
Abstract
PURPOSE We sought to identify and compare studies reporting the prevalence of multimorbidity and to suggest methodologic aspects to be considered in the conduct of such studies.
METHODS We searched the literature for English- and French-language articles published between 1980 and September 2010 that described the prevalence of multimorbidity in the general population, in primary care, or both. We assessed quality of included studies with a modified version of the Strengthening the Reporting of Observational Studies in Epidemiology checklist. Results of individual prevalence studies were adjusted so that they could be compared graphically.
RESULTS The final sample included 21 articles: 8 described studies conducted in primary care, 12 in the general population, and 1 in both. All articles were of good quality. The largest differences in prevalence of multimorbidity were observed at age 75 in both primary care (with prevalence ranging from 3.5% to 98.5% across studies) and the general population (with prevalence ranging from 13.1% to 71.8% across studies). Apart from differences in geographic settings, we identified differences in recruitment method and sample size (primary care: 980–60,857 patients; general population: 1,099–316,928 individuals), data collection, and the operational definition of multimorbidity used, including the number of diagnoses considered (primary care: 5 to all; general population: 7 to all). This last aspect seemed to be the most important factor in estimating prevalence.
CONCLUSIONS Marked variation exists among studies of the prevalence of multimorbidity with respect to both methodology and findings. When undertaking such studies, investigators should carefully consider the specific diagnoses included and their number, as well as the operational definition of multimorbidity.
- prevalence
- multimorbidity
- comorbidity
- primary care
- general population
- family practice
- chronic disease
- practice-based research
INTRODUCTION
As a result of various factors, including aging of the population and advances in medical care and public health policy, a growing proportion of patients have multiple coexisting chronic diseases, also referred to as multimorbidity.1,2 Because of the negative consequences and high cost associated with multimorbidity, it has received growing interest in the primary care literature over the past few years and is now acknowledged by some as a research priority.3–7 At a time when several countries are undergoing major primary care reforms, multimorbidity appears to be a driver of change as it implies a shift in health services from the single-disease paradigm from which the majority of medical knowledge arises to a more holistic view of patients and a “generalist approach” to care.8
Unlike single chronic diseases or conditions for which strong epidemiologic data are available, however, results for multimorbidity vary widely among studies, making it difficult to determine whether differences among countries and locations and between the general and primary care populations are real or due to a wide variety of methodologic issues. Considering the importance of valid descriptive data, this area of research deserves greater attention.9 In this systematic review, we evaluate prevalence studies on multimorbidity and highlight the differences and possible explanations for variations among them. Our aim was to identify and compare studies reporting the prevalence of multimorbidity, and to suggest methodologic aspects to be considered in the conduct of such studies.
METHODS
Inclusion Criteria
We searched for articles meeting both of 2 inclusion criteria: they described the prevalence of multimorbidity or reported results that allowed its calculation, and they reported studies conducted in primary care, in the general population, or both.
Search Strategy and Article Selection
We conducted an electronic literature search of the Ovid MEDLINE and MANTIS databases for English- and French-language articles published between 1980 and September 2010. The strategy was run in both databases simultaneously, and duplicates were eliminated (as shown in Supplemental Appendix 1, available at http://www.annfammed.org/content/10/2/142/suppl/DC1). We used 4 Medical Subject Headings (MeSH): prevalence, chronic disease, primary health care, and family practice; we also used the key words multimorbidity and its lexical and nonlexical linguistic variation multi-morbidity, multiple diseases, prevalence study, general practice, and population. To broaden the scope of our research, we also applied the search strategy to the same databases using the MeSH comorbidity and its linguistic variation co-morbidity. We also examined reference lists for additional relevant articles.
One team member (J.A.) read the abstract to exclude articles that were not eligible. Two authors (J.A. and M-E.P.) independently appraised the full text of the retrieved papers. Articles meeting all inclusion criteria were retained for quality assessment and data extraction. Discrepancies between the 2 reviewers were resolved by team consensus.
Assessment of Study Quality
We assessed study quality with a modified version of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (available at http://www.strobe-statement.org/fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_cross-sectional.pdf).10,11 The checklist was modified to include items that should be considered in reports of cross-sectional studies. Each reviewer (J.A. and M-E.P.) independently determined a global quality score for each article, giving 1 point for each STROBE item the article addressed. To be retained in our review, articles had to have a quality score of at least 12 out of a possible 23.
Data Extraction and Calculations
We extracted all data related to multimorbidity prevalence or its calculation from the included articles. As multimorbidity is strongly associated with older ages, and there was no uniformity in the way age and sex were reported in the articles, we made the following age-related adjustments so that we could display all prevalence studies in a single graph for comparison (one for primary care and one for the general population).
-
If prevalence was reported for an age range, we calculated mean age between the lower and upper limits to represent the range in the graph.
-
If prevalence was reported for an age range with an upper limit only, we adjusted the age to approximately 10 years below the upper limit to represent the range. For example, if the age was either 25 years or younger, or younger than 25 years, we used an age of 15 years.
-
If prevalence was reported for an age range with a lower limit only, we adjusted the age to approximately 10 years above the lower limit to represent the range. For example, if the age was either 70 years or older, or older than 70 years, we used an age of 80 years.
-
If prevalence was reported for male and female individuals separately, we calculated the weighted mean value of both groups to represent the prevalence in the graph.
RESULTS
Articles Included in the Review
Our process for selecting articles is shown in Figure 1. The search strategies identified 27 references with the word multimorbidity and 2,173 with the word comorbidity, of which 1,942 remained after removing articles written in languages other than English or French and duplicates. After the abstracts were read for eligibility, 17 articles were retained to be read completely; 8 more were identified by reviewing reference lists. Of these 25 publications, 4 were excluded because they did not contain prevalence information or data allowing its calculation. The final sample used for data extraction and calculations was thus 21 articles: 8 containing prevalence information in primary care,1,2,12–17 12 in the general population,18–29 and 1 in both settings.30

Number of references identified at each stage of the systematic review.
