
Abstract
PURPOSE The purpose of this study was to explore the responses of primary care clinicians to patients who complain of symptoms that might indicate depression, to examine the clinical strategies used by clinicians to recognize depression, and to identify the conditions that influence their ability to do so.
METHODS The grounded theory method was used for data collection and analysis. In-depth, in-person interviews were conducted with a purposeful sample of 8 clinicians. All interviews were audiotaped and transcribed.
RESULTS This study identified 3 processes clinicians engage in to recognize depression—ruling out, opening the door, and recognizing the person—and 3 conditions—familiarity with the patient, general clinical experience, and time availability—that influence how each of the processes is used.
CONCLUSIONS The likelihood of accurately diagnosing depression and the timeliness of the diagnosis are highly influenced by the conditions within which clinicians practice. Productivity expectations in primary care will continue to undermine the identification and treatment of depression if they fail to take into consideration the factors that influence such care.
INTRODUCTION
Underrecognition of depression in primary care is a critical public health problem1–,7 that has high societal costs related to disability,8,9 morbidity,10,11 mortality,1 and excessive health care utilization.12–,15 During the past decade, published findings of studies concerning the recognition of depression in primary care settings identified several potentially important influences: clinician characteristics, such as gender, years of practice, training background,16–,21 and setting22; patient characteristics and symptom presentation23–,26; and health care system variables, such as salary or capitation reimbursement.27
Although these studies have broadened our understanding about factors that can influence clinicians’ recognition and treatment of depression, they do not identify how those factors come into play in everyday practice of depression care. In rigorous pursuit of the US goal to promote high-quality mental health care, a number of research studies have indicated that targeting clinician knowledge alone does not increase the likelihood of recognizing depression.28–,38 A new line of research suggests that clinician-patient interactions in the context of everyday practice may be an important component in recognizing depression.39–,47
No study has thus far examined how the conditions of everyday practice operate in clinical decision making related to depression care. This study was designed to explore the relationships among the conditions of clinical practice, patient-clinician interactions, and the likelihood that clinicians will recognize depression in their patients complaining of ambiguous symptoms.
METHODS
The grounded theory method was used to guide sampling, data collection, and data analyses.48 Based on symbolic interactionism,49 grounded theory is most useful in research that seeks to explicate the relationship between actions and understandings to illuminate the perspectives of subjects and how these perspectives influence action. The method is designed for in-depth exploration of how conditions influence the phenomenon of interest (in this study, recognizing depression).50,51
Sampling and the Sample
Grounded theory relies on a purposive sampling technique (eg, theoretical sampling) that is driven by ongoing analysis. Sampling decisions are made to facilitate the constant comparison of cases and to identify sources of variation. In this study, sources of influence and variation in clinicians’ decision making regarding depression recognition were identified from interviews with clinicians and from published research. Sampling was determined to enhance analysis of whether and how these factors influenced the recognition of depression by the clinicians interviewed for the study. In response to published literature, theoretical sampling was initially done to explore the impact of time available for patient encounters. As the analysis proceeded, it became clear that other factors—familiarity with patients, extent of clinical experience in general, and the patients’ recognition that depression might be the source of the symptoms, for example—were also influential in both the likelihood that clinicians would recognize depression and speed with which they might do so. Theoretical sampling was therefore done to examine the impact of these factors, leading to a final sample that included variation in time pressures, general clinical experience of the clinician, and the patients’ identification of depression as a possibility.
The final study sample included 8 clinicians from the 3 groups: family physicians, general internists, and nurse practitioners. We reached theoretical saturation on the conditions that influence the sorting processes in which clinicians engage; that is, time available, years of experience, and familiarity with the patient continued to explain variations in the symptom-sorting process and in the likelihood of recognizing depression. This finding was consistent across the clinicians, regardless of training or specialty.
