
Article Figures & Data
Figures
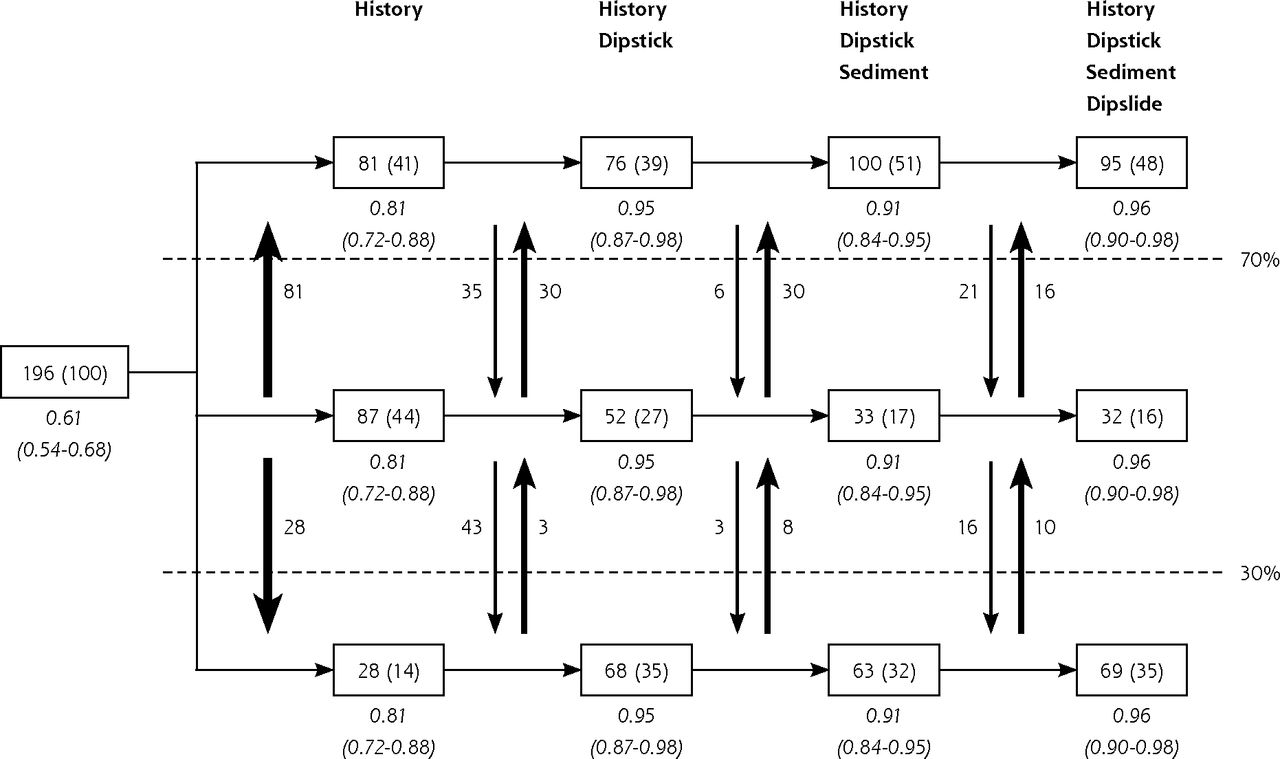
- Figure 1
Discrimination by subsequent tests when performed for all patients.
UTI=urinary tract infection.
Notes: In the boxes, patient numbers in each predicted risk category (with corresponding percentage in brackets) are shown after application of each subsequent diagnostic model to all 196 patients. The predicted risk categories used are <30%, 30%–70% and >70%. The vertical arrows display the numbers of patients that switch between categories after performing a test. The observed risks (and their 95% CIs) are shown in italics.