Study quality was assessed in all but 2 publications that were not research articles, one a statistical report28 and the other a chartbook.29 Quality scores in the final sample of articles ranged from 15 to 23 out of 23 (as shown in Supplemental Appendix 2, available at http://www.annfammed.org/content/10/2/142/suppl/DC1); therefore, all articles were retained.
Primary Care Settings
The primary care articles reported prevalence in the Netherlands,1,2,15,30 the United Kingdom,14,16 Canada,13 Australia,12 and Greece.17 Table 1 shows characteristics of those reporting prevalence estimates of 2 or more coexisting chronic conditions. One article reported the prevalence based on 2 or more domains of the Cumulative Illness Rating Scale (CIRS) affected by chronic diseases.12 The CIRS makes it possible to classify any illness within 1 of the 14 organ system domains of the instrument, simplifying coding down to 14 possible domains. Britt and colleagues12 have proposed that multimorbidity be defined as involvement of 2 or more organ domains by chronic diseases.
Studies Reporting Prevalence of Multimorbidity in Primary Care Settings
The studies were heterogeneous in terms of recruitment methods, sample size, data collection, and operational definition of multimorbidity or comorbidity. Three studies sampled patients from those consulting their family physician,12,13,17 whereas the others included all patients from the selected practices. The number of participants in each study varied tremendously, from 980 to 60,857. In 2 studies, data were collected using chart review13,14; in the others, data were collected from a registry or an electronic health record. With regard to the operational definition of multimorbidity and comorbidity, the main source of variation was the number of diseases considered in the count (5, 8, 68, 83, 185, or all possible chronic conditions) regardless of the data collection approach used. The definition of a chronic condition varied among studies, and the importance or severity of the disease was usually not specified. All publications defined multimorbidity as having 2 or more chronic diseases (or 2 or more affected CIRS domains) and reported results accordingly, but the majority also reported other cutoffs such as 3 or more, or 4 or more.2,12,13,15–17,30 One article reported the number of patients with chronic diseases in more than 2 domains of the CIRS without weighting for severity.12
Figure 2 summarizes the prevalence estimates reported by these studies based on a count of 2 or more chronic diseases (or CIRS domains) according to age and shows a wide variation in the results, the only constant being the increasing prevalence with age. The largest difference in prevalence (Δ = 95.0%) was observed at age 75 years, with prevalence ranging from 3.5% in a study reporting on 5 chronic diseases15 to 98.5% in another reporting on all chronic diseases.13 Among studies that included patients of all ages, there was an S-shaped curve for the association between age and prevalence: prevalence was roughly 20% or lower before the age of 40 years, then increased dramatically, and finally plateaued around the age of 70 years at 75%.
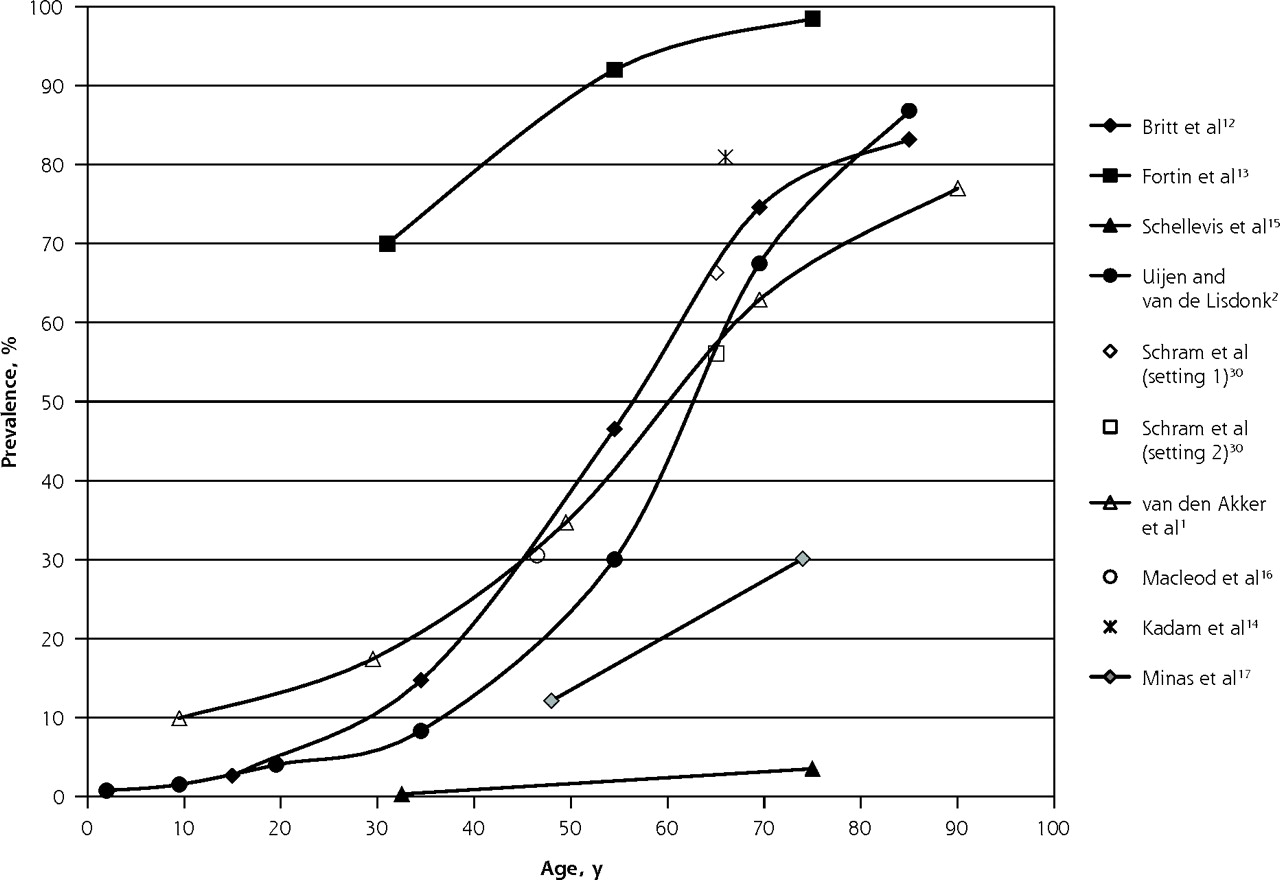
Prevalence of multimorbidity (defined as ≥2 diseases) reported in primary care settings.