Data Collection
Using a letter approved by the University of Wisconsin Institutional Review Board as an invitation, in-depth, face-to-face interviews were conducted with 8 primary care clinicians in 3 primary care settings. Early interviews were deliberately broad and open, using unstructured questions, such as, “Tell me about your work here,” and “Tell me about seeing patients here.” The data from these 2 interviews were then used to develop conceptual categories and guide ongoing data collection. Several questions were asked in every interview (Table 1⇓), whereas other questions evolved to fill in theoretical gaps as the analysis progressed. Drafts of ongoing interview questions were developed and discussed in 2 grounded theory research groups. Interview probes were used as needed throughout the interviews to clarify, expand, and compare what was being talked about. For example, when familiarity with a patient emerged as a condition for recognizing depression, clinicians in subsequent interviews were asked to compare how their approach to familiar and unfamiliar patients differed.
Initial Interview Questions
Data Organization and Analysis
All interviews were audiotaped and transcribed. Grounded theory coding schemes—open, axial, and selective—were used to analyze the data. To promote reliable interpretation of the data, we used 2 experienced grounded theory research groups. Group analysis increased sensitivity to and awareness of assumptions that the researchers might have brought into the analysis and opened the analysis for interpretation across a broad range of perspectives. In the same vein, we also talked openly about our preconceptions and expectations related to primary care clinicians’ care of depression. For example, one preconception was that the conditions under which a clinician works (eg, time) would influence his or her care for patients with depression. After an analysis of each interview, data matrixes were developed to organize categories with indexes to supporting quotes and succinct descriptions of relationships among the emerging theoretical categories.
RESULTS
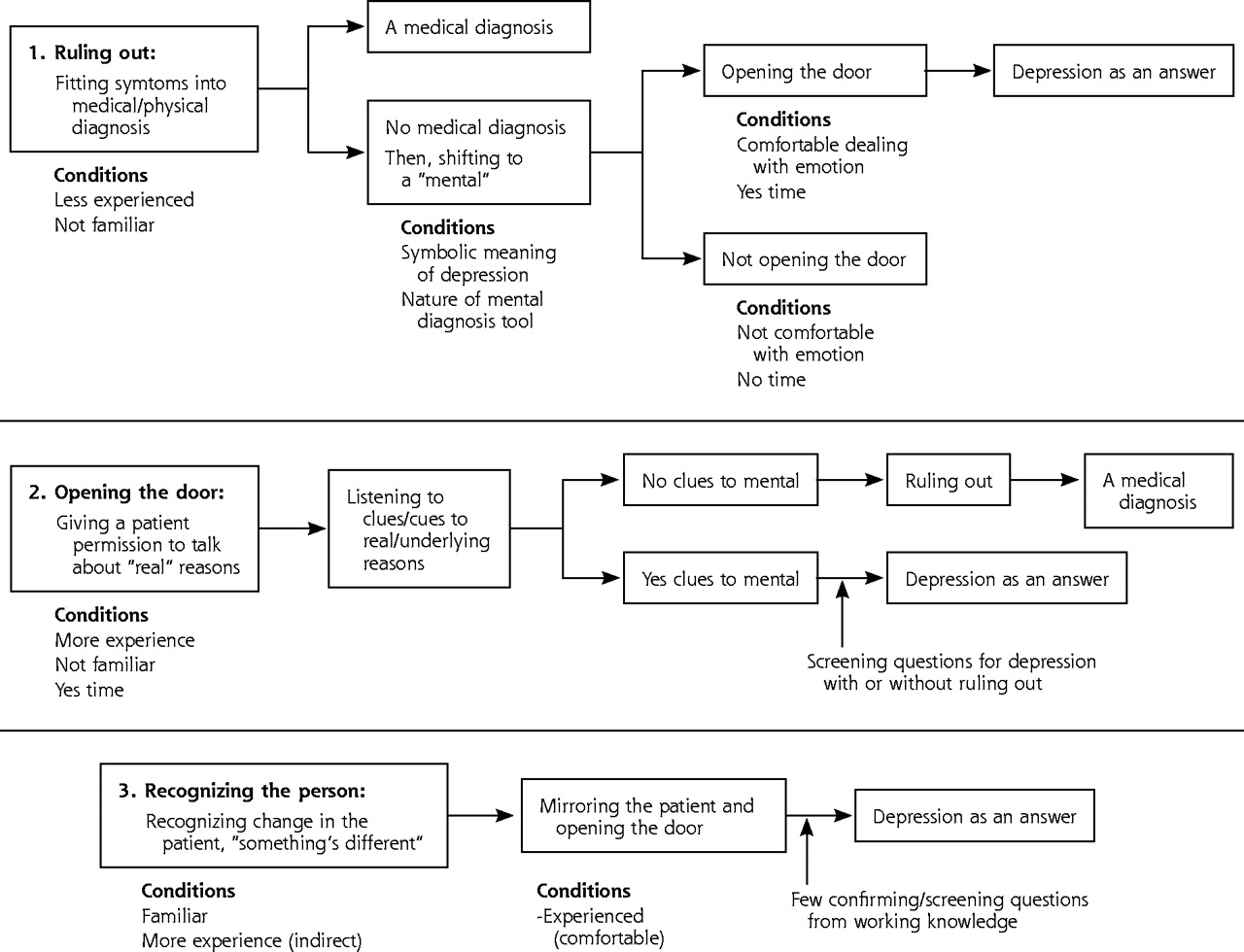
Patients seen in primary care settings often report symptoms that are unclear and could indicate any of several diagnoses, including depression. Even when clinicians suspect depression, they engage in a sorting process, ruling out physical causes first. Under such situations, clinicians engage in some combination of 3 processes to assist in sorting through the symptoms and arriving at a diagnosis: ruling out, opening the door, and recognizing the person. How these processes are used and the speed with which clinicians sort through the symptoms are influenced by 3 conditions: familiarity with the patient, clinical experience, and time availability (Figure 1⇓).
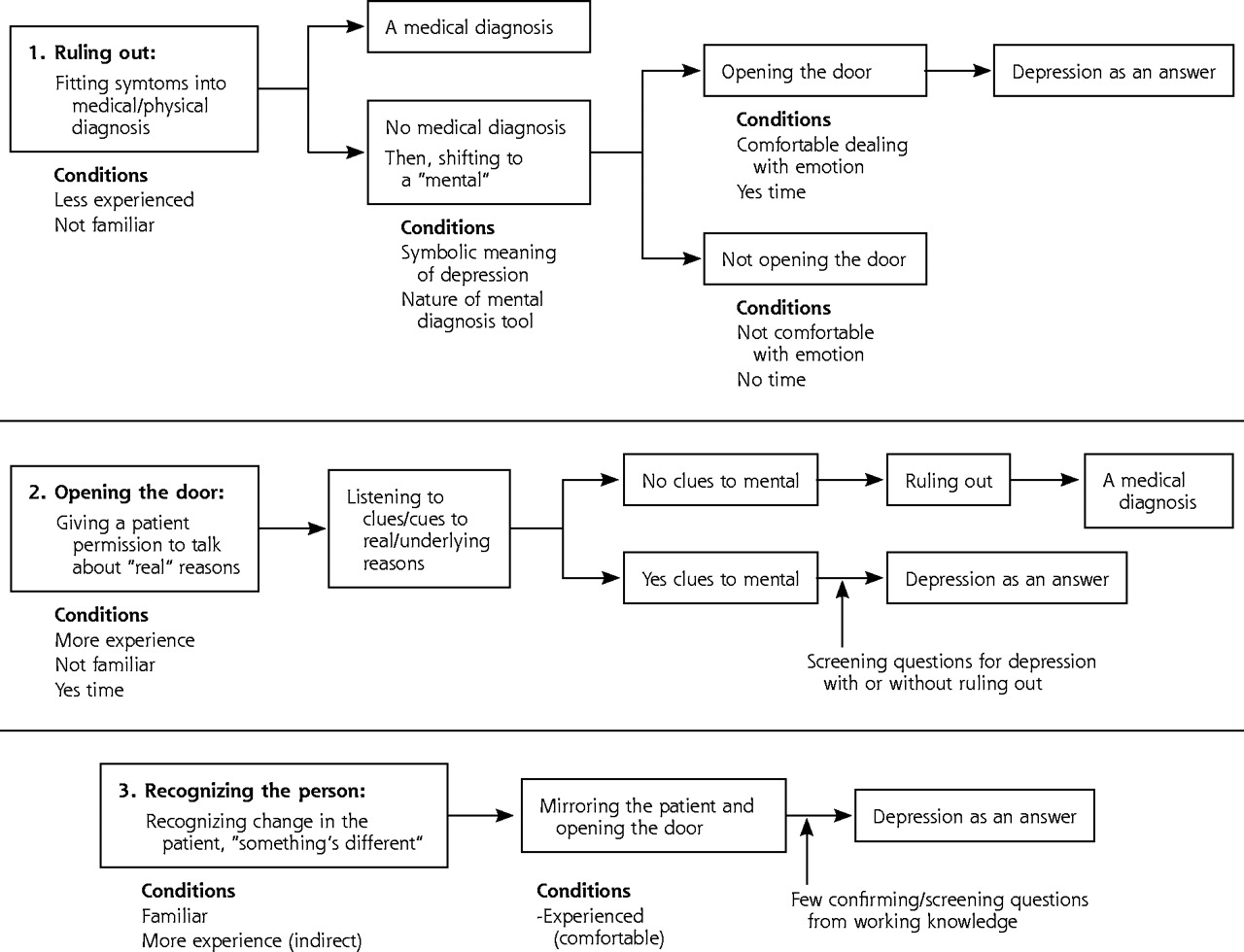
Preliminary model of clinicians’ recognition of depression: conditions under which patients report multiple issues without interpretation, and 3 possible processes by which clinicians recognize depression.
Ruling Out
When patients complained of symptoms that might indicate depression but did not identify themselves as depressed, clinicians responded by thoroughly sorting through the patient’s symptoms. Even when clinicians suspected depression, they considered a broad range of possibilities in the initial sorting of symptoms. This sorting began with a ruling out of organic causes. Ruling out generally began with fitting symptoms into a medical-physical (vs mental health) diagnosis. This medical explanation gave clinicians a framework for understanding symptoms—they could fit the symptoms into a medical diagnosis.
A lot of times people who come in with fatigue … I’m tired, I’m just tired all the time. Well, immediately you start thinking this could be cardiac, it could be heart failure, it could be lung failure, it could be a metabolic problem.… So it just becomes part of a differential diagnosis. [Nurse practitioner (NP)1]
Two characteristics of depression—the subjective nature of the symptoms combined with an absence of corroborating physical evidence and the stigma associated with the diagnosis—often prolonged the ruling out process, delaying the diagnosis of depression. The societal stigma of mental illness and current and more subjective methods to diagnose depression that rely on what the patient says (rather than on a biological or objective marker) led clinicians to rule out other possible medical causes before shifting their thinking to the possibility of a mental illness, such as depression.
