Abstract
PURPOSE We wanted to design and validate the Hearing-Dependent Daily Activities (HDDA) Scale as a means of identifying the impact of hearing loss in older persons by measuring capacity to carry out hearing-dependent activities.
METHODS We undertook a cross-sectional, observational study to validate a scale administered during a personal interview with 1,160 participants aged 65 years and older. When using the instrument to identify patients with hearing impairment, sensitivity and specificity were determined using an audiogram with Ventry and Weinstein criteria as the criterion standard. Standardized audiometries were performed blindly, without knowledge of results of the HDDA Scale.
RESULTS According to the criterion standard, 506 participants had hearing impairment (43.6%; 95% confidence interval [CI], 40.8%–46.5%). The HDDA scale showed high internal consistency (Cronbach’s α =0.91). Regarding hearing impairment criteria, the HDDA scale obtained a sensitivity of 80.0% (95% CI, 76.3%–83.3%) and a specificity of 70.2% (95% CI, 66.5%–73.5%).
CONCLUSIONS The HDDA scale constitutes a clinically useful instrument for identifying the impact of hearing loss on daily life in the elderly, a condition frequently overlooked during routine medical check-ups. This tool has acceptable psychometric properties and high internal consistency.
- Hearing loss
- hearing impairment
- disability evaluation
- elderly
INTRODUCTION
Evidence exists that up to 25% of persons between the ages of 65 and 75 years have undiagnosed hearing loss that may be detectable through screening questionnaires.1 Despite the high prevalence of hearing impairment and the effectiveness of rehabilitation measures, family physicians do not normally make systematic use of hearing impairment screening tests or structured interviews for all older patients. Evaluation scales can be a rapid and easy means of assessing the impact of hearing loss on daily life if appropriately chosen for each situation and if previously validated in persons of comparable socioeconomic characteristics. Hearing loss can be improved by means of the correct diagnosis and treatment,2 thereby facilitating patients’ and family members’ understanding of the problem and providing the means to increase quality of life. Correctly fitted hearing aids frequently contribute to successful rehabilitation of the patient, resulting in a positive influence on the elderly person’s self-perception of health and on their daily life functioning.3 In fact, one major standard-setting organization, the US Preventive Services Task Force, currently recommends (“B” recommendation) screening of older adults for hearing impairment by periodically questioning them about their hearing, counseling them about the availability of hearing aid devices, and making referrals for abnormalities when appropriate. The optimal frequency of such screening has not been determined and is left to clinical discretion.
Some instruments most frequently used to identify the functional impact of hearing loss are often reputed to possess insufficient validity in the community-dwelling elderly.4 These scales include the Hearing Measurement Scale5 (25 items), the Social Hearing Handicap Index6 (20 items), the Hearing Performance Inventory7 (90 items), the Hearing Disability and Handicap Scale8 (20 items), the Hearing Handicap Inventory for the Elderly9 (25 items), the Hearing Handicap Inventory for the Elderly Screening test10 (HHIE-S) (10 items), or adaptations of the same in the Mexican population, such as the Spanish Hearing Impairment Inventory for the Elderly.11 The above-mentioned instruments often possess low sensitivity, not surpassing the 75% level4,12–14 in the case of the test currently used most frequently (HHIE-S). Accordingly, there is a need for new instruments of detection that are simple, rigorous, and adapted to the psychosocial characteristics of older persons, given that cultural patterns, education, and linguistic differences can have a major impact on the functioning of these instruments.
The object of our study was to design and validate the Hearing-Dependent Daily Activities (HDDA) Scale as a means to identify the impact of hearing loss on daily life in older persons by measuring capacity to carry out hearing-dependent activities. We considered tonal audiometry as the reference comparison standard, because it is markedly reliable in evaluating the hearing capacity of the elderly, their therapeutic needs, and functional prognosis.
METHODS
Design and Study Population
This observational, cross-sectional study consisted of 2 parts: (1) development of an instrument, and (2) validation of that instrument, administered by means of a personal interview. The study took place in the city of Albacete, Spain, which comprises 8 principal health zones and a population of 159,518 inhabitants, 13.4% of whom are aged 65 years or older. Study participants were residents of Albacete and aged 65 years and older. Exclusion criteria included cognitive disorders and immobilized elderly persons unable to reach the health center for audiometry testing.