Note: Data reported in the studies were adjusted to fit into the graph, as described in the Methods section.
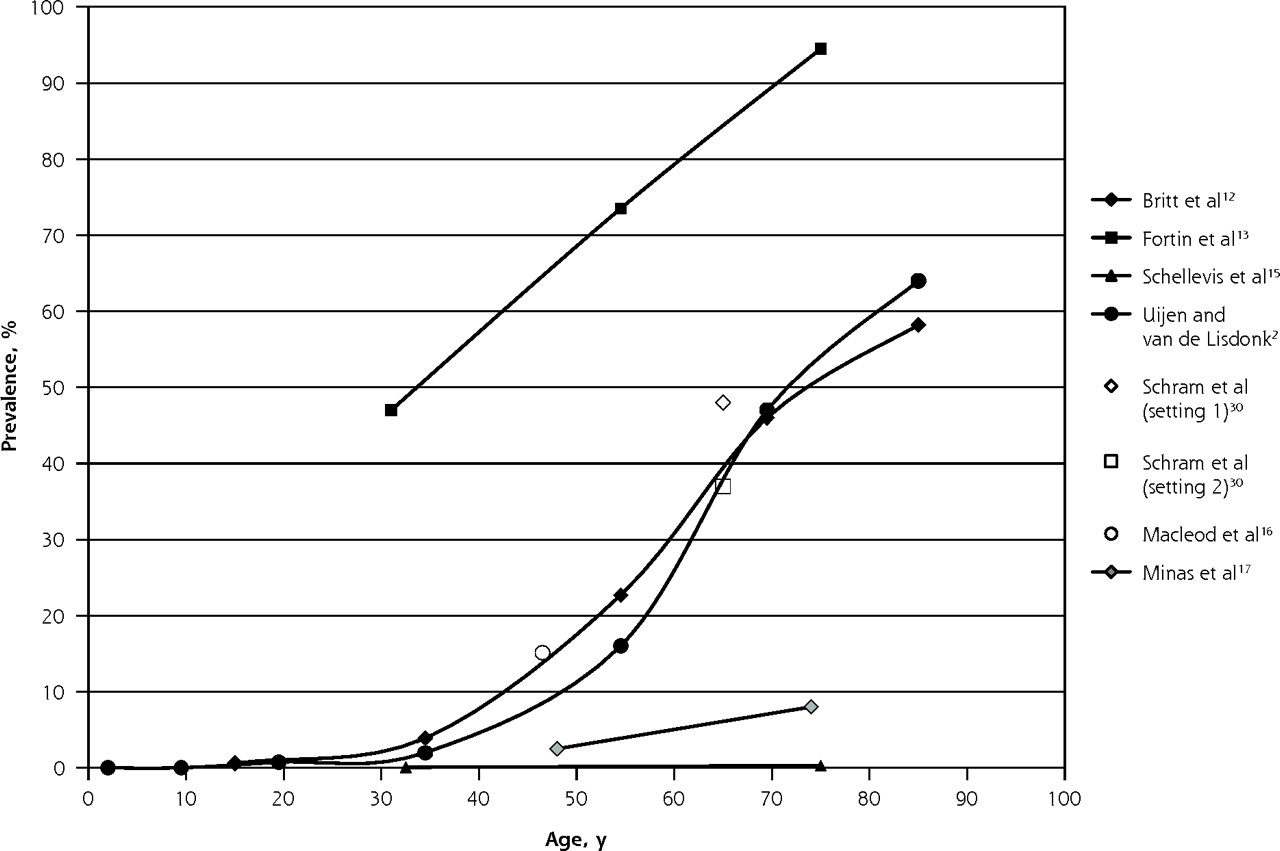
Figure 3 shows the results for studies reporting results with a cutoff of 3 or more chronic diseases used to define multimorbidity. The S-shaped curves are still evident, although the curves are less pronounced and more linear, with an overall lower prevalence as expected. The 2 studies looking at broad age ranges reported increasing numbers of chronic conditions with advancing age.1,13
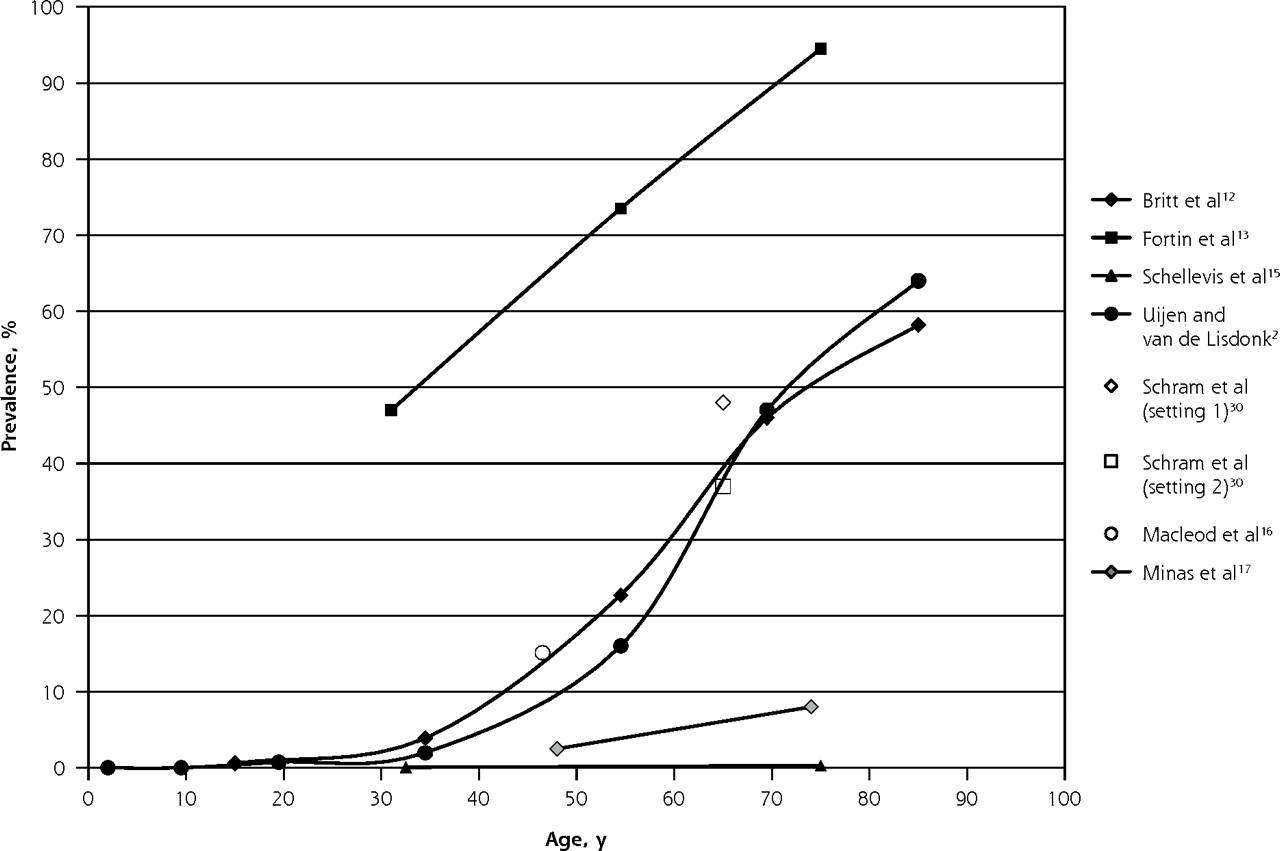
Prevalence of multimorbidity (defined as ≥3 diseases) reported in primary care settings.
Note: Data reported in the studies were adjusted to fit into the graph, as described in the Methods section.
General Population
Studies of the general population reported either national or local prevalence of multimorbidity in the United States,22,24,27,29 Canada,25,28 Israel,26 Ireland,23 Germany,21 Sweden,19 the Netherlands,30 and Spain.18 One article gathered data from sites in Finland, Italy, and the Netherlands.20 Table 2 shows the characteristics of articles reporting prevalence estimates of 2 or more coexisting chronic conditions in the general population.
Studies Reporting Prevalence of Multimorbidity in the General Population
