain within normal limits.14,17,18
With any clinical recommendations, access to care must be considered. For TGD individuals, structural barriers such as cost, discrimination, excessive administrative burdens, a lack of clinician education about gender-affirming care, and institutional exclusions (such as unavailability of gender neutral restrooms) reduce access to medical care.19-21 Initiating GAHT can be a difficult and time-consuming process for the patient, and the need for continuous laboratory monitoring may pose an additional challenge. With the COVID-19 pandemic normalizing low- or no-touch visits, medical clinicians have been compelled to re-evaluate the clinical value of some in-person exams. These factors led us to further investigate the need for routine quarterly laboratory draws by determining the cumulative incidence of erythrocytosis among people receiving testosterone for gender-affirming care in the first 20 months of therapy.
METHODS
Study Design & Population
This is a descriptive fixed cohort study. This study was reviewed and qualified for exemption by the Institutional Review Board at Virginia Commonwealth University.
The study population included people aged 16 years and older who were prescribed testosterone for GAHT and received routine hematocrit or hemoglobin monitoring at any Virginia League for Planned Parenthood (VLPP) affiliate site between January 1, 2017, and December 31, 2019.
People were excluded from the study if they were taking testosterone before the start of the study period, did not have a baseline hematocrit or hemoglobin laboratory value, or had “insufficient data,” characterized as fewer than 2 hematocrit or hemoglobin values over their first 12 months of GAHT (Figure 1). We also excluded people with gaps in hormone therapy, defined as any period greater than 1 month where they had not taken testosterone for any reason. For those who met study criteria, we manually reviewed charts for the following data: hemoglobin and/or hematocrit laboratory values, testosterone prescription details, and patient age, height, weight, and smoking status. Where the data were not normally distributed, we reported median, minimum, and maximum. Information regarding self-reported race was also collected in order to describe the patient population. For those who had erythrocytosis, additional information regarding medical history was collected. R statistical software (the R Foundation) was used.

Exclusion criteria.
GAHT = gender-affirming hormone therapy.
Analysis
We calculated the cumulative incidence of erythrocytosis at each 3-month follow-up time point up to 32 months of testosterone therapy, using survival analysis and censoring of those lost to follow-up. Erythrocytosis was defined using the reference range for “men” provided by the laboratory. This range included values exceeding 17.5 g/dL for hemoglobin and 50.4% for hematocrit. In order to further evaluate the degree of erythrocytosis, we categorized the elevated hematocrit values into 3 levels that have been used as cutoffs for erythrocytosis in other manuscripts9,14,18: 50.4% to 51.9%, 52% to 53.9%, and >54%, where >54% is universally considered by guidelines to require intervention.15,22,23 Where hematocrit concentrations were missing but we had a hemoglobin value (14.5% of data points), we imputed the hematocrit by multiplying the hemoglobin by a calculated factor of 3.023, which was derived as the mean multiplying factor of all the complete data. For the group of individuals with erythrocytosis, we additionally reported prevalence of cigarette smoking and sleep apnea. Due to high loss to follow-up in the 32-month time period (Table 1), we presented the 20-month data throughout the manuscript.
Follow-Up Table for Erythrocytosis in Patients on Testosterone
RESULTS
Participants
Five hundred and forty individuals’ charts were initially identified as eligible for the study. After applying the exclusion criteria (Figure 1), 282 were included in the analysis, all of whom were taking testosterone cypionate except for 3 who were taking testosterone gel.
Demographic Features and Baseline Data
At GAHT initiation, median age was 21 years, minimum age 16 years, and maximum age 60 years. Of 282 individuals, 172 (61%) self-identified as White, 34 (12%) as African American, 5 (1.8%) as Asian, 2 (0.01%) as Native Hawaiian or Other Pacific Islander, and 69 (24%) preferred not to answer. At baseline, 10 individuals had hematocrit and/or hemoglobin that were above the normal laboratory reference range for “women” but within range for “men.” We included these individuals in the study, and only included incidences of erythrocytosis as defined by the reference range for “men” at their first follow-up or thereafter.
