
Article Figures & Data
Figures
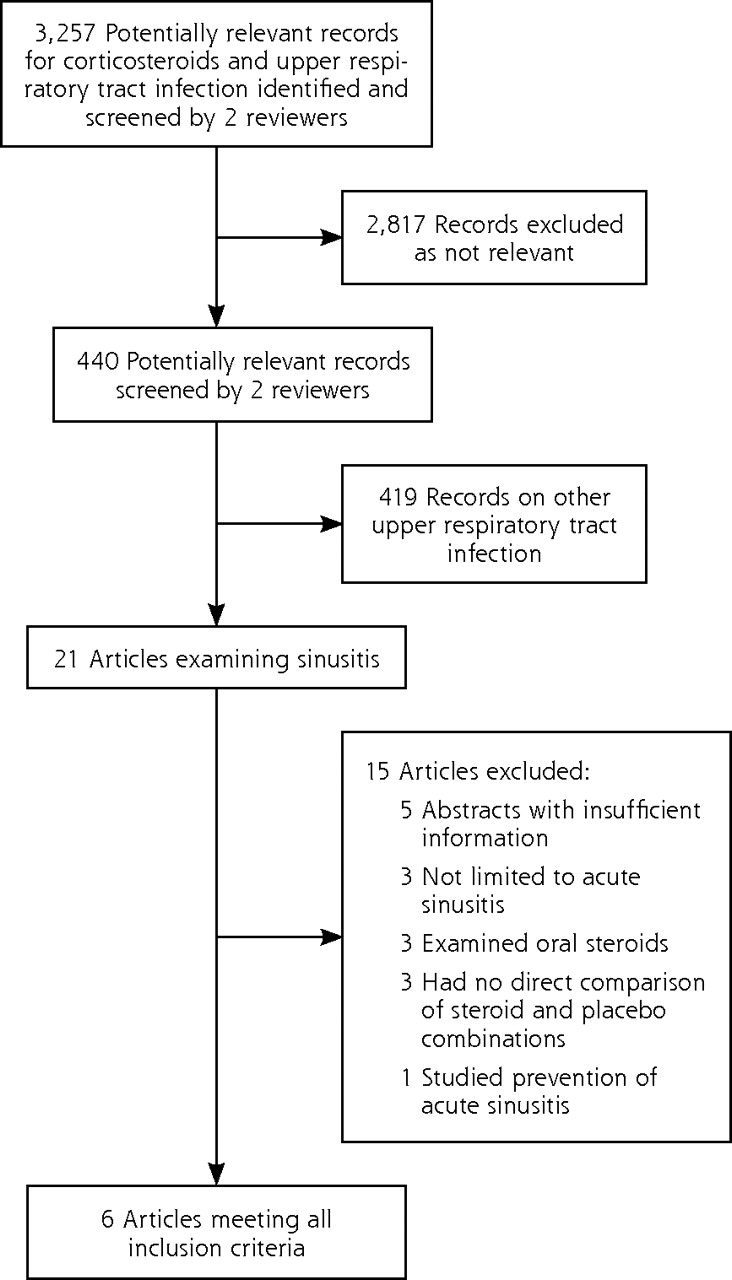
- Figure 1
Flow diagram of search results.
