
Abstract
BACKGROUND Electronic health records (EHR) have become commonplace in medicine. A disconnect between developers and users while creating the interface often fails to create a product that captures clinical workflow and issues become apparent with implementation. Optimization allows collaboration of clinicians and informaticists after implementation, but documentation of success has only been at the institutional level.
METHODS A 4-month, department-wide EHR optimization was conducted with information technology (IT). Optimizations were developed from an intensive quality improvement process involving all levels of clinicians and clinical staff. The optimizations were then categorized as accommodations (department adjusted workflow to EHR), creations (IT developed new workflows within EHR), discoveries (department found workflows within EHR), and modifications (IT changed workflows within EHR). Departmental productivity, defined as number of visits, charges, and payments, was standardized to ratios prior to COVID-19 and evaluated by Taylor’s change point analysis. Significant improvements were defined as shifts (change points), trends (5 or more consecutive values above/below the mean), and values outside 95% CIs.
RESULTS The 124 optimizations were categorized as 43 accommodations, 13 creations, 54 discoveries, and 14 modifications. Productivity ratios of monthly charges (0.74 to 1.28) and payments (0.83 to 1.58) significantly improved with the optimization efforts. Monthly visit ratios increased (0.65 to 0.98) but did not change significantly.
CONCLUSION Departmental collaboration with organizational IT for EHR optimization focused on detailed analysis of how workflows can impact productivity. Discovery optimization predominance indicates many solutions to EHR usability problems were already in the system. A large proportion of accommodation optimizations reinforced the need for better developer-user collaboration before implementation.
INTRODUCTION
In 2009, $27 billion in incentives were generated for development and implementation of electronic health records (EHRs) by the Health Information Technology for Economic and Clinical Health Act.1-8 What followed was an 11-fold increase in EHR implementations over the next 6 years,9 by which time 96% of all non-federal acute care hospitals and 86% of office-based practices utilized EHRs.2,10-12 The impetus of these changes was to improve communication, standardization, quality, and safety throughout medical care.3,13-18 Unfortunately, there have also been multiple unintended consequences such as increased work burden,1,2,16,19-23 negative clinician emotions,1,21,22 attenuated work flow communication,1,10,13,15,21 burnout,1,2,11,16,19 and facilitated medical errors.14,21
The implementation of EHR technology may be the root cause of some of these issues. This begins with developers designing a product based upon an organizational strategic vision, which routinely desires regulation compliance, billing productivity, and organizational growth.1 End-users are then asked to evaluate and customize the EHR for purchase. The time required for in-depth analysis of an unfamiliar system is often more than busy clinicians can commit to preimplementation.20 This results in an poorly aligned interface that fails to meet the clinicians’ needs as the developers lack an understanding of the clinicians’ workflow and the clinicians fail to appreciate all of the nuanced digital amenities.3,18,20,24 Overall efficient usability (speed and accuracy of task completion) can be compromised with this approach. Compromised usability directly relates to problems in productivity, error rate, and satisfaction.20
The theory of affordances states the benefits created by a concept, object, or system exist but are not utilizable (afforded) until they are perceived.15 New technologies take time before their outputs meet or exceed their inputs (information technology [IT] productivity paradox).1,4 The lack of time afforded busy clinicians to explore the nuances of an new EHR leaves them with feelings of helplessness and hopelessness.25 Furthermore, the formative usability of the interface depends upon the developers’ understanding of the workflow complexities for a group of diverse individuals.20 This is better handled in an optimization process, as developers rarely conduct a deep dive into the granular aspects of daily patient care before, and users rarely become deeply involved in, implementation.3,14,18,20,24 Therefore, it was essential for the project’s aim of improving our EHR’s summative usability that sufficient time and resources were afforded to fully understand each component of all aspects of all daily workflows, maximize their efficiency, identify those responsible for them, and create standardized best practices for each workflow.
