
- social determinants of health
- primary health care
- population characteristics
- medical informatics
- data collection
SOCIAL DETERMINANTS DRAMATICALLY INFLUENCE HEALTH
The United States falls behind other industrialized nations on most health indicators1 and remains plagued by stark health disparities.2 Efforts to understand the factors underlying these persistent inequalities and other shortcomings highlight the role of social determinants of health (SDH).
SDH are the nonclinical factors, such as the socioeconomic conditions and neighborhood resources, that influence patients’ health outcomes.3 The World Health Organization defines SDH as “the conditions in which people are born, grow, work, live and age and the wider set of forces and systems shaping the conditions of daily life.”4 A rich body of literature shows that SDH are associated with morbidity, mortality, and other health indicators.5–12 There is mounting evidence to suggest that SDH influence health outcomes more than medical care.13 Even so, attempts to address SDH in medical care settings have been limited and, for the most part, ineffective. Serious efforts to reduce health disparities and improve population health will require innovative solutions for systematically addressing SDH in all primary care settings.14,15
ADDRESSING SDH IN PRIMARY CARE SETTINGS
Primary care, the largest health care delivery platform in the United States, is widely regarded as a natural point of integration and coordination between clinical care and public health, behavioral health, and community services.16 Recognition of and attention to non-medical factors that influence health are not new concepts in primary care. Some primary care clinics in the early 1900s employed peer health aides and provided recreation and welfare activities for their communities, as well as more formal health care services.17 These early health centers focused on health promotion and education, seeking to address poor nutrition and other SDH.17 The recognition that social determinants influence health fueled the creation of community-oriented primary care concepts in the 1940s,18–20 the development of family medicine as a medical specialty in the late 1960s,21,22 the passage of legislation to create the neighborhood Health Center Program in 1964 (predecessor to federally qualified health centers),23 and the Alma-Ata declaration in 1978, which stated that “primary health care…is the first level of contact of individuals, the family, and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first elements of a continuing health care process.”24
Primary care has a tradition of partnering with patients, communities, and public health professionals to attempt to address SDH,25–27 yet the ability to act on SDH in medical care settings in a meaningful, systematic way has been constrained by a fee-for-service payment structure, a medical culture focused on treating disease rather than promoting health, and limited technologies, among other barriers.28 Recent changes in health care policy, however, including the passage of the Patient Protection and Affordable Care Act, paired with rapid advances in data and technology, have presented opportunities for a paradigm shift in primary care delivery. Payer experiments, such as the Comprehensive Primary Care Initiative, Accountable Care Organization pilots, and Medicare Access and CHIP Reauthorization Act legislation have created new incentives to pursue population health and value-based care.29 Simultaneous efforts to transform the primary care delivery platform, such as the patient-centered medical home model,30–32 are increasing the capacity of primary care teams to address patients’ health needs in a broader context and implement “upstream” interventions.28,29 Concurrently, technological advances have made it possible to better integrate SDH data into electronic health records (EHRs),33,34 facilitate primary care teams’ efforts to address patients’ SDH,35 and enable teams to coordinate community service referrals and other SDH-related actions.25,35
INTEGRATING SDH DATA IN PRIMARY CARE
The technological advances described above have the potential to eliminate important structural barriers to addressing SDH. Notably, health information technology now yields viable methods for standardizing the collection and presentation of SDH data. Since the passage of the Health Information Technology for Economic and Clinical Health Act in 2009, the use of health information technology, particularly EHRs, has dramatically increased.36 In 2011, the Center for Medicare and Medicaid Service launched the 3-stage EHR Incentive Program, which provides incentives for clinicians to show meaningful use of EHRs in activities that include patient engagement, reducing health disparities, and improving care coordination and population health.37
Many primary care practices already document select patient-reported SDH (eg, race/ethnicity, income, employment) and seek to engage in activities to address them (eg, social service referrals).38,39 To date, however, most SDH data collection in primary care is manual and not standardized. Only a limited range of social determinants known to affect health outcomes are documented, and the SDH data that are collected are rarely presented to care teams via automated structures designed to support care delivery, clinical decision making, and collaboration among multiple service organizations.39 The National Academy of Medicine (NAM, formerly the Institute of Medicine) recently recommended that 11 SDH domains be routinely collected and made available in EHRs, recognizing their potential to galvanize action on these domains in patient care, as a part of the third stage of meaningful use requirements.29,40 A few of these domains are already collected in most primary care settings, such as alcohol use, race and ethnicity, residential address, and tobacco use. The NAM-recommended routine collection of additional domains includes census tract-median income and patient-reported depression, education, financial resource strain, intimate partner violence, physical activity, social connections or isolation, and stress.29,40 Partnership between public health and primary care is likely to facilitate at least some of this expansion of relevant data for care of patients, families, and communities.