I think it’s a bit threatening to the patient to suggest that they may have a mental illness.… So you don’t want to jump to that conclusion quickly. You may want to … give it some thought. [General internist (GI)1]
I won’t force them [patients] into accepting it [depression], I mean you CAN’T! The patient has to agree, because depression is a little different in that there’s so much subjectivity to it. You know, like diabetes, if I say … and I’ve had patients say, “I don’t think I have diabetes.” And I’ll say, “YES! YOU DO, because your blood sugar would not be like that unless you had diabetes. You might not feel like it, but you do.” But depression, it’s not like that. Because if I say, “You are depressed,” and you say, “No I’m not,” the only thing I can say is, “Well, here’s how you feel, and you’re the one who knows how you feel.” There is no real objective measure for that. It’s a subjective feeling of your emotional state. So it’s not like I can prove to somebody that they’re depressed. I can tell them that it’s my OPINION that they have a lot of symptoms of depression and that they may be depressed, but they have to accept it. [Family physician (FP)2]
Familiarity with the patient was found to be an important condition. When clinicians were not familiar with the patient, the subjective nature of the symptoms and the social stigma associated with depression increased the reluctance of the clinician to diagnose depression. In addition, when clinicians were not familiar with the patient, they acknowledged that the patient was less likely to share personal information, making diagnosis even more difficult. The general experience of clinicians also influenced the process. Clinicians’ reluctance to suggest depression early in the visit increased when clinicians had less general experience. Lack of familiarity and less general experience led clinicians to exhaust medical diagnoses before considering or suggesting a mental health diagnosis.
Extensive ruling out was used to avoid missing a medical condition or upsetting the patient. As a consequence, recognizing depression was often delayed. In contrast, when clinicians were familiar with the patient, the ruling out process was considerably shortened. The clinician often explicitly compared the familiar person she or he knows with the person in the room, highlighting differences that might suggest depression. While this process is effective and results in much quicker identification of depression, it can be used only when the clinician is familiar with the patient.
When somebody comes in new, I really don’t have any information on them at all from previous appointments, and it’s kind of like starting from scratch. Because sometimes things don’t come out in their history.… “Do you have any history of health problems?” and they’ll say, “No.” Whereas they might have a lot of things that just aren’t at the point where they want to divulge it. I spend more time kind of getting to the bottom of it. [NP2]
Opening the Door
Opening the door was defined as allowing the patient to talk about whatever was bothersome, which most experienced clinicians saw as inviting patients to share the real reasons for the visit. Diagnosing a mental health condition such as depression requires the patient to share highly personal information, and gathering this personal information is crucial to diagnosing depression. When patients do not share information, the diagnosis is delayed. Such sharing is less likely with unfamiliar patients. By opening the door, these clinicians often could delve into personal information relatively early in patient encounters. Clinician experience also influences this process. Less experienced clinicians were more likely to express discomfort with opening the door and talking to patients about mental health issues. Clinicians with more experience (14 to 28 years), however, described how they gradually became more comfortable with opening the door to a conversation about depression and listening to clues about the real reason for the visit.
Experienced clinicians were more willing to use this strategy, especially with unfamiliar patients. Experienced clinicians believed that unfamiliar patients were much less likely to divulge personal information, so they deliberately open the door to patients early in the encounter to gather personal information. Experienced clinicians also described how they learned to recognize a patient’s verbal as well as nonverbal cues, whether the real issues have surfaced, and whether the patient is prepared to discuss them.
I do a lot of early work with patients now that I didn’t do 20 years ago … to say, “What are you worried it might be?” “Why did you come here today?” So I start to get at some of the things I think are real reasons why they came. [FP1]
They give you some nonverbal cues or they give you verbal cues, such as they’ll say, “BY THE WAY, there’s something else bothering me.” Or when they’re all finished, they’ll look like there’s still something else going on. They won’t say, “Thank you,” and get up and leave.… They will often switch the discussion if they don’t want to discuss it. [FP3]
Time availability also influenced a clinician’s willingness to open the door. If clinicians felt rushed and were catching up when they encountered such a patient, they were unlikely to open the door. Even when these clinicians were comfortable discussing emotions and considered depression a likely diagnosis, they anticipated that such discussions would be time consuming and avoided opening the door.