As for the primary care studies, these studies varied considerably in their recruitment methods, sample sizes, data collection methods, and operational definitions of multimorbidity. Participants consisted of national random samples,18,22,24–29 cohorts in particular geographic locations,19–21,30 or individuals identified from national pharmacy claims databases.23 The sample size again varied widely, from 1,099 to 316,928 individuals. Most studies used a questionnaire18,21,22,24–29; other methods were clinical assessment,19,20,30 medical history obtained from a health professional,30 and use of a pharmacy database to identify conditions.23
The number of reported conditions varied from 7 to any number, with variation in the criteria used to define them. All studies considered a count of 2 diseases or more as multimorbidity. Many studies included chronic conditions without regard for their severity, masking considerable variation in disease burden for patients.
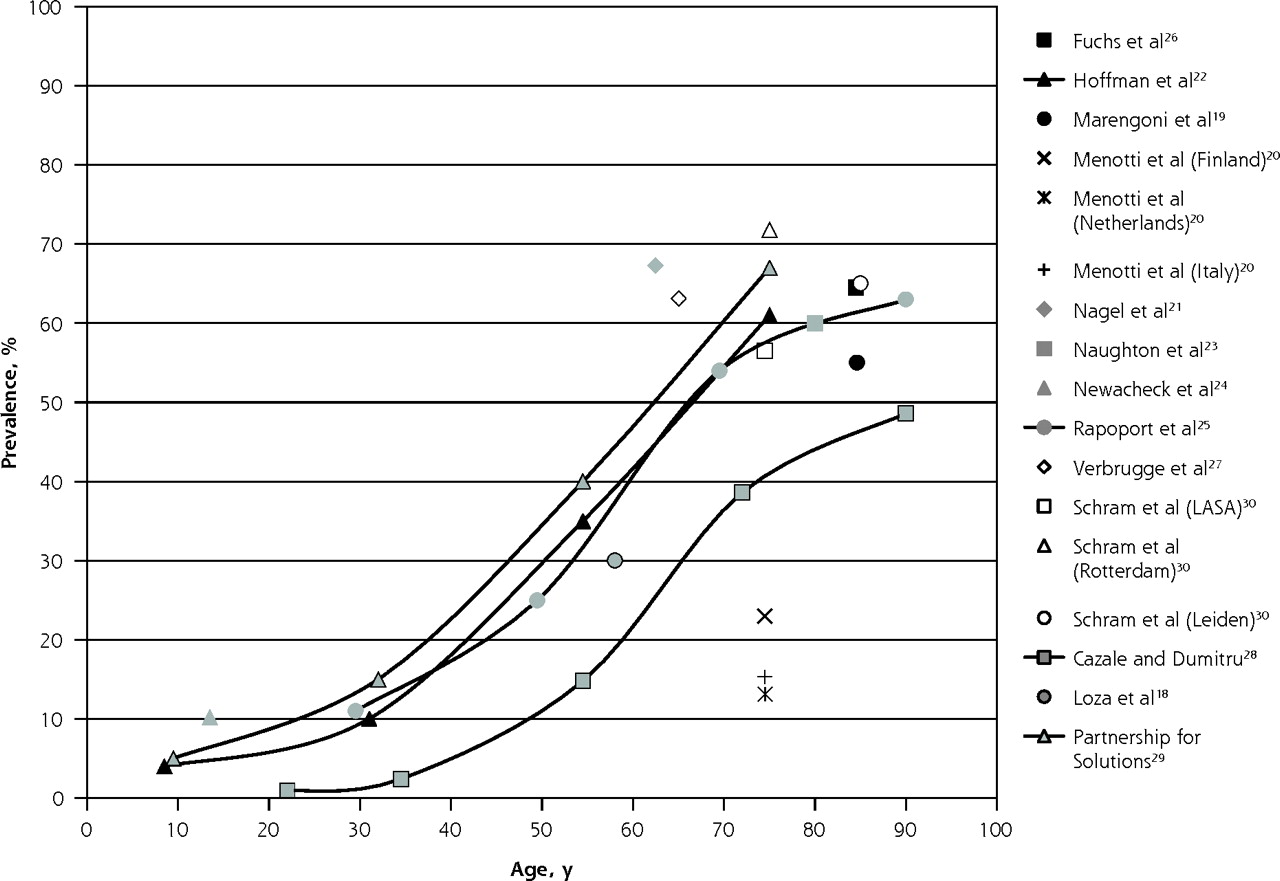
Figure 4 depicts the prevalence estimates reported in these general population studies according to age. Again, the highest variation in prevalence (Δ = 58.7%) was observed at age 75, with values ranging from 13.1%20 to 71.8%30 across studies; of note, both studies reported data from the Netherlands. The studies assessing individuals across broad age ranges showed S-shaped curves for prevalence by age, similar to those found in the primary care settings.