We needed an estimated a sample size of 971 participants based upon an expected 35% of older persons with hearing problems (95% confidence interval ± 3%). Allowing for a 30% nonresponse rate calculated using the formula “adjusted number of subjects = number of subjects [1/ (1 − expected proportion of losses)],” the definitive sample size increased to 1,387 participants. Participants were selected by simple random sampling from a list of persons aged 65 years and older registered in the National Health Care system. Our validation study corresponds to a simultaneous design in which diagnosis (audiometry) and testing (HDDA Scale) are concurrently applied to a sample of the population. To maintain tester objectivity, audiometries were performed without knowledge of HDDA Scale results.
Study Instrument
To construct the questionnaire items, we took into account the characteristics of the population (cultural level, state of health, etc) and reviewed the instruments available to date for the detection of hearing impairment.9,11,13,15–19 We then formulated questions concerning the following aspects related to hearing loss in the elderly and its impact on daily life: self-perception of hypoacusis, perception of basic sounds, interference with hearing-dependent daily life activities, and impact on social activities. Initially, we included a greater number of items in each domain than what remained in the final version of the scale. All items were devised and selected by means of consensus among participating researchers, and questions were written in a neutral, clear, and simple style, requiring a minimum amount of time and concentration on the part of the patients in their responses.
Once the questionnaire was formulated, a first pilot test was conducted on 7 subjects. The object was to establish the clarity of the 19 questions initially constituting the scale (in terms of patient comprehension) and the clarity of the instructions contained therein, as well as to record the time required to complete the test (average age = 74.1 ± 5.4 years, average time = 4.7 ± 1.0 minutes). After observing difficulties in the comprehension of several questions, the questionnaire was reduced to 12 items. A second pilot test was carried out on 40 subjects to ascertain the reproducibility of the scale’s results. Twenty subjects were interviewed on 2 different occasions within less than 1 week and the other 20 were given consecutive evaluations by 2 different interviewers to determine reliability between observers. In Supplemental Appendix 1, the HDDA Scale is shown in English, and in Supplemental Appendix 2, it is shown in Spanish. Appendixes are online-only and available at http://www.annfammed.org/cgi/content/full/6/5/441/DC1.
Data Collection
We contacted Albacete residents selected for the study by mail and later by telephone to explain the purpose of the trial. Next, they were given appointments at Health Centre Zone VI in Albacete for evaluation by 3 nurses who were previously trained in the Department of Otorrhinolaryngology of the University Hospital Complex of Albacete.
With the purpose of reducing error during data collection, conditions of the scale administration were standardized for all interviewees. The population sample was selected to represent the population under study, including the entire clinical spectrum or comorbidity of hearing impairment. Because our research involved older persons with high levels of illiteracy, we preferred to conduct interviews in which relevant issues could be clarified rather than rely on self-administered questionnaires, even though the latter ensures greater patient privacy and may be more effective for information gathering.
The predictor variable was the score obtained on the HDDA Scale. Overall scores were calculated by arithmetically summing points received for each item, with higher scores indicating fewer difficulties in carrying out hearing-dependent activities. There were 3 response options for each question: “always” or “no, I can’t” (0 points), “occasionally” or “with some difficulty” (1 point), and “never” or “yes, without difficulty” (2 points). Finally, results were classified dichotomously into impairment present/absent, with established different cutoff points.
The criterion standard used in this study was measurement of hearing threshold using liminal tonal audiometry. Diagnosis of hearing impairment was determined according to the criteria recommended by Ventry and Weinstein,20 consisting of a hearing loss of 40 dB or more at 1 and 2 kHz in 1 ear, or at 1 or 2 kHz in both ears. Standardized audiometries were performed blindly, without knowledge of results of the HDDA Scale. Hearing function was also evaluated by means of The HHIE-S9,11,14,21,22 in its abbreviated version of 10 questions (cutoff point between scores of 8 and 10).
The study was approved by the Clinical Investigation Ethics Committee of the Health Region of Albacete. Throughout the course of the trial, the following ethical principles were maintained: voluntary participation, informed consent, guaranteed anonymity, and protection of data privacy.