Recognizing the Person
Clinicians described recognizing the person as comparing the person in front of them with the person they know. Recognizing the person appeared to be an alternative (and often much quicker) process to ruling out or opening the door for expediting the depression-recognition process with familiar patients. When clinicians were familiar with patients, their perception of who the patient is compared with who the patient appears to be offered a clue to diagnosing depression. Although the clinicians could not fully elaborate what “knowing the patient” meant, it allowed them to read the patient’s behavioral language better, such as facial affect and body posture, when they were familiar with the patient. Clinicians also stated that, when they know the patient, they could recognize change early in the encounter, often within a few seconds to a minute. Once a level of suspicion has been established with familiar patients, clinicians could raise the possibility of a mental health diagnosis by asking the few screening questions they have found to be useful rather than going through the DSM list of symptoms. The 2 symptoms most often used to screen for depression were sleep problems and low energy level.
I had an experience almost 20 years ago with a very experienced general practitioner in Wales, in Britain. I watched him for a little while. One time he says to me, “Do you watch how I work? What I do is I pay complete attention for the first 15 seconds the patient is in the room. I use all of my senses, and I pay attention.” And he says, “I can get a feeling of what’s going on in the first 15 seconds.” You know, I thought this guy’s crazy. But actually—especially for people you know—he knew all of those patients, those were old patients of his. And he’d walk in and he’d say, “What’s the trouble?” And they’d say, “Why do you think there’s something that’s trouble?” And he says, “I know you, you look different, you seem different, you act different.” And it is true with people you know. Now think of people you work with regularly, and you walk in and you see them, and they look different or they seem different. Then you know something’s different. And whether they say, “No, I feel fine,” or not, reality is something different. Now whether it’s good or bad is not the issue, it’s different. So with my patients, it’s the same way. I actually … I see it in their faces, I see it in their bodies, I see it in how they make eye contact with me when I come in, I hear it in their voices. I mean, this old man, Dr. Williams, was right. It’s in the first 15 seconds, you KNOW something is different. [FP1]
Recognizing depression through recognizing the person seems to occur simultaneously with knowing the patient and being comfortable dealing with emotions. First, to recognize change in the patient, the clinician must know the patient and be willing to reflect this possibility verbally. More importantly, however, time availability overrides these 2 conditions. Even if the clinician recognizes change and feels comfortable dealing with emotions, time constraints often prevent clinicians from opening the door to patients.
DISCUSSION
Decades of effort to improve clinical decision making have yielded countless symptom-based diagnostic criteria intended to facilitate diagnostic reasoning.52–,54 Although such criteria are valuable in differentiating symptoms and in diagnosing illness, selective attention to patients’ symptoms and subsequent interpretation are subject to the conditions under which interactions between the clinician and patient occur.
The findings from this study suggest that primary care clinicians’ detection of depression may involve more than the clinician’s ability to recognize symptoms. Contrary to the depression care quality improvement efforts during the past decade that focused primarily on education, our study findings suggest that lack of knowledge may have little to do with recognition of depression in primary care. Rather, the likelihood of accurately diagnosing depression and the timeliness of the diagnosis may be highly influenced by the conditions within which clinical decision making occurs. In primary care settings, where patients come in with multiple issues and symptoms and where the possibility of a mental health diagnosis is often not stated as such, clinicians begin the process by sorting through multiple symptoms and ruling out physical and organic causes.
Knowing the patient allows clinicians to recognize depression quickly, bypassing much of the sorting and ruling out what is otherwise necessary. Experienced clinicians seemed more comfortable asking about the patient’s life and gathering personal information. They are also more likely to open the door early during the patient encounter, which may lead quickly to recognition of depression. Even an experienced clinician, however, may decide not to open the door when behind schedule or pressured to work quickly, raising serious questions about clinicians’ ability to respond appropriately to depressed patients in brief encounters. In contrast, clinicians agreed that short primary care visits could be sufficient to recognize depression if the clinician knows the patient, suggesting the importance of patient continuity, especially in time-constrained practices.