A FRAMEWORK FOR INTEGRATING SDH INTO PRIMARY CARE
The NAM identified actionable SDH domains for inclusion in EHRs; now we must learn how to use SDH data most effectively to improve health. Standardizing the collection and presentation of SDH data in EHRs could help primary care teams incorporate such data into clinical decision making and more actively address SDH, but we know very little about how to make this happen.41 How can we make SDH-related information easily accessible at the point of care and facilitate panel management and population health efforts? How might primary care teams integrate SDH data into existing care paradigms or use this information to create new ones?
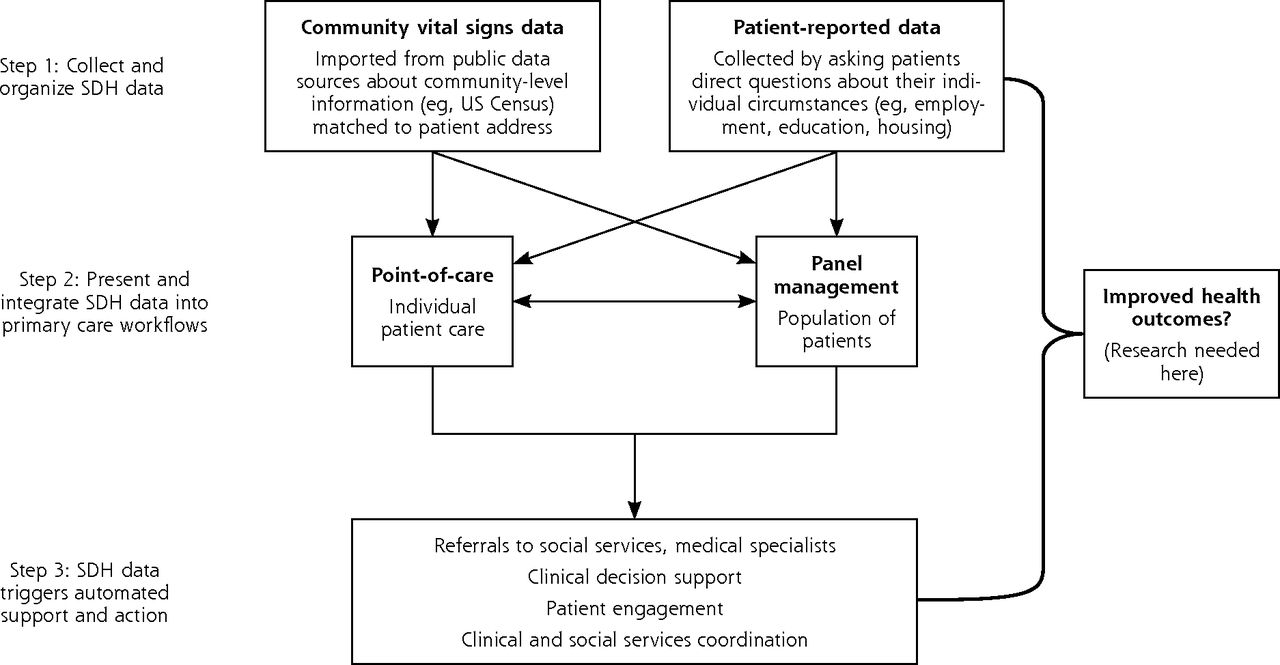
While developing a research agenda to help inform and evaluate efforts to address SDH in health care settings, we created a framework that outlines the integration of SDH into primary care practice, with specific ideas for how SDH information might prompt action (Figure 1). The first step is collecting and organizing the data in a systematic way. SDH data include community-level and individual-level information. Both apply to the individual patient, but individual-level data are reported by the patient (eg, patient reports household income below poverty line, dropping out of school after 8th grade, food insecurity), whereas community-level data provides characteristics about the neighborhood where the patient lives (eg, median household income is below the poverty line, most residents have less than a high school education, community is a food desert). Many primary care clinics have developed their own systems for collecting some individual-level SDH data from patients, but few are using validated instruments to standardize data collection and integration into EHRs.42–44 Community-level SDH (or community vital signs) are readily available in national data sets, and it is technically possible to integrate these community-level SDH into a patient’s medical record using current geocoding technologies; however, community vital signs have not yet been widely imported into primary care data systems.25
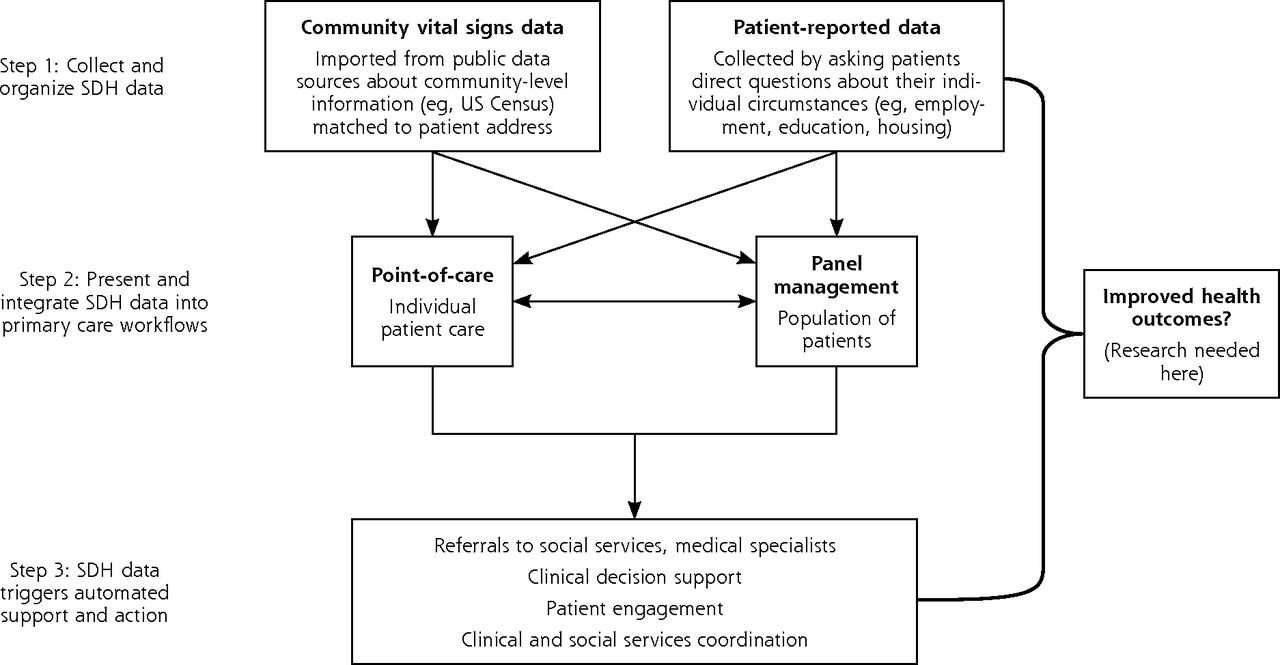
A framework for integrating social determinants of health (SDH) into primary care.
Once we make progress toward routine collection of SDH data, the second step is making the data available and useful in ways that enhance care (the right data, at the right time, in the right place). By systematizing the integration of SDH data into EHRs, these data become more readily and reliably available to the health care team, providing important contextual information and facilitating more relevant screenings, referrals to resources, and better tracking of processes and outcomes.35 For example, effective data integration could (1) inform clinical decision making (eg, indicate the urgency of screening, medications, or behavioral counseling; augment clinical risk