Statistical Methods
Statistical analysis, performed using SPSS 14.0 (SPSS Inc, Chicago, Illinois), began with a description of participants. We used the intraclass correlation coefficient, based on analysis of variance and suited to reflect the changes in average values and the correlation between the distinct measurements, to test the reliability of the scale (intra- and interobserver consistency). We evaluated internal coherence of responses using Cronbach’s α reliability coefficient (correlation between responses to the distinct questions of the scale to evaluate homogeneity of items).
To evaluate content validity of the HDDA Scale, we assessed questions for the information they contained regarding different dimensions involved in identifying hearing impairment. The results of qualitative analysis indicated adequate validity of construction, showing that the contents of the scale were concordant with the theoretical concept of the disorder and comparable to that of other instruments which measure the same attribute. We explored the latent dimensions of hearing loss using factor analysis, consisting of the principle components analysis factor extraction method followed by orthogonal varimax rotation. We used the Kaiser-Meyer-Olkin index and Bartlett’s test of sphericity for factor analysis evaluation.
To assess criterion validity, we determined sensitivity and specificity of the scale with its corresponding 95% confidence intervals. Using the receiver operating characteristic (ROC) curve, we established the most appropriate cutoff point, which served as an index of the exactitude with which the HDDA Scale identifies hearing impairment in the elderly. Finally, to evaluate the clinical utility of the test, we calculated positive and negative predictive values and the probability quotient (likelihood ratio).
RESULTS
Of the 1,387 potential participants selected, we were able to conduct audiometry testing on 1,160, for a response rate of 83.6%. The average age of interviewees was 73.3 ± 5.9 years (range 65–96 years); 44.1% (512 cases) were men, and 55.9% (648 cases) were women. There was a predominance of married persons (77.2%), 67.7% of participants did not complete primary school (including illiterate and functional illiterate participants), and 61.9% had chronic health problems (of more than 3 months’ duration) (Table 1⇓).
Participant Characteristics (N = 1,160)
The reproducibility of the results of the HDDA Scale was evaluated in a sample of 40 older persons not included in the previous study (average age 70.7 ± 5.3 years), of whom 20 were interviewed on 2 different occasions less than 7 days apart to measure intraobserver reliability, while another 20 received 2 consecutive interviews by 2 different interviewers to determine interobserver reliability. Spearman’s correlation coefficients for intra- and interobserver reliability were 0.935 (P <.001) and 0.977 (P <.001), respectively; intraclass correlation coefficients for the same reliability measures were 0.932 (95% confidence interval [CI], 0.832–0.973) and 0.985 (95% CI, 0.963–0.994), respectively.