During the past 10 to 15 years, most studies of depression in primary care have conceptualized influencing factors as separate variables and have left gaps in understanding the process of how these factors may come into play in clinical encounters of the everyday practice environment. The strengths of this study lie with the treatment of the clinician-patient clinical encounter as a mediating variable. That is, the impact of system factors, as well as any other factors, on the outcome of depression care is mediated through the clinician-patient encounters.
This study has several major limitations. First, a sample of 8 clinicians was barely enough to illustrate that there is more than one process of recognizing depression, to identify the conditions and contexts under which clinicians encounter patients, and to map how they influence the process. In the same vein, had the sample size been larger, the possible differences among the clinician groups could have been more confirming. Second, given the time limits, several theoretical sampling possibilities were not pursued. Experience as a condition for primary care clinicians’ recognition of depression could be explored more in depth had this study used theoretical sampling of 2 distinct groups of clinicians, such as very new and very experienced clinicians. Third, the term experience in this study was used as a proxy to depict multiple dimensions of what clinicians phrased as “as you practice.” The term experience, however, connotes only years of practice; therefore, in future studies the investigators will continue to search for a better proxy to capture experience. Experience appeared to be closely related to being comfortable dealing with emotions.
This study was designed to illuminate the range of processes that clinicians use to arrive at outcomes and the multiple factors and conditions that influence such processes. As such, it is a first logical step to determine where limitations and inadequacies lie in those processes so that quality improvement interventions can be designed. Identifying processes and influencing conditions for the care of depression in primary care require a conceptual and methodological step back from assuming that there is only one right way. Identifying multiple processes and influencing conditions to arrive at a desirable performance level could be leveraged in future interventions. Because this study is a first qualitative step toward building interventions, it would be premature to identify fully the processes and conditions for designing future interventions. Our findings suggest several possibilities, however. For instance, clinicians who are comfortable with emotions tend to ask patients psychosocial (perceived as personal) questions that can lead to a more timely recognition of depression, suggesting that clinician education about symptoms of depression alone would not likely lead to recognition of depression. A better use of organizational resources might be to facilitate clinicians’ comfort in dealing with emotions through interventions aimed at increasing emotional competence in patient interaction, which could be tailored to the individual clinician, as well as groups of clinicians and clinicians-to-be. Another leverage point inferred from the findings is to improve clinicians’ familiarity with their patients, which might be addressed by augmenting continuity of care within organizational delivery structures.
Acknowledgments
The authors thank the University of Cincinnati and the University of Cincinnati College of Nursing for the funding of the secondary analysis of the data and the preparation of this manuscript. The authors also thank Carolyn Dawson, PhD, David A. Kindig, MD, PhD, Susan Riesch, DNSc, and Bonnie Svarstad, PhD, for their discussion in the development of this study.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This study was supported by the University of Cincinnati (UC) and UC College of Nursing.
- Received for publication March 24, 2004.
- Revision received September 12, 2004.
- Accepted for publication September 20, 2004.
- © 2005 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- Development and psychometric evaluation of a questionnaire for the assessment of depression in primary care: a cross-sectional study
- Self-Rated Health and Long-Term Prognosis of Depression
- Suffering in Silence: Reasons for Not Disclosing Depression in Primary Care
- Managing Depression Among Ethnic Communities: A Qualitative Study
- Reinvention of Depression Instruments by Primary Care Clinicians
- Recent trends in the incidence of recorded depression in primary care
- What Comprises Clinical Experience in Recognizing Depression?: The Primary Care Clinician's Perspective
- Do ultra-short screening instruments accurately detect depression in primary care?: A pooled analysis and meta-analysis of 22 studies
- Mothers' Comfort with Screening Questions about Sensitive Issues, Including Domestic Violence
- Predictors of Physician-Patient Agreement on Symptom Etiology in Primary Care
- Stimulus, Response, Interpretation
- Depression Research in Primary Care: Pushing the Field Forward
- In This Issue