scores, such as the Framingham cardiovascular disease risk score has done in the UK); (2) enable teams to tailor services, facilitate appropriate referrals, and coordinate care across community organizations; and (3) facilitate active panel management approaches that identify and prioritize patients for focused outreach (eg, community health worker visits, intensive care management).29,35,43,45 Standardizing the collection of SDH data and presenting this information at critical points in care delivery may lead to improved patient and population health outcomes. There is likely another important step needed to maximize the potential usefulness of integrating SDH into primary care, however. This third step involves the development of automated systems that harness SDH data to prompt action. For decades, primary care clinicians have sought to engage in activities to address SDH (eg, referrals to support services, engaging in community health activities); new technologies can greatly accelerate these efforts.35,43,44 Systems that automatically act upon SDH information to facilitate care (eg, clinical decision support tools, pop-up reminders to prompt special consideration or services, care management registries) could improve care delivery and coordination with minimal burden to health care clinicians.41 Studies suggest that clinicians routinely underestimate patients’ social needs46 and that standardized approaches can identify unmet needs more effectively than can informal screening or ad hoc interviews.47
RESEARCH MUST KEEP PACE WITH INTEGRATION EFFORTS
The time for integrating and acting upon SDH data in primary care is now. Yet, we know very little about how to ensure effective integration and action. Currently, SDH information is sporadically collected across primary care, and actions to address this information are based on anecdote and best guess approaches.35,39 What is known from studying EHR-based tools intended to support clinical decision making is that simply documenting SDH data in EHRs may not be enough to create meaningful change; a critical next step will be to identify evidence-based workflows for care teams to use the data purposefully in clinical care.35,40 The nation needs a bold, forward-thinking research agenda to study and produce the evidence for how SDH data can and should be incorporated into primary care. As we move forward with efforts to address SDH, we must simultaneously investigate which social determinants are most influential on health outcomes, how to present SDH data in the EHR to maximize its utility, where in clinic workflows and in what format the data should be made available, and how care teams can best use such data. There is also vital work to be done in answering the key question: Is the integration of SDH into primary care merely the emperor’s new clothes, or is it precision public health that directly leads to improvements in patient and population health?