After determination of auditory thresholds using tonal audiometry in the 1,160 elderly participants, we found a hearing impairment rate of 43.6% (506 cases) (95% CI, 40.8%–46.5%) according to Ventry and Weinstein criteria.
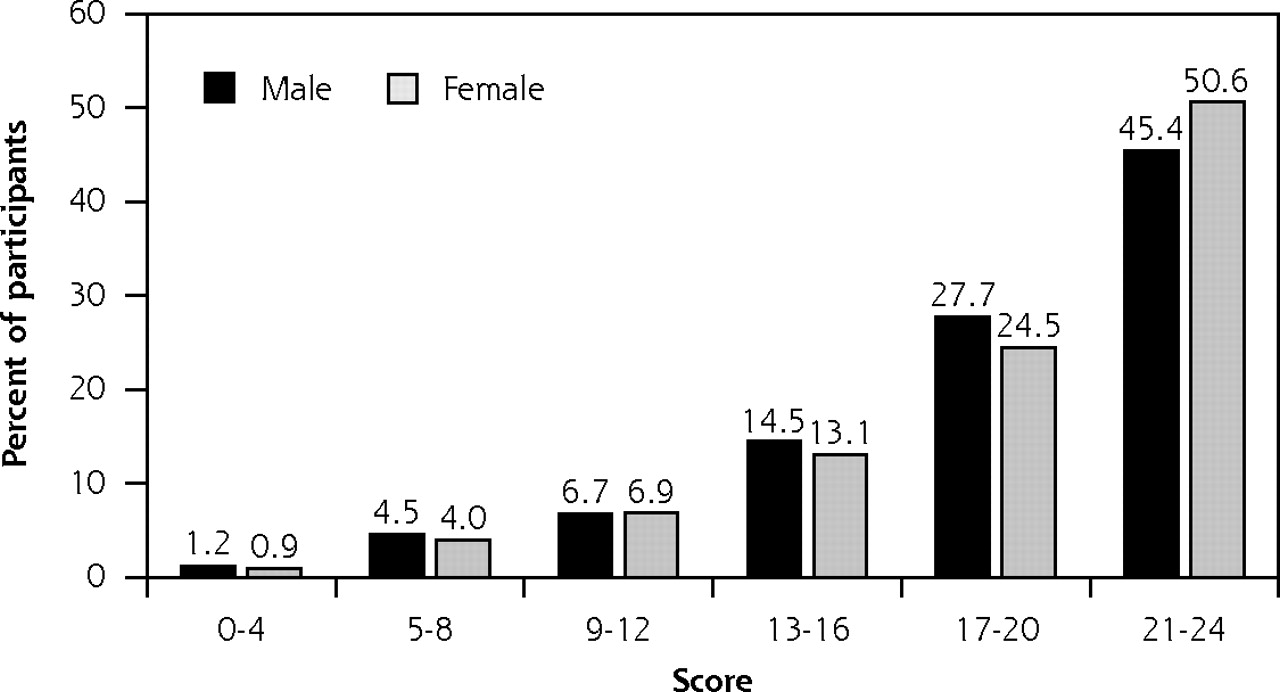
Table 2⇓ displays the items of the HDDA Scale and the distribution of responses. Participants’ scores ranged from 0 to 24, with an average score of 18.94 points ± 5.03 points. The percentage distribution of participants according to sex and score obtained on the HDDA is displayed in Figure 1⇓.
Distribution of Responses to Questions Contained in the Hearing-Dependent Daily Activities Scale (N=1,160 Participants)

Distribution of Hearing-Dependent Daily Activities Scale scores by participant’s sex (N = 1,160 participants).
The internal coherence of responses to items on the HDDA Scale was evaluated by means of Cronbach’s α (correlation between responses to the distinct questions to ascertain homogeneity of items); the scale was found to have very high internal consistency (Cronbach’s α = 0.91).
The latent dimensions of the scale were explored using factor analysis. Adequacy of the analysis was assessed by the Kaiser-Meyer-Olkin index (0.897) and Bartlett’s test of sphericity (9,690.36, 66 df; P <.001), allowing us to conclude that there were significant correlations between attributes. The factor analysis found 2 factors capable of explaining 65.5% of the total variance: (1) items related to degree of hearing loss and to its social impact for the patient, and (2) items indicating ability to perceive basic sounds. For each factor, items with highest saturation levels were included, and item content was interpreted to construct each of the dimensions of the scale. The factor loadings obtained for the items in the factor analysis are displayed in Table 3⇓.
Loadings Obtained for the Hearing-Dependent Daily Activities Scale Items in the Factor Analysis
In Table 4⇓, we display the validity parameters of sensitivity, specificity, and predictive values according to chosen cutoff point. Figure 2⇓ shows the ROC curve of the HDDA Scale, with an area under the curve of 0.822 (95% CI, 0.798–0.847). By means of this curve we calculated the most appropriate cutoff point for identifying hearing impairment, corresponding to a score of 20 or less on the HDDA Scale and a sensitivity and specificity of 80.0% (95% CI, 76.3%–83.3%) and 70.2% (95% CI, 66.5%–73.5%), respectively. Despite our use of a standardized, sufficiently proven hearing test to confirm a diagnosis, an imperfect criterion standard bias may have resulted in our potentially overestimating indices of sensitivity and specificity for the HDDA Scale.
Test Characteristics of the Hearing-Dependent Daily Activities Scale According to Cutoff Point (N=1,160 Patients)

{kind=link}
{kind=link}
ROC curve for HDDA Scale in detecting hearing loss in older adults (N = 1,160 patients).
ROC = receiver operating characteristic; HDDA = Hearing-Dependent Daily Activities.