Family physicians, and departments that train them, require a user-friendly EHR interface. When implementation fails to yield an EHR with high usability, optimization is necessary. Optimization is the process of continually improving a standing EHR1,3,24 using data analysis through real-time feedback16 and a focus on efficiency of patient outcomes, workflow, and sustainability.1,17 The quality improvement process is identified as a method for conducting the optimization process.3 Because of this, our family medicine department created a department-wide, multidisciplinary improvement process, in partnership with the institution’s IT department, to optimize our EHR 9 months after its implementation. The current literature on EHR optimization best practices is limited, but predominately details overall institutional initiatives.1,11,17,19 Even smaller organizations have had difficulty adjusting to large, complicated EHR systems.3 Our aim is to demonstrate that an individual department can create measurable changes in productivity, as defined by charges, payments, and visits, to preimplementation levels through a quality improvement–driven EHR optimization process.
METHODS
The EHR optimization plan (Table 1, Figure 1) was conducted at a moderate-sized (24 residents and 40 faculty) family medicine department in a public academic health care center serving a mostly rural population. Initially, senior departmental leadership validated the project’s importance by understanding the need, empowering a project lead, providing time and resources, and communicating these to the faculty. Eight work groups were created, related to specific critical areas within the department’s daily workflow: care coordination, communication, front desk, medication, notes, nursing, orders/referrals, and revenue. Groups were facilitated by a faculty lead and were comprised of a multidisciplinary team of both senior-level and junior-level individuals: administrators (3), care coordinators (3), junior and senior faculty (21), IT (4), nurses (7), pharmacy (1), front desk staff (2), residents (8), and social worker (1). Each team had 1-hour monthly meetings over a 4-month period co-facilitated by project and work group leads. Workflow problems were identified, and each facet of each problem was analyzed for efficiency in a step-by-step manner to identify best practices (responsibility, appropriate orders, appropriate location) and create workflow policy. Ideas were collected from all individuals within the department between meetings. Newfound knowledge was disseminated piecemeal at the time of discovery and in consolidated virtual job-specific formats that allowed participants to view the presentation and experiment within the EHR simultaneously on a double-screen set-up. Following dissemination, clinicians and staff were encouraged to schedule one-on-one sessions with IT to create their own favorite order set collections and text templates.
Departmental EHR Optimization Process

Flow diagram of departmental EHR optimization process.
EHR = electronic health record; IT = information technology.
We considered project interventions if they had potential to be impactful on productivity. Productivity was defined by clinical work and measured by the metrics of number of visits, charges, and payments. Number of visits allowed assessment of the relative speed with which patients could be seen. Charges and payments reflected changes in visit complexity that the EHR allowed physicians to identify and document. These numbers were collected from corporate accounting. The initial intervention of this optimization was the project’s initiation in June 2021. After the 4 monthly meetings, formal dissemination of the EHR improvements occurred in October 2021. The final intervention was the individualized favorite order sets and templets in February 2022.
Optimizations within and related to the EHR were tracked and categorized (Table 2, 3) as either an accommodation (workflow adjustments made by the department outside of the EHR), creation (workflow added to the EHR by IT), discovery (workflow found by the department already inside the EHR), and modification (workflow changed within the EHR by IT). Category designation was assigned when more than 80% of author agreement occurred from independent ratings. Improvements failing to meet this consensus were assigned based on group discussion. Improvements spawned from multiple groups and were attributed to each.
Optimization Breakdown by Work Group and Improvement Type
Examples of Optimizations
Analysis
Monthly departmental measurements of productivity (number of departmental visits, charges, and payments) were obtained from verifiable institutional numbers. A baseline was created for analysis by the average of the 2 months before COVID-19 and all numbers were reported as a ratio of that. The statistical process control methodology was utilized to identify significant process variance. Significant results include 5 or more consecutive values above the mean (trend), shifts identified by Taylor’s change point analysis, and values outside the 95% CIs.26,27 Upper and lower 95% CIs were assigned through the bootstrapping method. This project was deemed exempt by the Marshall University Internal Review Board.
RESULTS
There were 124 identified optimizations divided into 4 categories: accommodations, discoveries, creations, and modifications (Table 2, 3).