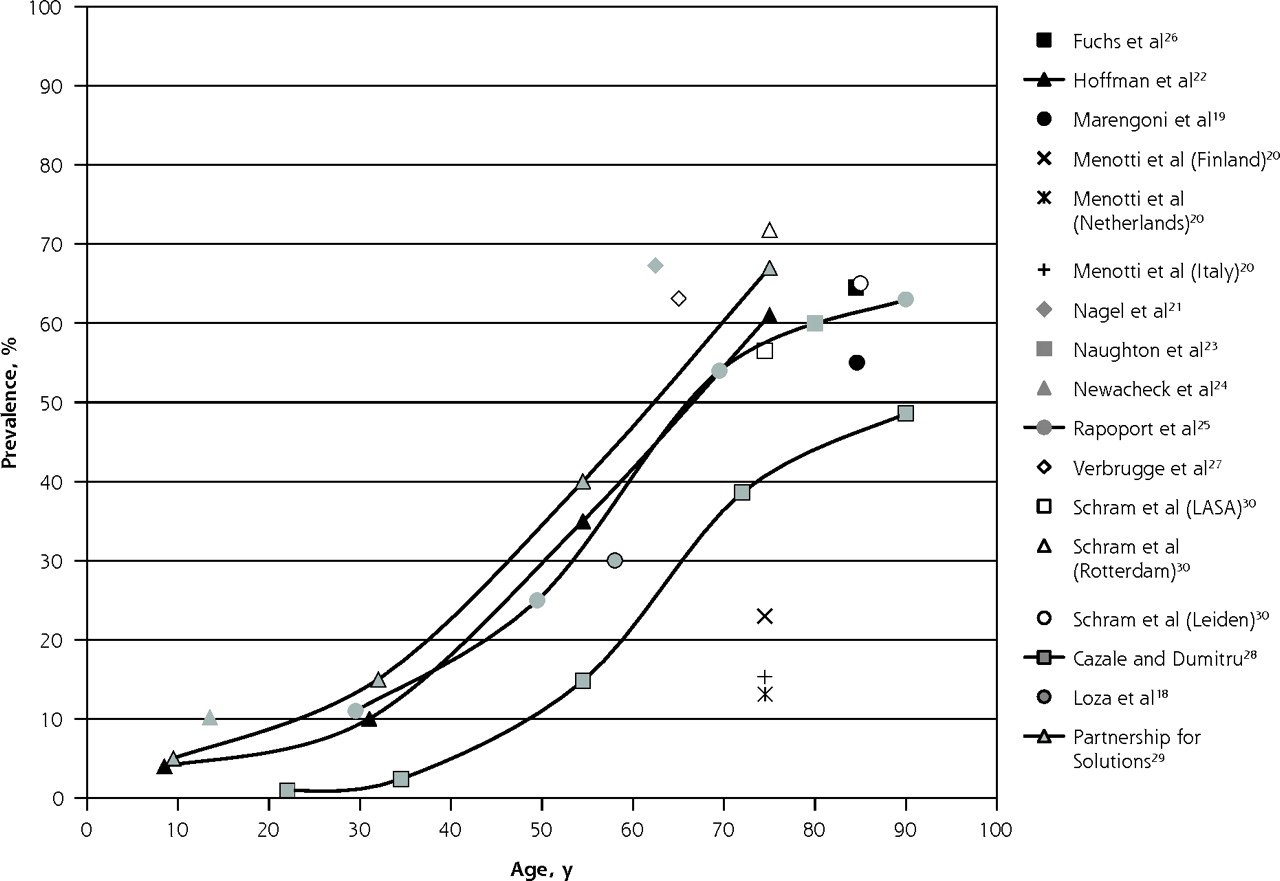
Prevalence of multimorbidity (≥2 diseases) in the general population.
LASA = Longitudinal Aging Study Amsterdam.
Note: Data reported in the studies were adjusted to fit into the graph, as described in the Methods section
DISCUSSION
Our systematic review shows that prevalence estimates of multimorbidity vary widely among studies. The largest difference was observed at the age of 75 years both in primary care and in the general population (Δ across studies = 95% and 59%, respectively). Differences of this magnitude are unlikely to reflect real differences between populations and more likely to be due to biases in methods. In addition to their differing geographic settings, the studies differed in recruitment method and sample size, data collection, and operational definition of multimorbidity, including the number of conditions and the conditions selected. All of these factors may affect prevalence estimates.