The figure is best read from left to right: 196 patients (100%) were included and the prevalence of UTI was 61%. Based on the results from the history questions only, 28 patients (14%) had a predicted risk of <30% and 81 patients (41%) had a predicted risk of >70%. When both history and a urine dipstick were performed, 68 patients (35%) had a predicted risk of <30% and 76 patients (39%) had a predicted risk of >70%. Additional performance of a sediment and dipslide resulted in removal from the intermediate category of 20 more patients (11%), mainly those who were correctly classified into the highest risk category after history only, but were incorrectly reclassified into the intermediate risk category after a negative nitrite test result on a urine dipstick. All observed risks were close to the predicted risks (good calibration).
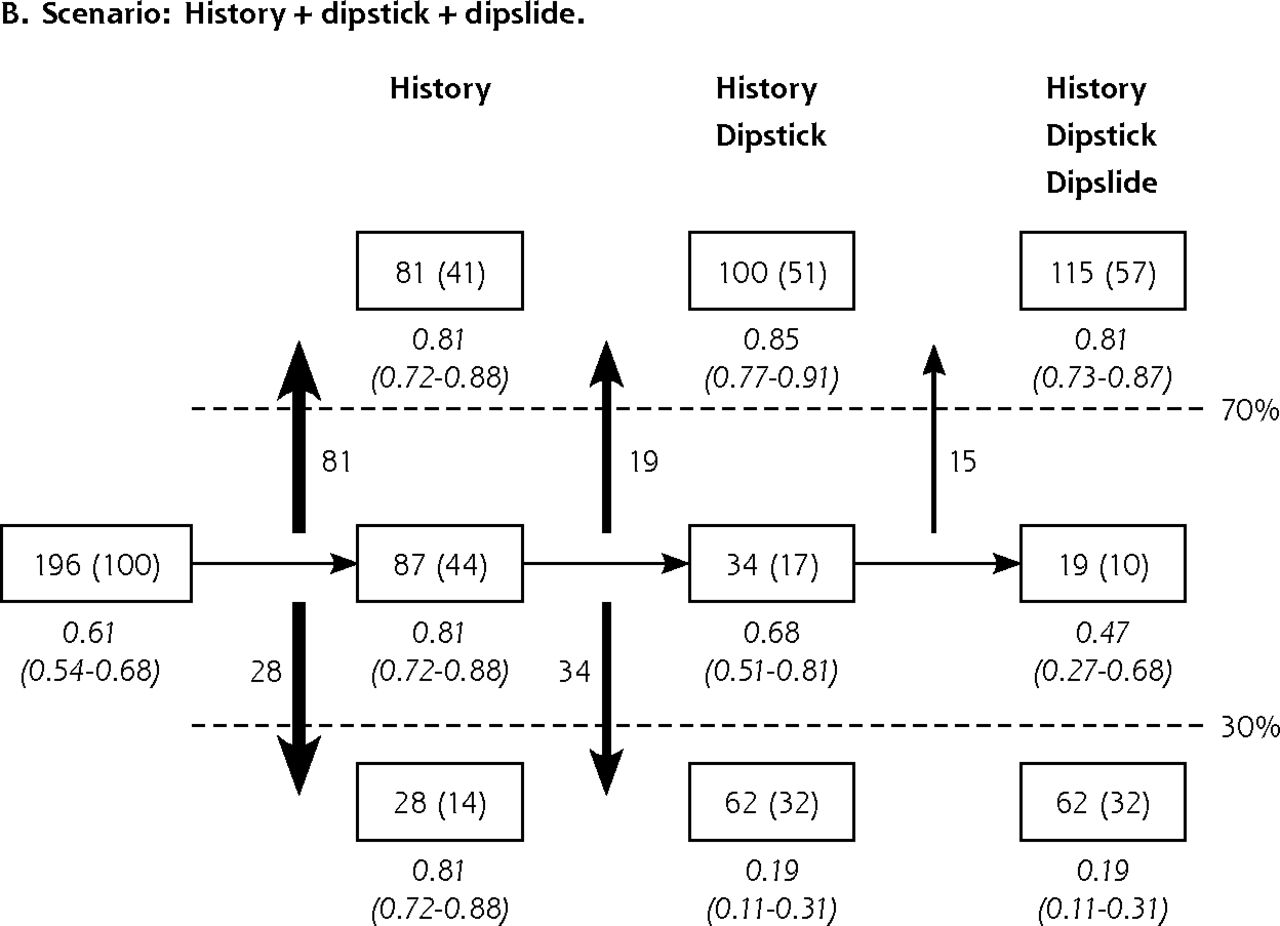
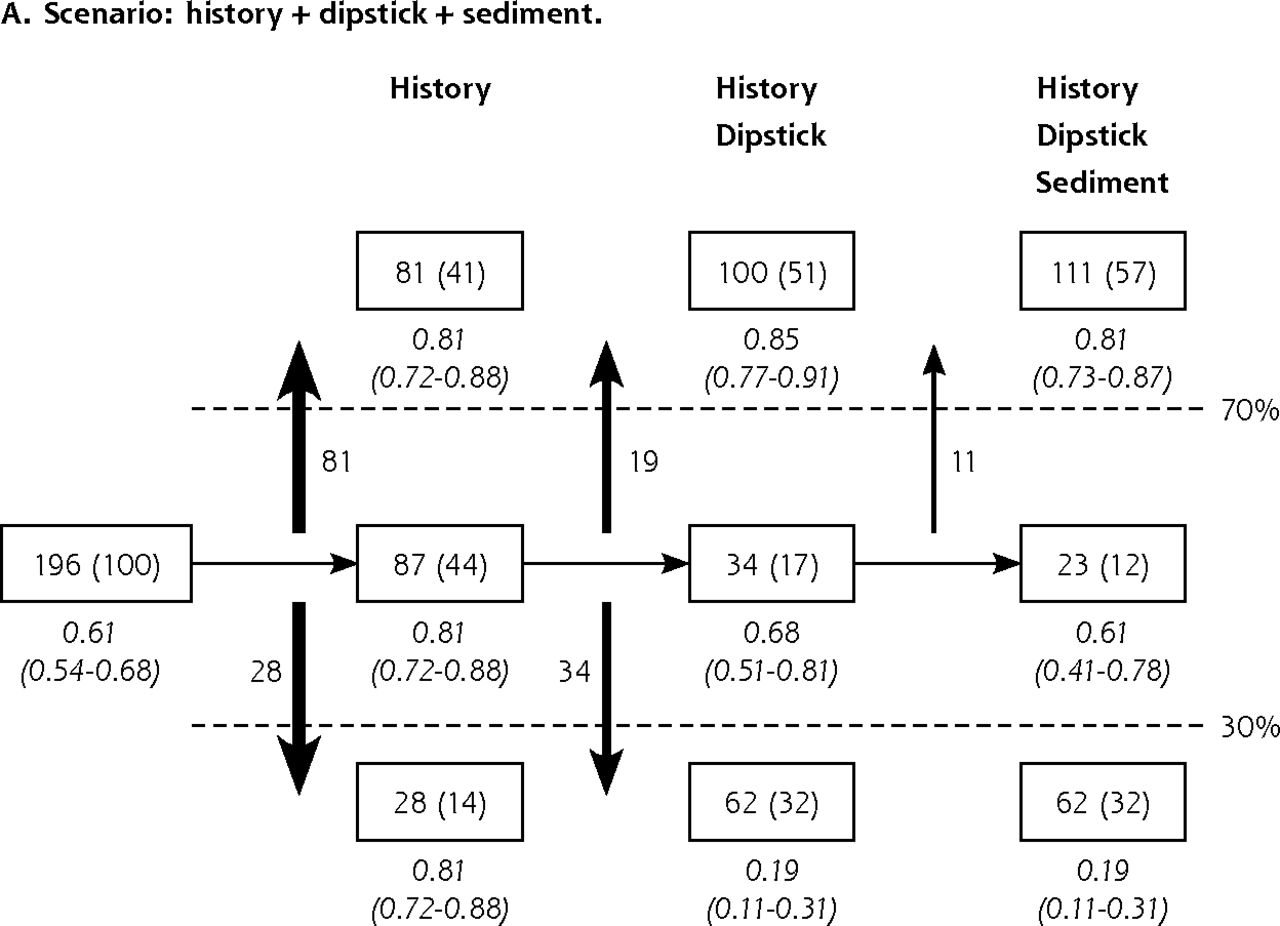
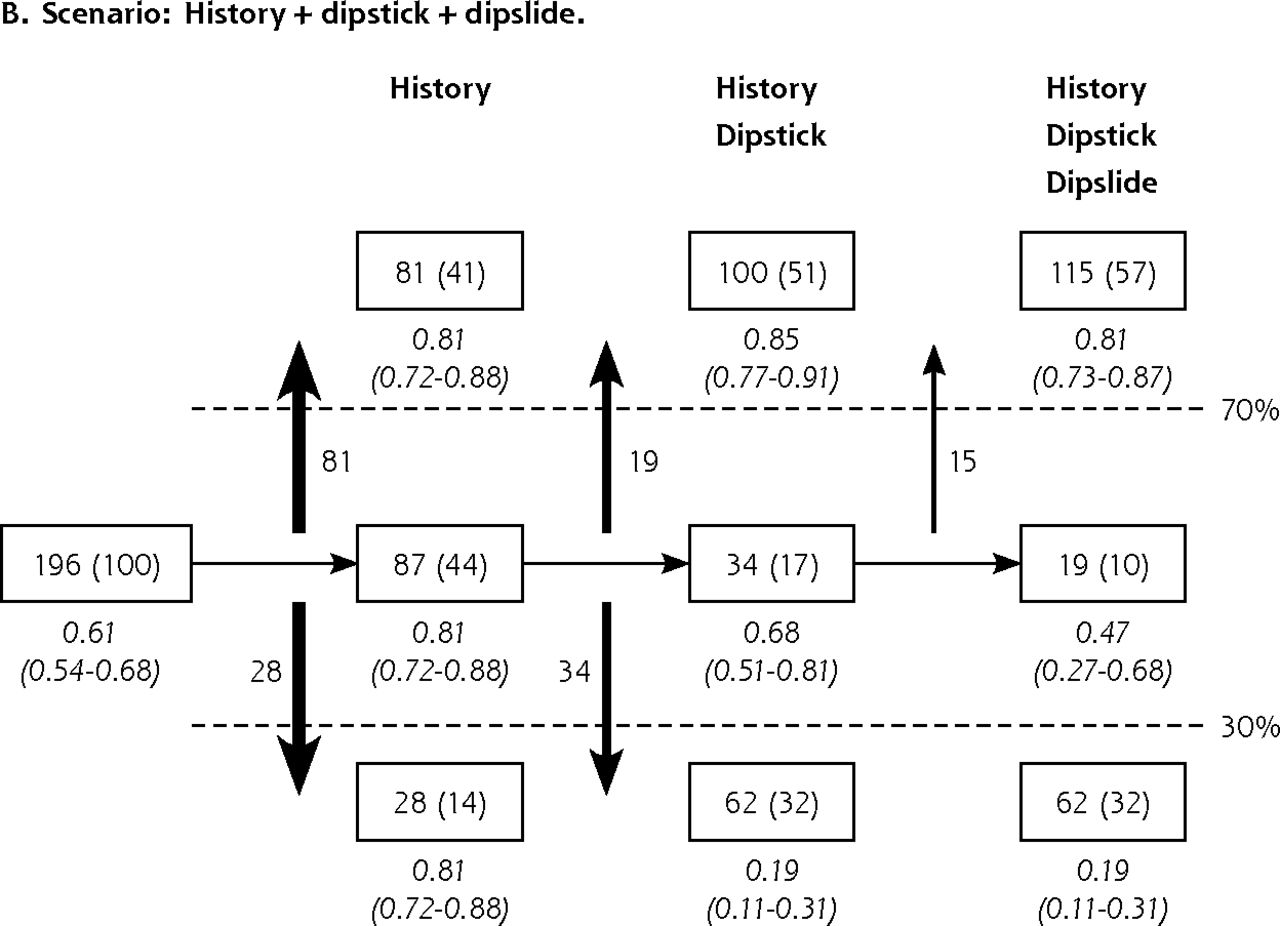
- Figure 2
Discrimination by subsequent tests when performed in patients in the intermediate risk category only.
UTI=urinary tract infection.
Notes: In the boxes, patient numbers (percent) in each predicted risk category are shown after application of each subsequent diagnostic model to patients in the intermediate predicted risk category only for the scenarios history + dipstick + sediment and history + dipstick + dipslide (Figure 2A and 2B, respectively). The predicted risk categories used are <30%, 30%–70% and >70%. The vertical arrows display the numbers of patients that moved from the intermediate risk category to one of the extreme risk categories (<30% or >70%) after performing a test. The observed risks (95% CI) are in italics.
Figures are best read from left to right: 196 patients (100%) were included, and the prevalence of UTI was 61%. Based on the results from the history questions only, 28 patients (14%) had a predicted risk of <30% and 81 patients (41%) had a predicted risk of >70%. After subsequent performance of a urine dipstick for patients in the intermediate risk category, 62 patients (32%) had a predicted risk of <30%, 100 patients (51%) had a predicted risk of >70%, and 34 patients (17%) remained in the intermediate risk category (between 30% and 70%) as the result of a negative nitrite test and a positive blood test. Subsequent performance of either a sediment or a dipslide reclassified 5% or 7%, respectively, of patients from the intermediate category into the high-risk category (>70%) because of a positive test result (Figure 2A and 2B, respectively). All observed risks were close to the predicted risks (good calibration).

Tables
Characteristic No. (% of Total) Culture Sample, No. Positive Culture % Positive Negative Total 196 (100) 120 76 61 Ethnicity Dutch/German 171 (87) 107 64 63 Surinam/Antillian/Aruban 15 (8) 6 9 40 Other 10 (5) 7 3 70 General health Very good 22 (11) 12 10 55 Good 110 (56) 74 36 67 Reasonable 44 (22) 25 19 57 Moderate 11 (6) 7 4 64 Bad 9 (5) 2 7 22 Marital status Married 81 (41) 51 30 63 Partner, cohabitating 31 (16) 20 11 65 Partner, living apart 36 (18) 24 12 67 Single 48 (24) 25 23 52 ≥ First-grade relative with recurrent UTIs? No 137 (70) 83 54 61 Yes 59 (30) 37 22 63 Last menstruation >1 year ago? No 133 (68) 81 52 61 Yes 63 (32) 39 24 62 Diabetes mellitus according to patient? No 172 (88) 111 61 65 Yes 24 (12) 9 15 38 Times of sexual activity in past week 0 67 (34) 34 33 51 1 39 (20) 23 16 59 2 40 (21) 33 7 83 3 22 (11) 14 8 64 4 14 (7) 9 5 64 ≥5 14 (7) 7 7 50 UTIs in past year according to patient 0 92 (47) 57 35 62 1 28 (14) 24 4 86 2 30 (15) 19 11 63 ≥3 32 (16) 15 17 47 Don’t know 14 (7) 5 9 36 ≥1 UTI ever diagnosed according to patient? No 42 (21) 24 18 57 Yes 154 (79) 100 54 65 Patient thinks she has a UTI? No 9 (5) 4 5 44 Yes 164 (84) 114 50 70 Don’t know 23 (12) 2 21 9 Symptoms Duration of symptoms, d 0 18 (9) 12 6 67 1 40 (20) 28 12 70 2 37 (19) 23 14 62 3 37 (19) 22 15 59 4 24 (12) 14 10 58 ≥5 40 (20) 21 19 53 False urge to urinate No 54 (28) 30 24 57 A little 82 (42) 53 29 65 Quite much 43 (22) 27 16 63 Very much 17 (9) 10 7 59 More frequent micturition than usual No 12 (6) 3 9 25 A little 62 (32) 31 31 50 Quite much 81 (42) 59 22 73 Very much 41 (21) 27 14 66 Pain during micturition No 35 (18) 14 22 39 A little 73 (37) 39 34 53 Quite much 64 (33) 53 11 83 Very much 23 (12) 14 9 61 Urge to urinate hard to control No 49 (25) 22 27 45 A little 88 (45) 57 31 65 Quite much 33 (17) 24 9 73 Very much 26 (13) 17 9 65 Vaginal discharge No 133 (68) 86 47 65 A little 49 (25) 27 22 55 Quite much 14 (7) 7 7 50 Very much 0 (0) 0 0 n/a Vaginal irritation or itching No 110 (56) 72 38 65 A little 57 (29) 28 29 49 Quite much 19 (10) 15 4 79 Very much 10 (5) 5 5 50 Bother at work/school No 24 (13) 9 15 38 Hardly 37 (19) 21 16 57 Moderate 69 (35) 48 21 70 Much 46 (23) 29 17 63 Very much 20 (10) 13 7 65 Bother at social activities No 47 (24) 24 23 51 Hardly 49 (25) 29 20 59 Moderate 53 (27) 36 17 68 Much 33 (17) 21 12 64 Very much 14 (7) 10 4 71 -
n/a=not applicable; UTI=urinary tract infection.
-
a Percentages represent the fraction of positive cultures for the corresponding characteristic, eg, 70% of patients with symptoms for 1 day had a positive culture (implying that the positive predictive value of having symptoms for 1 day is 70%).
-
Characteristic No. (% of Total) Culture Result, No. Positive Culture, %a Positive Negative Total 196 (100) 120 76 61 Dipstick Blood Negative 35 (18) 11 24 31 Trace 38 (20) 15 23 39 1+ 29 (14) 20 9 69 2+ 36 (19) 26 10 72 3+ 58 (30) 48 10 82 Leukocytes Negative 39 (20) 10 29 26 Trace 15 (8) 5 10 33 1+ 47 (24) 31 16 66 2+ 35 (18) 27 8 77 3+ 60 (31) 47 13 78 Nitrate positive No 133 (68) 60 73 45 Yes 62 (32) 60 3 95 Sediment Bacteria, No./HPF None 52 (27) 18 34 35 Few 48 (24) 27 17 56 Many 53 (27) 40 13 75 Very many 43 (22) 35 8 81 Leukocytes, No./HPF 0 26 (13) 6 20 23 1–3 32 (16) 9 23 28 4–10 18 (9) 9 9 50 11–20 24 (12) 14 10 58 ≥20 96 (49) 82 14 85 Dipslide CLED medium, CFU/mL <103 64 (33) 21 43 33 103–104 32 (16) 10 22 31 104–105 10 (5) 6 4 60 ≥105 90 (46) 83 7 92 -
CFU = colony-forming unit; CLED = cystine lactose electrolyte deficient; HPF = high-power field.
-
↵a Percentages represent the fraction of positive cultures for the corresponding characteristic.
-
- Table 3
Clinical Scores for History Only and History + Dipstick: Regression Coefficients and Scores of Selected Indicators
Indicatora History Only History+Dipstick Odds Ratio (95% CI) Coefficient Score Odds Ratio (95% CI) Coefficient Score History Patient thinks she has a UTI 8.85 (3.35–24.05) 2.18 8 15.64 (3.94–63.43) 2.75 11 At least considerable pain on micturition 2.80 (1.52–5.16) 1.03 4 0.97 (0.91–1.03) −0.03 0b Vaginal irritationc 0.77 (0.54–1.08) −0.26 −1 0.61 (0.36–1.04) −0.50 −2 Dipstick Nitrate positive – – – 31.19 (7.39–130.32) 3.44 14 Blood ≥1+ – – – 7.32 (3.03–17.81) 1.99 8 Regression intercept – −1.77 – – −3.89 – -
UTI=urinary tract infection.
-
↵a Indicators from history and urine dipstick that were retained after logistic regression analysis with bootstrapped backward elimination (P remove .05).
-
↵b This clinical score of 0 had no added value.
-
↵c Vaginal irritation reduced the probability of a positive culture, whereas the other indicators increased it.
-
- Table 4
Clinical Scores for History Only, and History + Dipstick: Sum Scores and Predicted Probabilities per Risk Category
Risk Category History Only History+Dipstick Score Predicted Probability (95% CI) Score Predicted Probability (95% CI) <30% ≤3 16 (7–34) ≤12 15 (7–31) 30%–70% 4–8 56 (44–68) 14–17 61 (41–77) >70% ≥11 79 (69–86) ≥19 91 (76–96) -
Notes: For example, for history only, patients with a sum score of ≥3 have a predicted probability of 16% and are therefore classified into the lowest risk category (<30%).
-
Supplemental Appendix
Supplemental Appendix. Detailed Description of Variable Selection Method
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file, 2 pages
The Article in Brief
Toward a Simple Diagnostic Index for Acute Uncomplicated Urinary Tract Infections
Bart J. Knottnerus , and colleagues
Background Sixty percent of all women experience at least one acute uncomplicated urinary tract infection (UTI) during their life. Various medical history questions and urine investigations can be used for UTI diagnosis. This study analyzes different approaches to diagnosing acute uncomplicated urinary tract infections in women and proposes a model that reduces the number of questions asked and urine investigations needed.
What This Study Found Analyzing data on 196 women presenting with painful and/or frequent urination, researchers find that 3 questions, sometimes followed by a urine dipstick test, can provide a practical level of accuracy. Specifically, they recommend asking (1) does the patient think she has a UTI, (2) is there at least considerable pain on urination and (3) is there vaginal irritation? Asking these questions, they find, may be sufficient to correctly classify more than one-half of women with painful and/or frequent urination as having UTI risk of either less than 30 percent or greater than 70 percent. Subsequent performance of nitrite and blood dipstick tests raises this proportion to 73 percent. The percentage rises to 83 percent if a urine dipstick is performed only for patients with a UTI risk between 30 percent and 70 percent after history and avoids the possibility of a false-negative nitrate tests in patients with high UTI risk (greater than 70 percent) after history.
Implications
- Expensive and time-consuming urinary sediment and dipslide tests may add little diagnostic information. The authors call for future research to validate these recommendations.
Annals Journal Club
Sep/Oct 2013: Diagnosing Urinary Tract Infections
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1
HOW IT WORKS
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/site/AJC/.
CURRENT SELECTION
Article for Discussion
- Knottnerus BJ, Geerlings SE, Moll van Charante EP, ter Riet G. Toward a simple diagnostic index for acute uncomplicated urinary tract infections. Ann Fam Med. 2013;11(5):442-451.
Discussion Tips
Urinary tract infections are common, and clinicians' diagnostic approaches are based on long tradition, local practice, and personal experience. This interesting clinical study provides empirical information on the conjoint diagnostic value of combinations of medical history and simple laboratory testing for acute uncomplicated urinary tract infections in women with painful and/or frequent urination.
Discussion Questions
- What question is asked by this study, and why does it matter?
- How does this study advance beyond previous research and clinical practice on this topic?
- How strong is the study design for answering the question?
- To what degree can the findings be accounted for by:
- How patients were selected, excluded, or lost to follow-up?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How the findings were interpreted?
- What do you think of the outcome variable?
- How comparable is the study sample to similar patients in your practice? What is your judgment about the transportability of the findings?
- What are the main study findings?
- Which approach indicated by the different models do you think you are likely to use, and how might your approach vary based on patient characteristics?
- Do you think the findings have implications for self-treatment by selected patients?
- What are the next steps in interpreting or applying the findings?
- What researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals Journal Club: It's time to get RADICAL. Ann Fam Med. 2006;4(3):196-197.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Knowledge, attitudes and practices around urinary tract infections of general practitioners in the Netherlands: a cross-sectional internet survey
- Impact of sociodemographic status and UTI symptoms on womens health-care seeking and management in England: findings from an e-survey conducted during the first year of the COVID-19 pandemic
- Diagnosis of urinary tract infection based on symptoms: how are likelihood ratios affected by age? a diagnostic accuracy study
- Predicting the use of antibiotics after initial symptomatic treatment of an uncomplicated urinary tract infection: analyses performed after a randomised controlled trial
- Diagnosing Urinary Tract Infections
- In This Issue: Mindfulness in Practice and Policy