Of those, 27 (22%) were in the IT dependent categories: 13 were creations (11%) and 14 were modifications (11%). For IT-driven changes, the work groups for care coordination, communication, orders/referrals, and revenue were nearly evenly split in contributions and exceeded the combined total of 22%. Front desk, medications, notes, and nursing had few contributions. Creations optimizations had the highest percentages of changes from work groups for care coordination (25%), communication (20%), and revenue (22%). Modifications optimizations were predominatly created by the ordering/referrals group (6 of the 14 modifications).
Departmental dependent categories accounted for 97 (78%) of the optimizations: 43 (35%) were accomodations and 54 (44%) were discoveries. Accommodations optimizations were predominantly from the front desk (70%) and nursing (71%) groups. Discoveries optimimizations were dominated by the notes work group (88%).
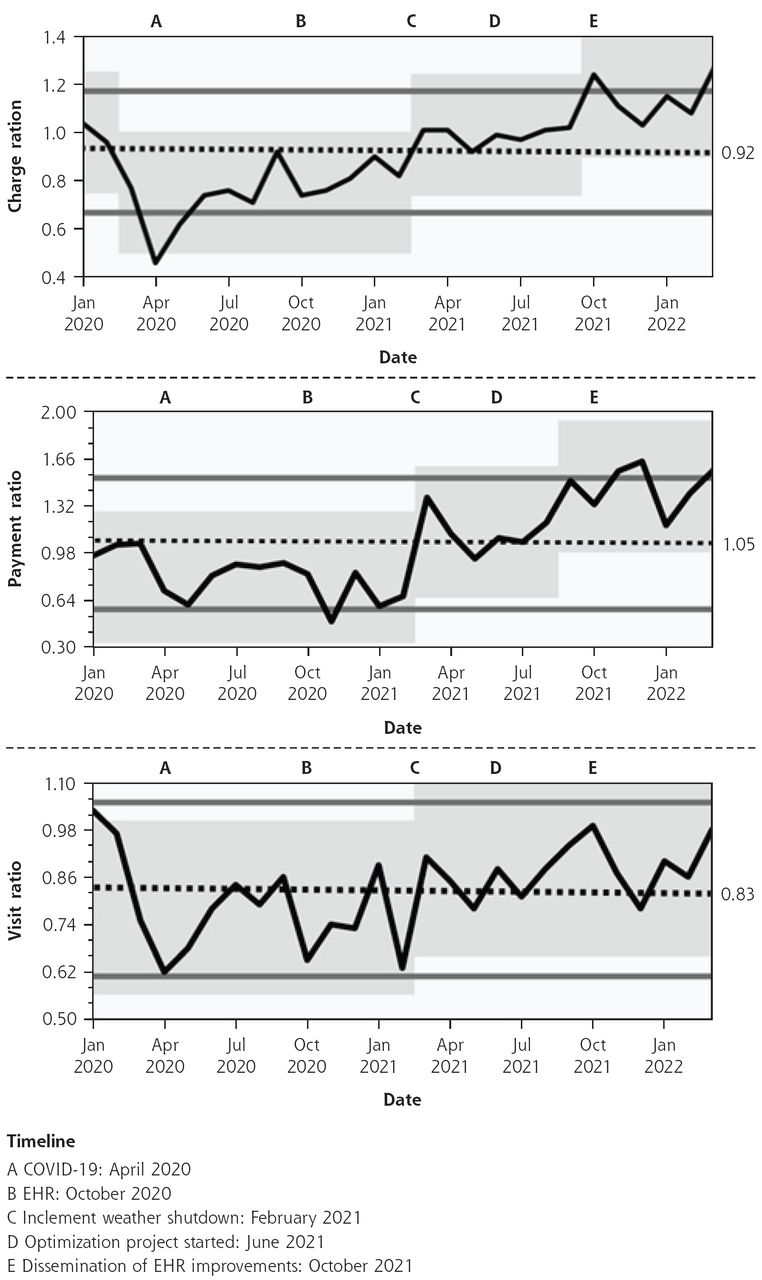
Special cause variation in departmental productivity (Figure 2), displayed as a ratio compared with production prior to COVID-19, was measured by overall trend, shifts in change point analysis, and values extending beyond the 95% CIs.26,27

Longitudinal assessment of charges, payments, and visits in and around the time of the digital optimization project.