Impact of Methodology
The majority of studies conducted in primary care used existing patient databases. These cohorts have the advantage of including a very large number of diverse patients.2,15,16,30 Their prevalence estimates are probably a good representation of the actual prevalence at the primary care level in their respective locations, provided that a random sample of practices is included; however, the reliability of these estimates can be affected by factors such as the completeness of records and how data are codified.
In contrast, studies wherein patients are recruited during a visit with the physician may overrepresent frequent attenders, who have more complex medical problems and would increase the apparent prevalence of multimorbidity observed in the practice. This phenomenon may explain why 3 of the 4 primary care studies using this recruitment method also had the highest multimorbidity prevalence.12–14 In addition, this kind of recruitment is likely to produce smaller sample sizes, reducing the precision of estimates.
Differing methods may also partly explain the differences we observed in prevalence estimates. This influence can be inferred from the results of one study in the general population involving individuals of the same age-group among whom conditions were assessed using a variety of sources.30 The prevalence estimate based on self-reports and general practitioner reports was lower than that obtained when data were collected from an extensive physical examination (56.5% vs 71.8%). One study in primary care extracted data from the combined input of general practitioners (using their knowledge of patients), patient self-reports, and medical records.12 This approach should provide more reliable estimates than those based on only a single source of information.
One study estimated the prevalence in the general population based on a pharmacy database.23 This method works better for chronic diseases treated with drugs that are specific to the disease and are taken continuously; however, its main drawback is the lack of definitive diagnostic information.
Prevalence estimates seemed to be greatly influenced by the operational definition of multimorbidity, which has 2 components: the list of diagnoses considered and the cutoff used to define presence of the diagnosis. As an example, the study in our review with the fewest diagnoses considered (5 diagnoses) reported the lowest prevalence values in primary care (0.3% at age 32.5 years and 3.5% at age 75 years) despite its very large size (23,534 patients).15 Other studies from the same country (the Netherlands) that considered more diagnoses reported higher prevalence estimates.1,2,30 This pattern is consistent with a previous report that found large differences in prevalence estimates according to the number of chronic diseases considered.9
Similarly, Figure 4 includes 2 studies of the general population of Canada, using comparable methods. The study of Rapoport et al,25 with 22 diseases taken into consideration, reported a higher prevalence than the study of Cazale and Dumitru,28 with just 7 diseases.
Studies done in both primary care and the general population showed an S-shaped curve for prevalence by age, with low estimates before the age of 40 years and then a steep increase in prevalence followed by a plateau at about the age of 70 years (Figures 2 and 4). This plateau may be due to a balance between new cases and mortality at older ages, or to the current definition of multimorbidity as 2 or more chronic conditions. The plateau at older ages is not as flat when the definition of 3 or more chronic conditions is used (Figure 3).
Suggestions for Study Conduct
Considering all of the various aspects of prevalence studies on multimorbidity highlighted in this systematic review, we suggest some methodologic issues to be considered in the conduct of such studies.
Sampling Method
At the primary care level, there are basically 2 approaches for sampling. One approach is to extract data from existing databases, which usually provides information on the whole practice or a large number of patients, and reflects the general situation prevailing in the setting. Data could be extracted for randomly selected patients or for all patients. The second approach is to include patients seen during clinical sessions within a time period. This method may oversample complex patients with several diseases or frequent attendees; however, it provides insight into the physician’s daily work. Use of one sampling frame or the other is dictated by the research question and the resources available. In studies involving the general population, random samples, either at a national level or in particular geographic locations, are appropriate.
Data Collection
The method most often used for data collection in prevalence studies at the practice level was to check patients’ medical history in medical charts or computerized databases. This method has the advantage of being based on written evidence but assumes that the records are complete, which may not always be the case.
Another approach is to obtain data from the combined input of physicians, patient self-reports, and medical records. Intuitively, the use of multiple sources should provide more reliable estimates than a single source and is preferred when feasible. Studies conducted in the general population predominantly used questionnaires. As this method is based on self-report, it may present the disadvantage of assigning equal weight to both major and minor health conditions. The use of this method may be justified when the research question specifically addresses perceived burden or when very large samples are studied, when no other data are available as in many health surveys. In some studies in the general population, data were obtained from more than 1 source (self-report, medical history from general practitioners, clinical assessment). Again, a multisource method is preferable to a single-source method.
Operational Definition
The list of conditions assessed seems to be the most critical issue in studying prevalence estimates. Our review suggests that considering 4 to 7 diagnoses would lead to an underestimation of the prevalence of multimorbidity. In studies that considered 12 or more diagnoses, we did not observe much variation. We therefore suggest using a list of at least 12 chronic diseases. Further research is needed to select which specific diseases, but a list of the 12 most prevalent chronic diseases with a high impact or burden in a given population would be a good compromise. We cannot provide a precise list from this review.
Tabulation of the number of domains of the CIRS affected by chronic diseases is another method of measuring multimorbidity prevalence comparable to the simple count of diseases.12 This approach deserves further attention as it may simplify coding and data collection.
Concerning the cutoff in number of medical conditions, we found that studies generally reported main results based on a count of 2 or more conditions, but some also reported the number of patients with higher counts. We suggest systematic use of at least 2 operational definitions of multimorbidity, namely, both 2 or more diagnoses (or CIRS domains) and 3 or more diagnoses (or CIRS domains). The latter definition results in a lower prevalence of multimorbidity and likely better identifies patients with higher needs, and thus may be more meaningful for clinicians than a count of 2 or more, which is less discriminating. In addition, the difference in the S-shape pattern between Figures 2 and 3 may further support this new operational definition. Additional research is needed to test this definition.
Reporting Results
When reporting prevalence estimates by age-group, as there is no standard for age-groups, investigators should be sure to provide enough information to allow good assessment of their cohorts in terms of age, especially when they use open-ended age-groups (eg, aged ≥65 years). Information about the age structure (or at least the mean and SD) would facilitate graphical display and comparison. Reporting results both for each sex and for the sexes combined would also facilitate comparison.