Footnotes
Conflicts of interest: authors report none.
- Received for publication August 24, 2015.
- Revision received August 25, 2015.
- Accepted for publication August 25, 2015.
- © 2016 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Relationship Between Social Risks and Diabetes Metrics in a US Health System
- A Brief Tool to Screen Patients for Precarious Employment: A Validation Study
- Expert panel identified health-related social needs and methodological considerations for a polysocial risk score
- Patient-Reported Social Risks and Clinician Decision Making: Results of a Clinician Survey in Primary Care Community Health Centers
- Community Health Workers as Trust Builders and Healers: A Cohort Study in Primary Care
- Routinely asking patients about income in primary care: a mixed-methods study
- Resource Brokering: Efforts to Assist Patients With Housing, Transportation, and Economic Needs in Primary Care Settings
- Shared Language for Shared Work in Population Health
- The Role of Community-Based Organizations in Improving Chronic Care for Safety-Net Populations
- The Impact of Social and Clinical Complexity on Diabetes Control Measures
- Primary Care Is an Essential Ingredient to a Successful Population Health Improvement Strategy
- When and How Do We Need Permission to Help Patients Address Social Risk?
- Task Sharing Chronic Disease Self-Management Training With Lay Health Coaches to Reduce Health Disparities
- How French general practitioners adapt their care to patients with social difficulties?
- Patient perspectives on routinely being asked about their race and ethnicity: Qualitative study in primary care
- Adults with Housing Insecurity Have Worse Access to Primary and Preventive Care
- Primary Care Practices' Implementation of Patient-Team Partnership: Findings from EvidenceNOW Southwest
- Progress towards using community context with clinical data in primary care
- Core Principles to Improve Primary Care Quality Management
- Adoption of Social Determinants of Health EHR Tools by Community Health Centers
- Employment Interventions in Health Settings: A Systematic Review and Synthesis
- Advancing the Science of Implementation in Primary Health Care
- Clinician Experiences with Screening for Social Needs in Primary Care
- Unstable Housing and Diabetes-Related Emergency Department Visits and Hospitalization: A Nationally Representative Study of Safety-Net Clinic Patients
- Proactive Strategies to Address Health Equity and Disparities: Recommendations from a Bi-National Symposium
- Association of the Social Determinants of Health With Quality of Primary Care
- Revisiting Primary Care's Critical Role in Achieving Health Equity: Pisacano Scholars' Reflections from Starfield Summit II
- Using State Administrative Data to Identify Social Complexity Risk Factors for Children
- Framework for building primary care capacity to address the social determinants of health
- Mapping Neighborhood Health Geomarkers To Clinical Care Decisions To Promote Equity In Child Health
- Perspectives in Primary Care: Family Medicine in a Divided Nation
- Health Benefits and Cost-Effectiveness of Brief Clinician Tobacco Counseling for Youth and Adults
- Cohort study of early literacy and childbearing over the reproductive lifecourse
- Taking action on the social determinants of health in clinical practice: a framework for health professionals
- "A Paradox Persists When the Paradigm Is Wrong": Pisacano Scholars' Reflections from the Inaugural Starfield Summit
- In This Issue: Confronting Constraints on Individual Behavior & Outcomes
- Theory vs Practice: Should Primary Care Practice Take on Social Determinants of Health Now? No.