EHR = electronic health record.
Note: Data represented as a ratio of the monthly rate compared with the average monthly level of function prior to COVID-19 with 95% CIs (solid lines) and mean level (dotted line). Shaded areas represent shifts in baseline by Taylor’s change point analysis.
Minimal change was observed for number of visits where a shift was only seen from February to March 2021 (0.63 to 0.91; 99% confidence). Still, gradual improvement was seen from the first full month of COVID-19 in April 2020 (0.62) until data collection ceased in March 2022 (0.98).
Charges plummeted in March 2020 (0.96 to 0.77; 94% confidence) creating a nadir outside the lower limit of normal in April 2020 (0.46). Change points were seen in March 2021 (0.82 to 1.01; 99% confidence) and October 2021 (1.02 to 1.24; 97% confidence). Significant values above the upper limit of normal were seen in the latter data of October 2021 (1.24) and March 2022 (1.28).
Payments had similar shifts in March 2021 (0.67 to 1.38; 100% confidence) and September 2021 (1.20 to 1.50; 95% confidence), as well as values above the 95% CI in 3 of the last 5 months (1.57, 1.64, and 1.58). Unlike in charges, the payment measurement in November 2020 (0.49) was below the 95% CI, which was 1 month following the EHR implementation date.
DISCUSSION
Ostensibly, the usability of an EHR is a function of how its interface allows users to care for their patients effectively, efficiently, and safely. It should be intuitive and provide necessary information in a timely manner. Usability of the EHR is directly related to productivity, error rate, and user fatigue metrics, but is perceived through user satisfaction which should not be the ultimate assessment.20 As a whole, EHRs were rated as unacceptable (9th percentile; mean 46; SD 21) on the System Usability Scale for Technology in a survey of 870 physicians (70% response rate).2 The wide variance is thought to be due to the many unique EHR systems.2 Poorly communicated strategic vision, unengaged clinicians, and insufficient resources for training result in an oft-missed opportunity to enhance an EHR’s productive usability before and during implementation.3,20,25
The aim of our optimization project was to enhance the usability of our existing EHR through an intentional and coordinated effort that incorporated ideas from every individual in the department. As this was a multidisciplinary departmental effort (Figure 1), it differs from previously described optimizations in the literature, which were conducted at the organizational level.1,11,17,19,28 By conducting this optimization on the departmental level, we were able to tailor changes to create a more homogenous workflow, specific to a single specialty, while also designing a format that could be replicated in other departments or institutions.
Productivity data must be examined through the context of specific events to evaluate the impact of an optimization process. Operational changes created to mitigate the clinical impact of the COVID-19 pandemic were devastating to departmental productivity.29 This was seen with a shift in charges between March 2020 and April 2020, and in a drop below the lower limit of normality in April 2020 for visits and charges. Six months later, as visits, charges, and payments were just beginning to rebound, the improved EHR implementation occurred. This further depressed visits and charges,20 while the normally delayed effect on payments was not seen until the significantly lower level the following month. A trend above the mean was seen from the beginning of the optimization efforts in June 2021 through the end of data collection in March 2022 for both charges (0.92) and payments (1.05). Benefits of the interventions were further affirmed with an upward shift in charges and visits when improvements were disseminated in October 2021, and in payments the following month. Finally, the cumulative effect of all interventions can be seen with 2 values above the 95% CI noted for charges and 3 seen for payments in the project’s last 6 months. Fewer significant findings occured for visits. This is likely due to a wellness intervention during the project that changed visit duration from 15 to 20 minutes. Any impact on visits was blunted by the reduction of 8 visits per clinician per day. This made the return to near pre-pandemic levels in March 2022 (0.98) noteworthy. Unexpectedly, there was a shift seen on all 3 productivity metrics between February 2021 and March 2021. This is likely due to the combination of February being a short month and impactful ice storms in the area that prevented clinic visits for a week, reducing the number of office days to 15, compared with the 23 in following month.