Study Limitations
A limitation of any systematic review is the potential omission of relevant articles. Although we tried to use exhaustive inclusion criteria, it is possible that we did not identify all publications on the subject. Our search strategy was based on MeSH and key words assigned by authors, and we may have missed publications that were not indexed under these terms, although we tried to identify further articles through reference lists. Our search strategy had the advantage of using 2 large databases, however, enabling an exhaustive literature review.
Conclusion
In conclusion, in this review of 21 studies, we observed marked differences across studies in the estimated prevalence of multimorbidity. These differences appeared to be largely due to variations in study methodology, especially how multimorbidity was defined. Investigators designing future studies to assess the prevalence of multimorbidity should consider the number of diagnoses to be assessed (with ≥12 frequent diagnoses of chronic diseases appearing ideal) and should attempt to report results for differing definitions of multimorbidity (both ≥3 diseases and the classic ≥2 diseases). Use of a more uniform methodology should permit more accurate estimation of the prevalence of multimorbidity and facilitate comparisons across settings and populations.
Acknowledgments
We would like to acknowledge Elizabeth Bayliss, MD, MSPH, for her contribution in reading and commenting on the manuscript. We also thank Susie Bernier and Tarek Bouhali for their editorial assistance.
Footnotes
-
Conflicts of interest: authors report none.
-
Funding support: Dr Fortin is supported by the Canadian Institutes of Health Research (CIHR) and partners (CIHR Applied Health Services and Policy Research Chair on Chronic Diseases in Primary Care/Canadian Institutes of Health Research-Institute of Health Services and Policy Research, Canadian Health Services Research Foundation, and Centre de santé et de services sociaux de Chicoutimi). Dr Stewart is funded by the Dr Brian W. Gilbert Canada Research Chair.
-
Disclaimer: None of the funding agencies had any role in the collection, analysis, and interpretation of the data, or in the preparation, review, or approval of the manuscript.
- Received for publication February 11, 2011.
- Revision received June 23, 2011.
- Accepted for publication August 5, 2011.
- © 2012 Annals of Family Medicine, Inc.
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence and predictors of sub-optimal laboratory monitoring of selected higher risk medicines in Irish general practice: a 5-year retrospective cohort study of community-dwelling older adults
- Operationalizing multimorbidity in relation to mortality and physical function: findings from a prospective longitudinal cohort study
- Investigating associations between physical multimorbidity clusters and subsequent depression: cluster and survival analysis of UK Biobank data
- Assessing the impact of Canadian primary care research and researchers: Citation analysis
- Impact of multimorbidity and complex multimorbidity on healthcare utilisation in older Australian adults aged 45 years or more: a large population-based cross-sectional data linkage study
- Systematic review and meta-analysis of disease clustering in multimorbidity: a study protocol
- Multimorbidity in African ancestry populations: a scoping review
- Association between Johns Hopkins Adjusted Clinical Groups risk scores and self-reported outcome measures: an observational study among individuals with complex or long-term conditions in Norway
- Multimorbidity and blood pressure control: a cross-sectional analysis among 67,385 adults with hypertension in Canada
- What can death records tell us about multimorbidity?
- How do People with Multimorbidity Prioritise Healthcare when Faced with Financial Constraints? A Choice Experiment
- Age, sex, and socioeconomic differences in multimorbidity measured in four ways: UK primary care cross-sectional analysis
- Association between patient complexity and healthcare costs in primary care on a Japanese island: a cross-sectional study
- Association between maternal multimorbidity and preterm birth, low birth weight and small for gestational age: a prospective birth cohort study from the Japan Environment and Childrens Study
- Booster vaccination with inactivated whole-virus or mRNA vaccines and COVID-19-related deaths among people with multimorbidity: a cohort study
- Topic modelling with ICD10-informed priors identifies novel genetic loci associated with multimorbidities in UK Biobank
- Trends in prevalence and incidence of registered dementia and trends in multimorbidity among patients with dementia in general practice in Flanders, Belgium, 2000-2021: a registry-based, retrospective, longitudinal cohort study
- Prevalence of multimorbidity combinations and their association with medical costs and poor health: a population-based study of U.S. adults
- Early-onset burdensome multimorbidity: an exploratory analysis of sentinel conditions, condition accrual sequence and duration of three long-term conditions using the 1970 British Cohort Study
- Community prevalence and dyad disease pattern of multimorbidity in China and India: a systematic review
- What is the impact of multimorbidity on out-of-pocket healthcare expenditure among community-dwelling older adults in Ireland? A cross-sectional study
- Study protocol for an epidemiological study 'Multimorbidity - identifying the most burdensome patterns, risk factors and potentials to reduce future burden (MOLTO) based on the Finnish health examination surveys and the ongoing register-based follow-up
- Variation in the estimated prevalence of multimorbidity: systematic review and meta-analysis of 193 international studies
- Optimizing Therapy to Prevent Avoidable Hospital Admissions in Multimorbid Older Adults (OPERAM): cluster randomised controlled trial
- Multimorbidity patterns of chronic conditions and geriatric syndromes in older patients from the MoPIM multicentre cohort study
- Prevalence and factors associated with multimorbidity among older adults in Malaysia: a population-based cross-sectional study
- Magnitude, pattern and correlates of multimorbidity among patients attending chronic outpatient medical care in Bahir Dar, northwest Ethiopia: the application of latent class analysis model
- Multimorbidity in South Africa: a systematic review of prevalence studies
- Prevalence of chronic conditions and multimorbidity in Estonia: a population-based cross-sectional study
- Comparison of FORTA, PRISCUS and EU(7)-PIM lists on identifying potentially inappropriate medication and its impact on cognitive function in multimorbid elderly German people in primary care: a multicentre observational study
- Multimorbidity of chronic non-communicable diseases: burden, care provision and outcomes over time among patients attending chronic outpatient medical care in Bahir Dar, Ethiopia--a mixed methods study protocol