Incidence of Erythrocytosis
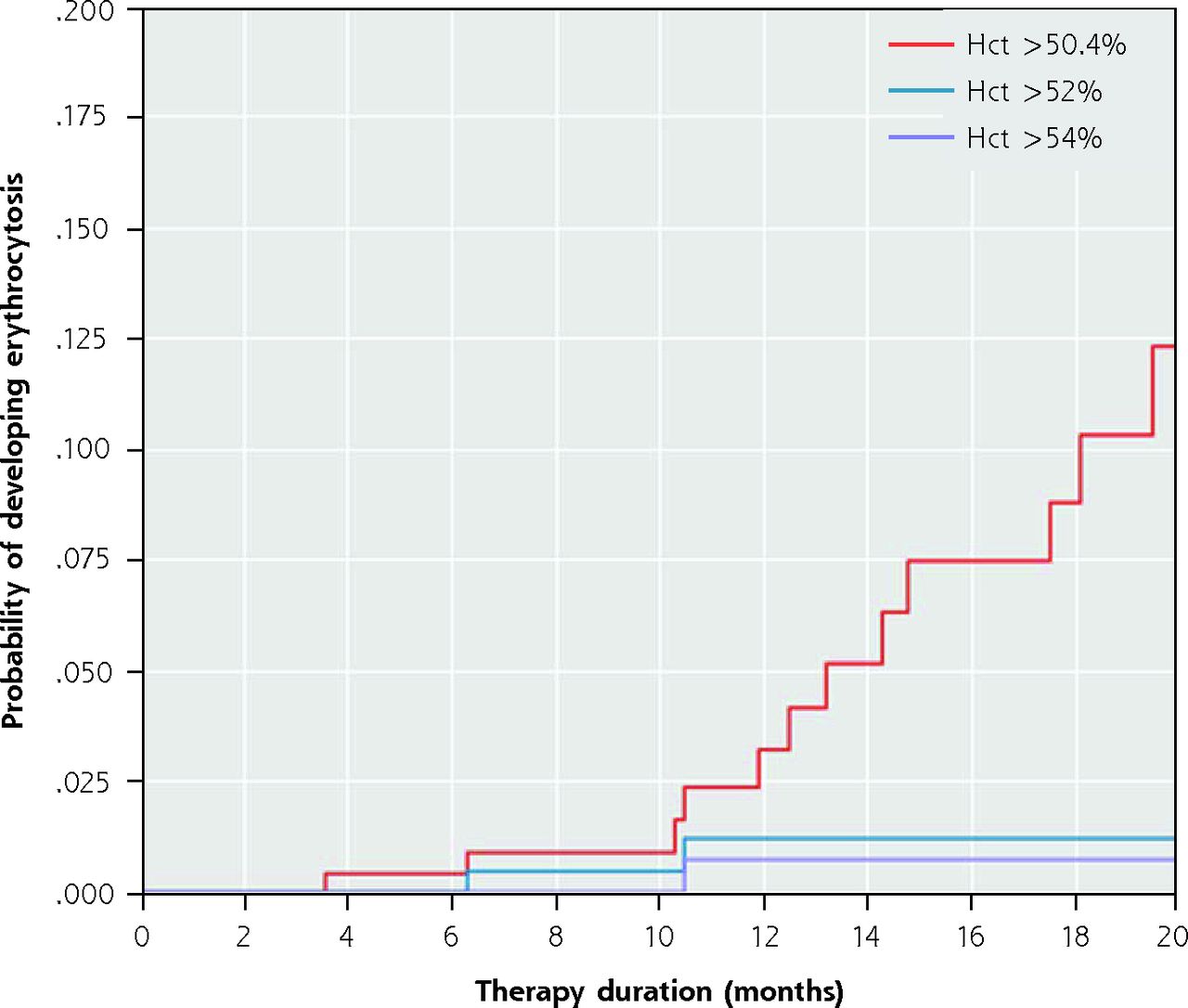
At 20 months, the cumulative incidence of erythrocytosis (hematocrit >50.4%) was 12.6%. The cumulative incidence of hematocrit greater than 52% was 1.0%, and the cumulative incidence of hematocrit greater than 54% was 0.6% (Figure 2).

Cumulative incidence of erythrocytosis over 20-month study period.
Hct = hematocrit.
Characteristics of Those Who Developed Erythrocytosis
For those who developed erythrocytosis within the first 20 months, at the initial time of erythrocytosis, the mean age was 26 years (SD = 6), mean duration on testosterone therapy was 12 months (SD = 5), and mean hematocrit was 51.4% (SD = 1.4). The median testosterone dose was 80 mg weekly (min: 40 mg, max: 120 mg), and the mean duration at current testosterone dose was 7 months (SD = 5). All participants who developed erythrocytosis were taking the testosterone cypionate formulation.
Among the 15 individuals who developed erythrocytosis in the first 20 months of therapy, 5 (33%) reported current smoking, and none had a documented diagnosis of sleep apnea at the time of testosterone initiation. Mean BMI was 33 (SD = 14). None had a known outcome of thromboembolism documented in their chart.
DISCUSSION
These results support a growing base of literature that suggests that although testosterone use is associated with erythrocytosis (defined as hematocrit >50.4%), severe erythrocytosis (hematocrit >54%) is uncommon among those who use testosterone as a medical intervention for gender affirmation. Furthermore, the clinical significance of this level of erythrocytosis in an otherwise healthy individual remains unclear. A recent study in Amsterdam found that among a group of 1,073 TGD people taking a variety of formulations of testosterone therapy for 20 years, 11% developed erythrocytosis (hematocrit >50%) over the 20 year duration, yet only 0.5% developed severe erythrocytosis (hematocrit >54% measured on 2 occurrences); they were unable to report on clinical interventions that may have occurred when hematocrit >50% was identified.18 Our study supplements these findings with data from people in the United States taking testosterone cypionate with weekly dosing (median dose 100 mg weekly), which is a commonly prescribed formulation and dosing frequency in the United States, rather than the higher dose (250 mg) every 2-4 weeks as in the Amsterdam study. Another recent study reviewing records for a US population showed that among 519 TGD people, up to 20% developed hematocrit >50% with a mean time-to-peak of 2.5 years.24 Importantly, this study was able to track outcomes through a database of patient hospital records and found that 0.9% (5/519) of the overall study participants had a thromboembolic event but none of these 5 patients had hematocrit >50% at the time of the event, and 4/5 had another inciting event or comorbidity.24
One of our study limitations was the high loss to follow-up throughout the 32-month follow-up period; 129 (46%) people remained in the study at 12 months and 71 (25%) at 20 months. Additionally, we did not document if the injectable testosterone was administered intramuscularly or subcutaneously; it is unclear if different routes of administration affect incidence of erythrocytosis. Another limitation is that we are not in a closed health system, so the fact that our patients with erythrocytosis did not have thromboembolic events documented in their charts does not guarantee that they did not occur. Further, our data on smoking status was difficult to access, which prevented us from investigating the prevalence of smoking in our overall study population compared with the subset that developed erythrocytosis. With cigarette smoking being a known risk factor for secondary erythrocytosis, this may be used as a marker to determine which individuals will need the frequent laboratory monitoring.18
Our findings show that routine erythrocytosis screening every 3 months in the first year of treatment for all individuals on testosterone may be unnecessary. We therefore suggest that those who draft clinical guidelines consider these findings, along with the summaries herein, in their screening recommendations. This may also be particularly true as more people identify as nonbinary or otherwise aim to be on lower doses of testosterone (eg, testosterone cypionate 40 mg weekly) compared with higher doses commonly prescribed in the past, and there may be a dose-dependence in development of erythrocytosis.18,25
When reviewing guidelines and protocols for clinical care with gender-diverse people, we must also consider the history and context of an oppressive medical system that has injured more often than it has healed.26 As gender diversity becomes more widely accepted, both patients and scholars make the case for the depathologization of the gendered experiences for TGD people.26 Allowing individuals to easily access their hormone therapy offers the freedom to utilize primary care in ways that they find most meaningful.27
We argue that drawing a hemoglobin/hematocrit laboratory routinely for everyone every 3 months is unnecessary, but there is tremendous value in integrating gender-affirming care into primary care, wherein patients can receive respectful assessment of their medical conditions and receive care that helps them address tobacco use, sleep apnea, and any other potential risks, not only for thromboembolic events but for any modifiable event.28 The extent of desired medical interventions (ie, surgery and hormone therapy) and monitoring varies greatly from person to person, and these individual preferences should be considered alongside medical risk factors to make monitoring decisions that best benefit each individual patient.
Acknowledgments
This study was made possible by staff and patients at Virginia League for Planned Parenthood. Thank you to the staff for their compassionate and LGBTQ+-affirming medical care. Thank you to the patients for engaging with a health care system that has only given them reasons to be skeptical. Thank you to Terence Rustia for data analysis and modeling.
Footnotes
Conflicts of interest: authors report none.
- Received for publication October 30, 2022.
- Revision received March 12, 2023.
- Accepted for publication April 12, 2023.
- © 2023 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}