Further lessons can also be understood from the interventions themselves. The IT-remedied interventions (creation and modification) were surprisingly few in number (27), accounting for only 22% of all. This is consistent with current literature,11,25 but different from what the department anticipated prior to optimization, as members thought that most improvements would occur from IT adding or amending current EHR functions. Within the IT interventions, changes were predominately compiling department-specific order entry preference lists (ie, medications, laboratories, billing codes, and orders) based on the most utilized departmental options from the previous 9 months. This ameliorated the fundamental issue of clinicians having an overabundance of options, which resulted in orders being abandoned in electronic destinations outside of the workflow of their intended recipients. These optimizations could have been generated before implementation had there been better collaboration between designers and users.
Another lesson can be seen in the large proportion (44%) of discovery optimizations (44%), in which the answers were already in the EHR, but the users were unaware that the function existed. This disconnect, dominant in the notes work group (88%), aligns with the current literature that better education during implementation allows for better interface functioning.3,14,18,20,24 As this is a well-established problem but continually occurs, we ask, “How do we fix the disconnect that continues to allow EHR implementation to be suboptimal for clinician needs?”
Sadly, the second largest proportion of optimizations (35%) were accommodations by the department adjusting workflow issues outside of the EHR. This was felt most by the front desk (70%) and nursing (71%) work groups and occurred when a digital fix for EHR difficulties was deemed impossible. Accepting the limitations within the EHR and working around them did become more palatable to clinicians the more they saw beneficial changes occurring from their collaboration with IT. Here too was a missed opportunity where better pathways could have been built in the EHR’s design before implementation when the structure was potentially more malleable. The only potential remedy at this point would be with better user engagement in future upgrades.
The costs of the process included 4 hours of optimization meetings for the participants in each group. The project lead and work group leaders spent an additional 2 to 4 hours in coordination and documentation efforts. Dissemination required meetings for front desk staff (patient service representatives, 1 hour), nurses (2 hours), and clinicians (6 hours). Despite the widespread dissemination efforts, the department maintained some level of patient care at all times and at all sites. The return on investment, in addition to the improved productivity, was better engagement with IT. This translated into some leaders and early adopters becoming clinician advocates within the greater organizational digital structure. Working directly with clinicians identifying barriers in productivity and workflow challenged the IT staff to identify EHR solutions, allowing for creation of workflows for how to address similar issues from other departments and disperse education at an organizational level.
Attempts to mitigate data limitations included group classification of improvements and pulling productivity numbers from an external record. Utilizing multidisciplinary frontline staff prevented EHR improvements from being too clinician- or administrative-centric. Including IT personnel likely provided a more balanced picture of the process. This study’s single site does limit its external validity. However, creating a framework from disparate evidence-based recommendations that explores and identifies the workflow needs of an organization and optimizes the standing EHR resources should be widely applicable. There is an obvious observation bias, as just starting this effort sparked noticeable enthusiasm for the optimization process. We, however, claim that as a benefit derived from breaking the prior user melancholy that this framework promotes. The external factor of the COVID-19 pandemic did inhibit our productivity, but this only muted the impact of our interventions.
CONCLUSION
This work is the first to demonstrate that a highly successful EHR optimization can be conducted at the departmental level. A practical, detail-oriented, proactive approach can produce real-world gains in productivity. Lessons learned herein, specifically regarding collaboration with IT, can be extrapolated to not only improving the function of active EHRs but potentially creating novel EHRs with better clinician interfaces. Optimization is a constant process. Further collaboration is required to maintain and enhance already-realized benefits. We hope that this work can inspire and empower other departments to optimize their digital records.
Acknowledgments
The authors would like to acknowledge Michelle Peters for her work in formatting and image development.
Footnotes
Annals Early Access article
Conflicts of interest: authors report none.
- Received for publication April 8, 2023.
- Revision received November 7, 2023.
- Accepted for publication November 16, 2023.
- © 2024 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}