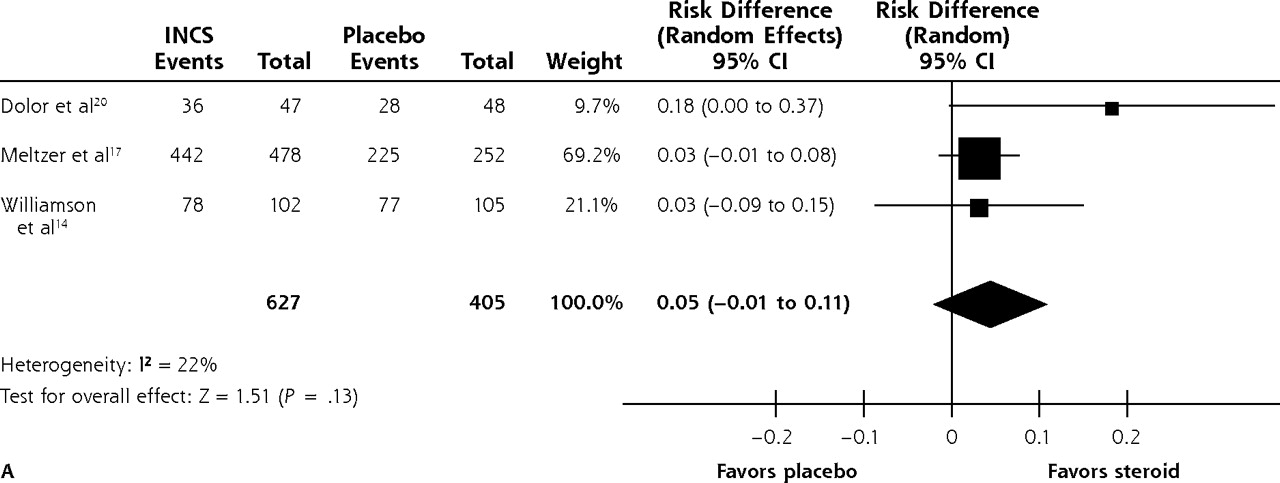
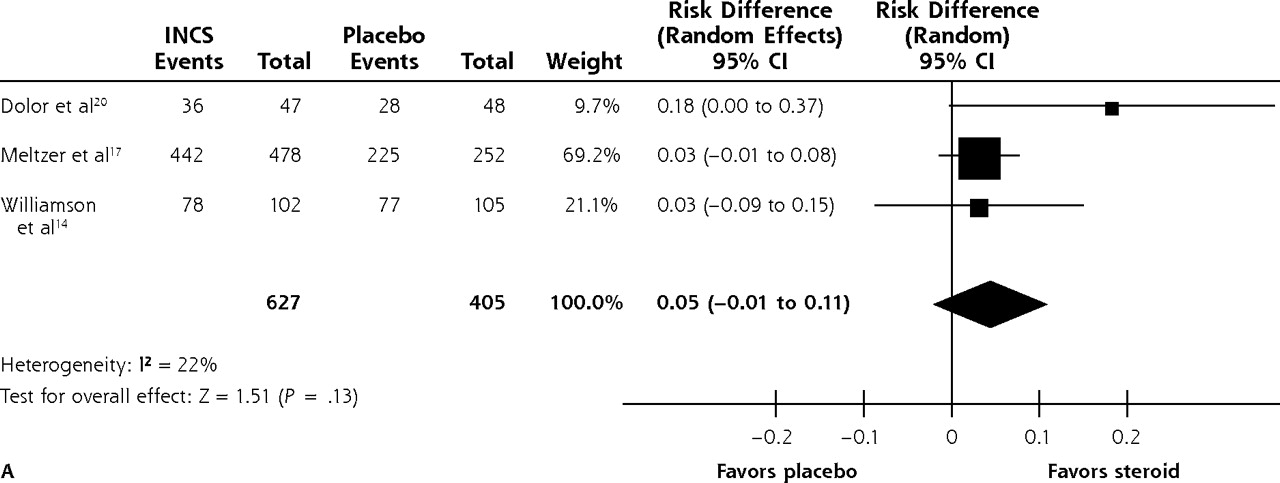
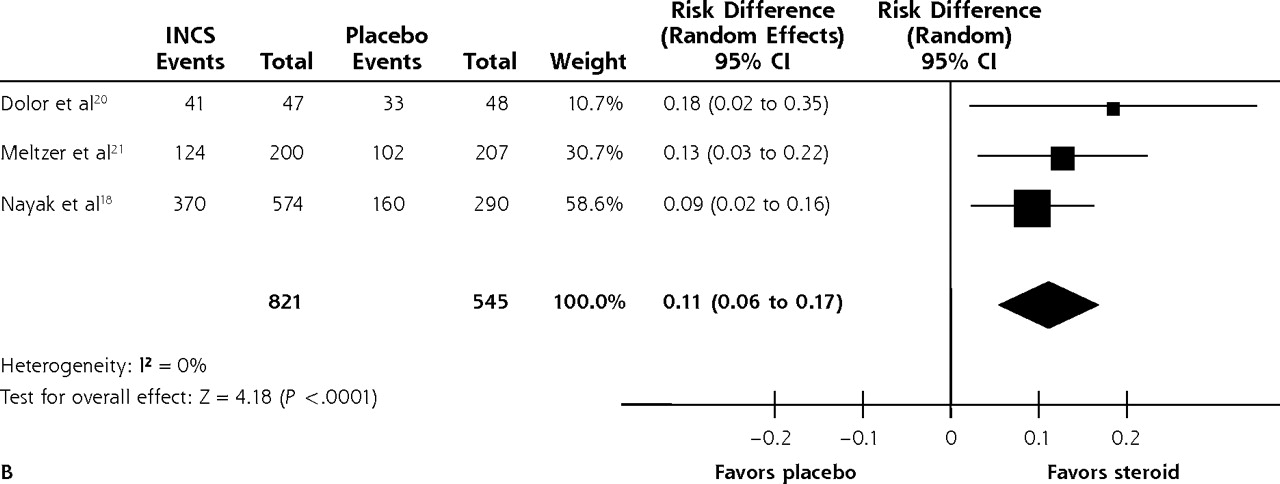
- Figure 2
Effect of intranasal steroids on resolution of symptoms of acute sinusitis at (A) 14 to 15 days and (B) 21 days.
INCS=intranasal steroid.
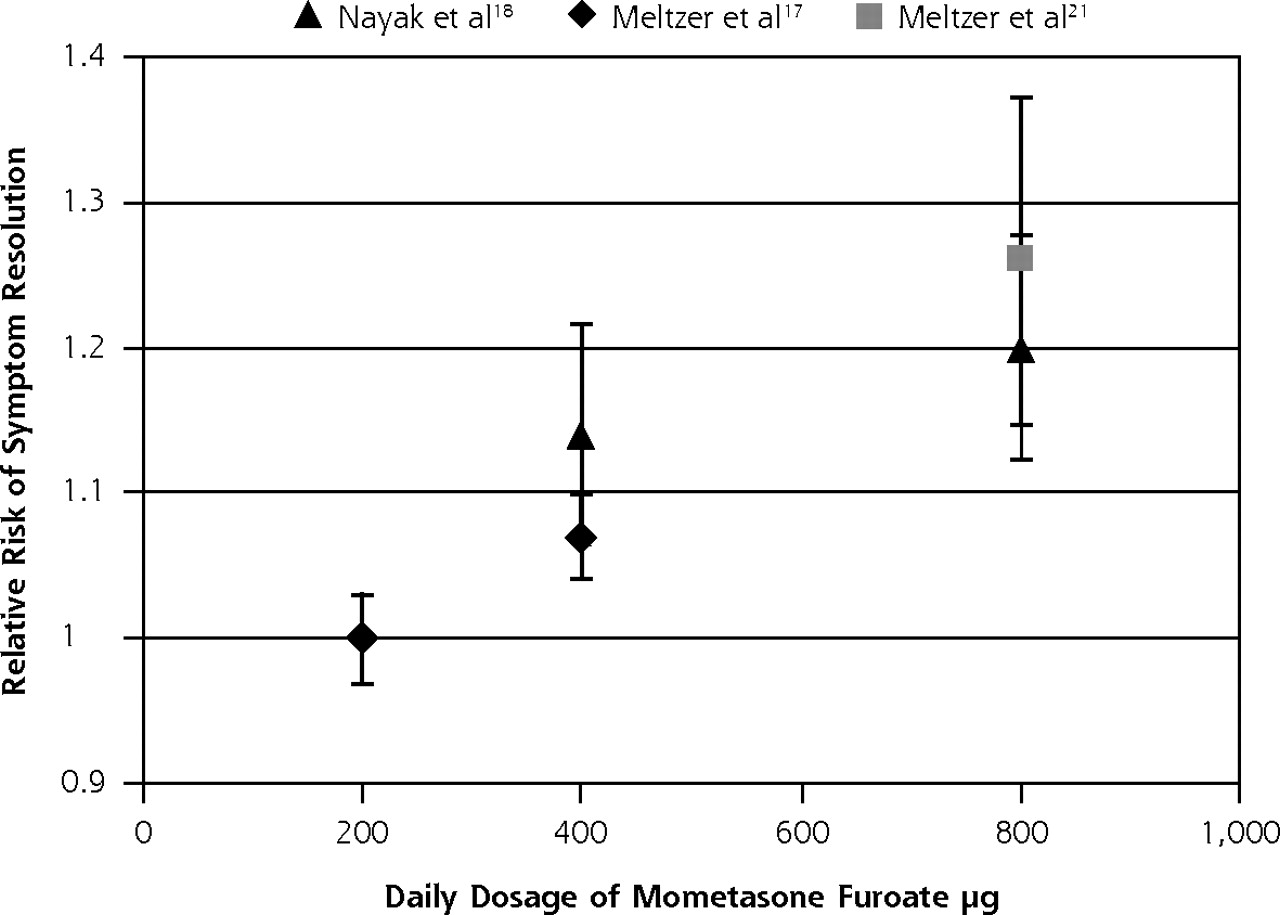
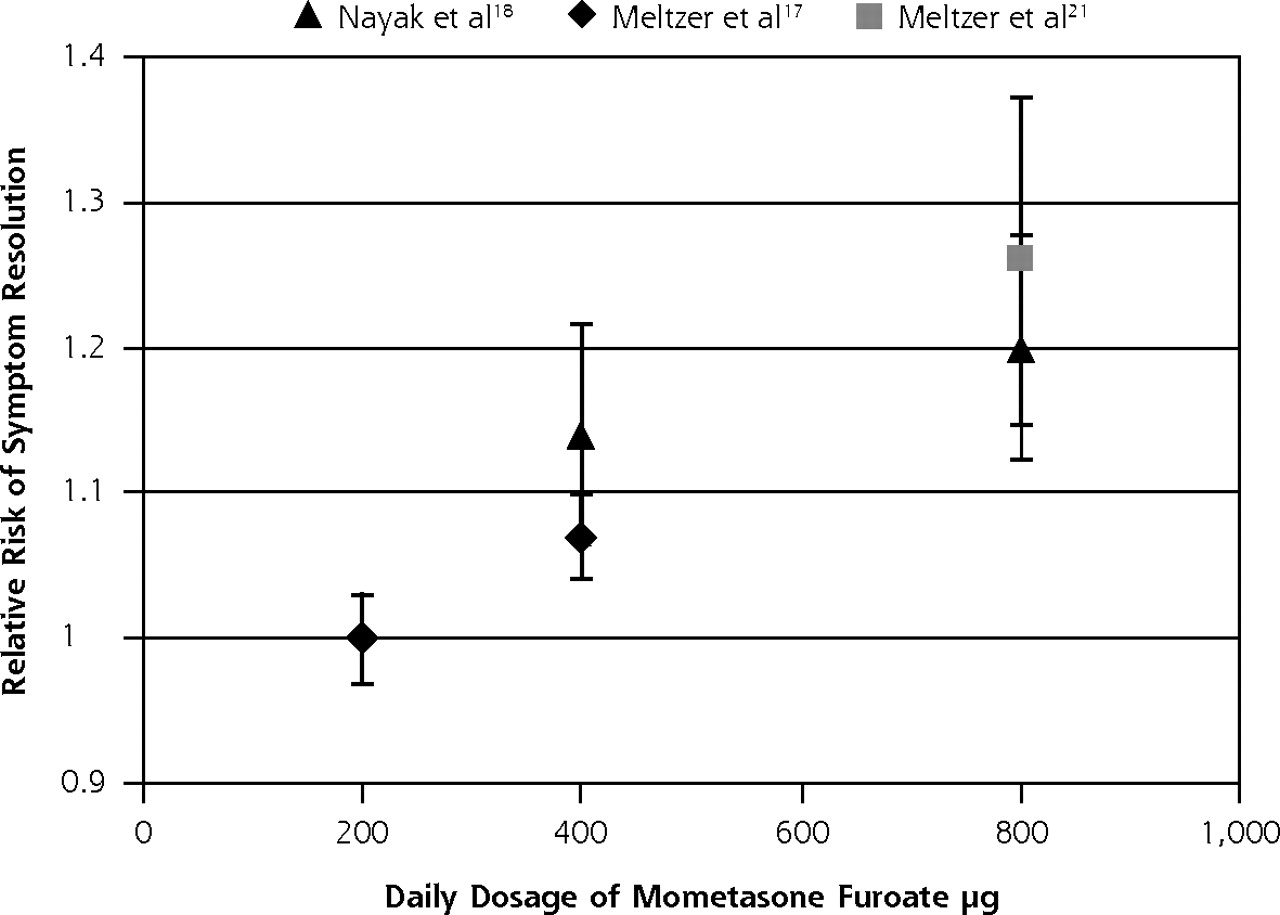
- Figure 3
Dose-response relationship of mometasone furoate and likelihood of symptom resolution.

Tables
Study (Year and Location) Age Range (Mean), y No. Analyzed Criteria for Sinusitis; Duration of Symptoms at Entry Treatment Other Medications Used Analgesia Outcomes and Definition of Symptom Resolution Intervention Control Interventiona Control Williamson et al14 (2007; United Kingdom, general practice) ≥16 (42.5) 102a 105b 2 of following: predominantly unilateral purulent nasal discharge and local pain, bilateral purulent nasal discharge, pus on inspection
Median duration of symptoms 7 days (IQR 10)400 μg budesonide once daily for 10 days Placebo spray Amoxicillin 500 mg 3 times a day for 7 days or placebo, factorial design used Not restricted, not reported Symptom scores assessed on 7-point scales
Time to resolution of symptoms
Percent with complete resolution of symptoms up to day 14
Resolution = patient reporting 0 or 1 on 7-point scale for 11 individual symptom scoresMeltzer et al17 (2005; 14 countries, medical centers) ≥12 (35.3) 478 252 Symptoms score ≥5/15 (scores of 0 = none to 3 = severe for facial pain, nasal congestion, headache, rhinorrhea, and postnasal drip)
Clinical signs/symptoms for >7 days but <28 days2 arms:c,d
MFNS 200 μg twice daily or
MFNS 200 μg once in the morning with placebo spray in the evening
Each given for 15 daysPlacebo spray Separate study arm received amoxicillin Prohibited Major symptom score = sum of individual symptom scores over days 2-15 of treatment
Time to onset of MSS being statistically different from placebo
Global response to treatment at day 15
Adverse events
Recurrence
Resolution = absence of failure of treatmentNayak et al18 (2002; United States, 61 treatment centers) ≥12 (39.1) 642 325 Coronal CT evidence of sinusitis
Total symptom score of ≥6/18 (scores of 0 = none to 3 = severe for facial pain, nasal congestion, headache, rhinorrhea, cough, and postnasal drip)
No information on duration given2 arms:c
MFNS 200 μg twice daily or
MFNS 400 μg twice daily
Each given for 21 daysPlacebo spray Amoxicillin–clavulanate potassium 875 mg twice daily for 21 days Not specifically commented on; not recorded Change from baseline in total symptom score
CT appearance of sinuses at 21 days
Percent of patients with resolution of symptoms
Adverse events
Resolution = patient reporting complete or marked relief of symptomsDolor et al20 (2001; United States, 12 primary care and 10 otorhinolaryngology clinics) ≥18 47 48 History of recurrent sinusitis
Clinical criteria: 2/5 of headache; facial pain and pressure; nasal congestion; purulent nasal discharge; and olfactory disturbance; and Water radiographic or endoscopic evidence of sinusitis
No information on duration given400 μg fluticasone propionate once daily for 21 days Placebo spray Cefuroxime axetil 250 mg twice daily for 10 days
2 puffs of xylometazoline hydrochloride in each nostril 10 min before the study nasal spray for the first 3 daysAllowed, unregulated Overall symptom score
Percent of patients with resolution of symptoms
Work attendance
Work performance
Quality of life (SNOT-20 score)
Adverse events
Recurrences
Additional attendances
Resolution = patient report of symptoms much improved or resolvedMeltzer et al21 (2000; United States, 29 medical centers, outpatient) ≥12 (40.4) 200 207 History of sinusitis episodes separated by symptom-free periods
Symptom score >6/18 (scores of 0 = none to 3 = severe on facial pain, nasal congestion, headache, rhinorrhea, cough, and postnasal drip) and coronal CT evidence of sinusitis
Mean duration of symptoms 13.5 daysMFNS 400 μg twice daily for 21 days Placebo spray Co-amoxiclav 875 mg twice daily for 21 days Paracetamol only; unregulated, unrecorded Symptom scores assessed on 6-point scale (individual symptoms and total scores)
Percent with complete resolution of symptoms at 21 days
CT scoring of sinusitis (10-point scale)
Adverse events
Resolution = patient reporting complete or marked relief of symptomsBarlan et al19 (1997; Turkey, pediatric outpatient clinic) ≤15 (6.95) 43 46 Clinical criteria: 2/3 of purulent nasal discharge, purulent pharyngeal drainage, and cough, or 1/3 of the above plus 2 of facial or tooth pain, edema, earache, sore throat, wheeze, headache, fever, and foul breath
No information on duration given100 μg budesonide twice daily for 21 days Propellant- only spray Amoxicillin–clavulanate potassium 40 mg/kg daily for 21 days Not reported Symptoms scores: median score of cough and nasal discharge for first, second, and third weeks
Relapse
Resolution (no overall measure reported)-
CT = computed tomography; IQR = interquartile range; MFNS = mometasone furoate nasal spray; MSS = mean symptom score; SNOT-20 = 20-item Sino-Nasal Outcome Test.24
-
↵a Total dose both nostrils.
-
↵b Factorial design means that each group included patients receiving both active and placebo antibiotics.
-
↵c Results of the 2 arms were combined for the overall analysis.
-
↵d A third arm evaluated amoxicillin 500 mg 3 times a day; therefore, these patients also received placebo capsules as a control for amoxicillin.
-
Study (Year) Allocation Concealment Randomization Comparability of Groups at Baseline Blindinga Provision of Care Apart From the Intervention Percentage Participation Williamson et al14 (2007) Adequate Random number table, block randomization Comparable Double blind Equal 86 Meltzer et al17 (2005) Adequate Computer-generated randomization stratified by duration of symptoms at presentation Comparable Double blind Equal 90 Nayak et al18 (2002) Adequate: matching placebo used Randomized, method not reported Comparable Double blind Equal 89 Dolor et al20 (2001) Adequate Permuted block randomization scheme stratified by site Comparable Double blind Equal 94 Meltzer et al21 (2000) Adequate: matching placebo used Randomized, method not reported Comparable Double blind Equal 100 Barlan et al19 (1997) Adequate Randomized, method not reported Comparable Double blind Equal 59 -
↵a Williamson et al was the only study to specifically describe the method of double blinding.
-
Supplemental Appendix
Supplemental Appendix. Mean Individual Symptom Scores Reported for Study and Dosage Arm
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 2 pages, 238 KB
The Article in Brief
Gail Hayward, and colleagues
Background Acute sinusitis is often treated with antibiotics, although there is little evidence for their benefit. This analysis of existing research examines the effects of intranasal corticosteroids on acute sinusitis symptoms.
What This Study Found After 14 to 21 days of intranasal corticosteroid use, patients show a small increase in the resolution or improvement of symptoms; the most consistently significant benefits are relief of face pain and congestion. The effect is most marked when patients are given longer durations of treatment (21 days) and higher doses of medication.
Implications
- The authors call for additional research comparing intranasal corticosteroids with placebo and without antibiotics to clarify the time-course of clinical benefit and the impact on work and quality of life.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Oral prednisolone for acute lower respiratory tract infection in clinically unrecognised asthma: an exploratory analysis of the Oral Steroids for Acute Cough (OSAC) randomised controlled trial
- Overuse of diagnostic tools and medications in acute rhinosinusitis in Spain: a population-based study (the PROSINUS study)
- A guide to the management of acute rhinosinusitis in primary care management strategy based on best evidence and recent European guidelines
- In This Issue: From Communities of Solution to Joy
- Intranasal Steroids for Acute Sinusitis?