We administered the questionnaire HHIE-S to 1,158 participants, yielding an average score of 2.9 ± 5.1 (range from 0–36). One hundred thirty-one participants scored above 10 points, considered to be indicative of a major hearing impairment (11.3% of those responding to the questionnaire; 95% CI, 9.5–13.1). On the other hand, 60.6% (702 cases) of interviewees did not manifest any hearing limitations (0 points). In response to the question, “How do you think your hearing is?”, we found that the majority (63.0%) described their hearing capacity as good or very good, 29.0% as “so-so” or not particularly good, and the remaining 8.0% as bad or very bad. When asked about the use of hearing aids, 52 (4.5%) of the elderly answered affirmatively.
Regarding hearing impairment criteria, the HHIE-S questionnaire obtained a sensitivity of 23.3% (95% CI, 19.8%–27.2%) and a specificity of 98.0% (95% CI, 96.6%–98.8%). The question pertaining to self-perceived hearing capacity classified as “so-so, bad, very bad” reached a sensitivity of 61.8% (95% CI, 57.5%–65.9%) and a specificity of 82.1% (95% CI, 79.0%–84.9%). Assessment of convergent validity of the HDDA Scale with respect to the HHIE-S questionnaire revealed a moderate to high correlation (r=0.776; P<.001).
DISCUSSION
Hearing impairment in the elderly patient may be overlooked in clinical practice, as patients and professionals tend to consider hearing loss as an age-related physiologic change. Because of the belief among physicians that treatment for hearing loss is ineffective, aid for this condition is frequently not given.15 Early detection is important, however, to reduce its impact on the functional state and social behavior of the older person.4,23–25 Moreover, it should not be forgotten that almost 90% of cases of hypoacusis are due to neurosensory changes and are amenable to hearing aids.26
Studies have shown that in primary care, identification rates of hearing disorders are low; heavy patient load and lack of time during office visits are likely contributors to this situation. Because only 20% of primary care physicians use some kind of screening method to identify hearing disorders,27,28 there appears to be a need for easy-to-use scales in clinical practice that aid not only the diagnosis of this condition but also evaluation of rehabilitation measures.29 To further these ends, the HDDA Scale shows adequate reliability indices and acceptable validity criteria. Most importantly, this instrument reaches a sensitivity as high as 80.0%, which is of interest when the primary aim is early detection of hearing loss in primary care practice. Specificity of the scale is modest, allowing correct classification of 70.2% of elderly patients with no hearing impairment. Our results indicate that the HDDA Scale may be more sensitive than other previously designed instruments in identifying older persons with hearing loss,13,18 and it may possess a higher predictive value than most items dealing with self-perceived hearing capacity.30 Because the positive predictive value of the HDDA Scale is conditioned by the increased prevalence of hearing impairment in the elderly, however, probability quotients are a less biased means of assessing the scale’s efficacy as a diagnostic tool.
For patients requiring special attention, such as the elderly, scales can be useful as aids to diagnosis and for measuring severity of the hearing condition, both during office consultations and in clinical studies. For maximum efficacy, it is essential that these tools are correctly adapted to the patient’s cultural environment and that they are endowed with robust psychometric properties. In this regard, the scale most utilized to date, the HHIE-S, has only minimally explored cultural differences in self-perceived hearing loss.31 Moreover, the instruments currently available for assessing hearing capacity frequently contain an excessive number of items, often multiple choice, which impede their successful completion and justify the attempts to simplify these scales. The HDDA Scale we propose offers ease of use, not only because of its simplicity, but also because of the short time required to complete it.
In conclusion, the aim of our study was to develop a clinically useful instrument to detect hearing loss in older patients, a condition that frequently goes unnoticed during routine medical check-ups. The HDDA Scale has been designed for use in primary care and may serve to easily identify hypoacusis and evaluate its impact on hearing-dependent activities. This scale was validated in a target population that approximated real-life conditions for diagnostic testing. Moreover, the HDDA Scale has good psychometric characteristics, which makes it an instrument that the family doctor can use to identify hearing impairment efficiently in clinical practice.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This study was financed by the Carlos III Institute of Health (Ministry of Health and Consumer Affairs Program for the Promotion of Biomedical and Health Sciences Research (Regulation SCO/3425/2002 of December 20th, File No. P1031562) and by the Ministry of Health of Castilla-La Mancha (Resolution 05-09-2003. D.O.C.M. No. 131 of September 12th, 2003).
- Received for publication September 2, 2007.
- Revision received February 28, 2008.
- Accepted for publication March 13, 2008.
- © 2008 Annals of Family Medicine, Inc.