- Clustering of comorbidities
- What is the impact of multimorbidity on the risk of hospitalisation in older adults? A systematic review study protocol
- Unravelling the mechanisms driving multimorbidity in COPD to develop holistic approaches to patient-centred care
- Patterns of Multimorbidity
- Systematic review on the instruments used for measuring the association of the level of multimorbidity and clinically important outcomes
- Impact of neighbourhood walkability on the onset of multimorbidity: a cohort study
- Patient-centred innovation for multimorbidity care: a mixed-methods, randomised trial and qualitative study of the patients experience
- Mise en {oelig}uvre de soins integres centres sur le patient pour des problemes chroniques multiples: Referentiel eclaire par des donnees probantes
- Implementing patient-centred integrated care for multiple chronic conditions: Evidence-informed framework
- Scaling Up Patient-Centered Interdisciplinary Care for Multimorbidity: A Pragmatic Mixed-Methods Randomized Controlled Trial
- Medical costs and out-of-pocket expenditures associated with multimorbidity in China: quantile regression analysis
- Trends in prevalence of chronic disease and multimorbidity in Ontario, Canada
- Prevalence of multimorbidity in South Africa: a systematic review protocol
- Comparing the prevalence of multimorbidity using different operational definitions in primary care in Singapore based on a cross-sectional study using retrospective, large administrative data
- Health-related quality of life in patients with non-communicable disease: study protocol of a cross-sectional survey
- Prevalence of multimorbidity with frailty and associations with socioeconomic position in an adult population: findings from the cross-sectional HUNT Study in Norway
- Socioeconomic inequalities in the prevalence of complex multimorbidity in a Norwegian population: findings from the cross-sectional HUNT Study
- Prevalence of secondary care multimorbidity in mid-life and its association with premature mortality in a large longitudinal cohort study
- Making the case for the study of symptoms in family practice
- Measuring multimorbidity beyond counting diseases: systematic review of community and population studies and guide to index choice
- Development and validation of the Cambridge Multimorbidity Score
- Multimorbidity patterns in chronic older patients, potentially inappropriate prescribing and adverse drug reactions: protocol of the multicentre prospective cohort study MoPIM
- Journey to multimorbidity: longitudinal analysis exploring cardiovascular risk factors and sociodemographic determinants in an urban setting
- Multimorbidity of chronic non-communicable diseases and its models of care in low- and middle-income countries: a scoping review protocol
- Multiple chronic conditions at a major urban health system: a retrospective cross-sectional analysis of frequencies, costs and comorbidity patterns
- Prevalence and patterns of multimorbidity among the elderly in China: a cross-sectional study using national survey data
- 'Multimorbidity: an acceptable term for patients or time for a rebrand?
- Chronic disease prevention and management programs in primary care: Realist synthesis of 6 programs in Quebec
- Rationale and design of OPtimising thERapy to prevent Avoidable hospital admissions in Multimorbid older people (OPERAM): a cluster randomised controlled trial
- Family practitioners' top medical priorities when managing patients with multimorbidity: a cross-sectional study
- Sex-specific intergenerational trends in morbidity burden and multimorbidity status in Hong Kong community: an age-period-cohort analysis of repeated population surveys
- Multimorbidity, eHealth and implications for equity: a cross-sectional survey of patient perspectives on eHealth
- Impact of educational attainment on the association between social class at birth and multimorbidity in middle age in the Aberdeen Children of the 1950s cohort study
- Predicting poorer health outcomes in older community-dwelling patients with multimorbidity: prospective cohort study assessing the accuracy of different multimorbidity definitions
- Shared vision for primary care delivery and research in Canada and the United States: Highlights from the cross-border symposium
- Prevalence and patterns of multimorbidity in Amazon Region of Brazil and associated determinants: a cross-sectional study
- Snapshot of the primary care waiting room: Informing practice redesign to align with the Patients Medical Home model
- Epidemiology of multimorbidity in New Zealand: a cross-sectional study using national-level hospital and pharmaceutical data
- Multimorbidity in Older Adults With Cardiovascular Disease
- Comparative analysis of methods for identifying multimorbidity patterns: a study of 'real-world data
- Prevalence of multimorbidity in general practice: a cross-sectional study within the Swiss Sentinel Surveillance System (Sentinella)
- Effectiveness of a complex intervention on Prioritising Multimedication in Multimorbidity (PRIMUM) in primary care: results of a pragmatic cluster randomised controlled trial
- The multimorbidity cluster analysis tool: identifying combinations and permutations of multiple chronic diseases using a record-level computational analysis
- Courage, relationships, and applicability: Big research from small places
- Courage, relations, et applicabilite: Recherche denvergure emanant de petites localites
- Multimorbidity and patterns of chronic conditions in a primary care population in Switzerland: a cross-sectional study
- Contextual and individual inequalities of multimorbidity in Brazilian adults: a cross-sectional national-based study
- Patient-Centred Innovations for Persons with Multimorbidity: funded evaluation protocol
- Prevalence, impact and cost of multimorbidity in a cohort of people with chronic pain in Ireland: a study protocol
- Does 'existential unease predict adult multimorbidity? Analytical cohort study on embodiment based on the Norwegian HUNT population
- Multimorbidity prevalence and pattern in Indonesian adults: an exploratory study using national survey data
- Multimorbidity in primary care: protocol of a national cross-sectional study in Switzerland
- Prevalence and outcomes of multimorbidity in South Asia: a systematic review
- Prevalence of multimorbidity in the adult population attending primary care in Portugal: a cross-sectional study
- Prevalence, Correlates, and Outcomes of Multimorbidity Among Patients Attending Primary Care in Odisha, India
- Why do patients with multimorbidity in England report worse experiences in primary care? Evidence from the General Practice Patient Survey
- Multimorbidity and weight loss in obese primary care patients: longitudinal study based on electronic healthcare records
- Perspectives in Primary Care: Implementing Patient-Centered Care Coordination for Individuals with Multiple Chronic Medical Conditions
- Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice