
Article Figures & Data
Figures
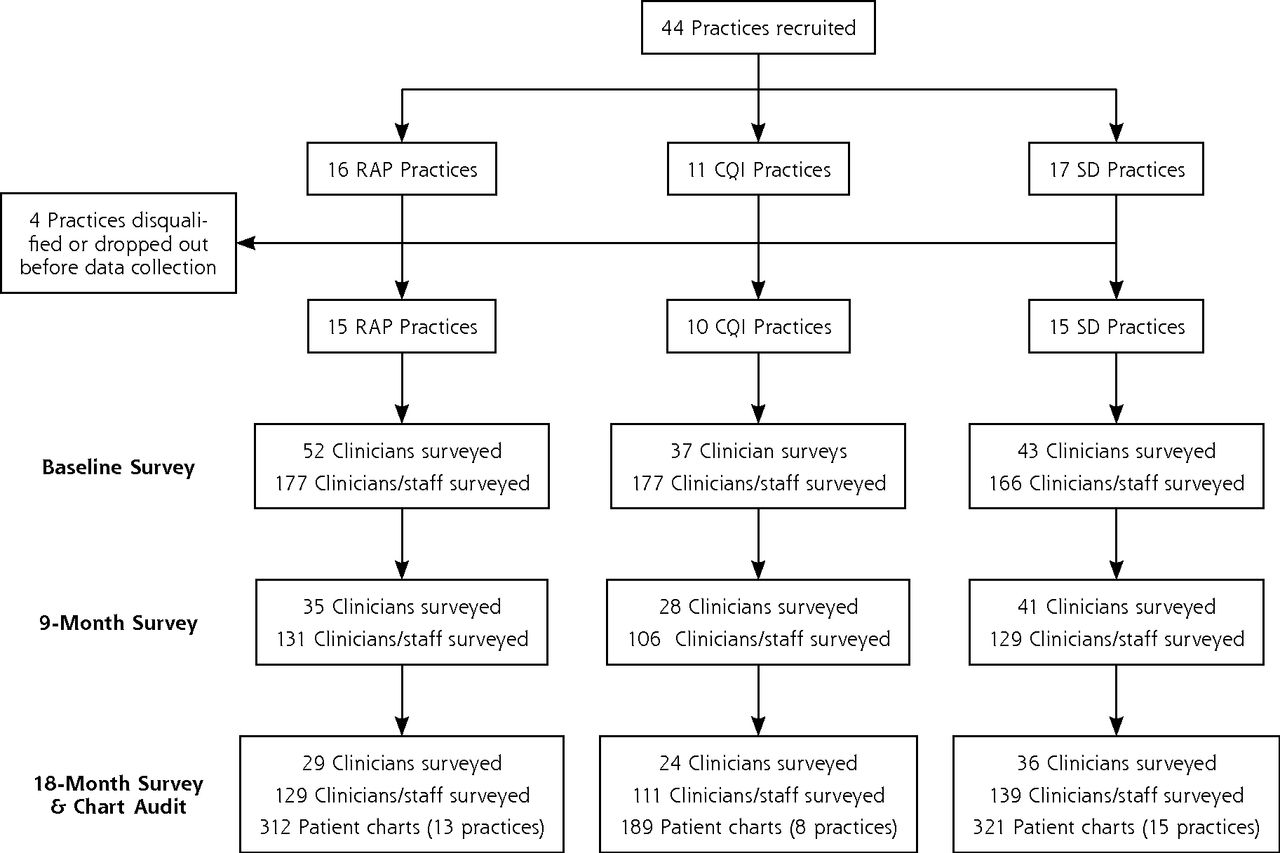
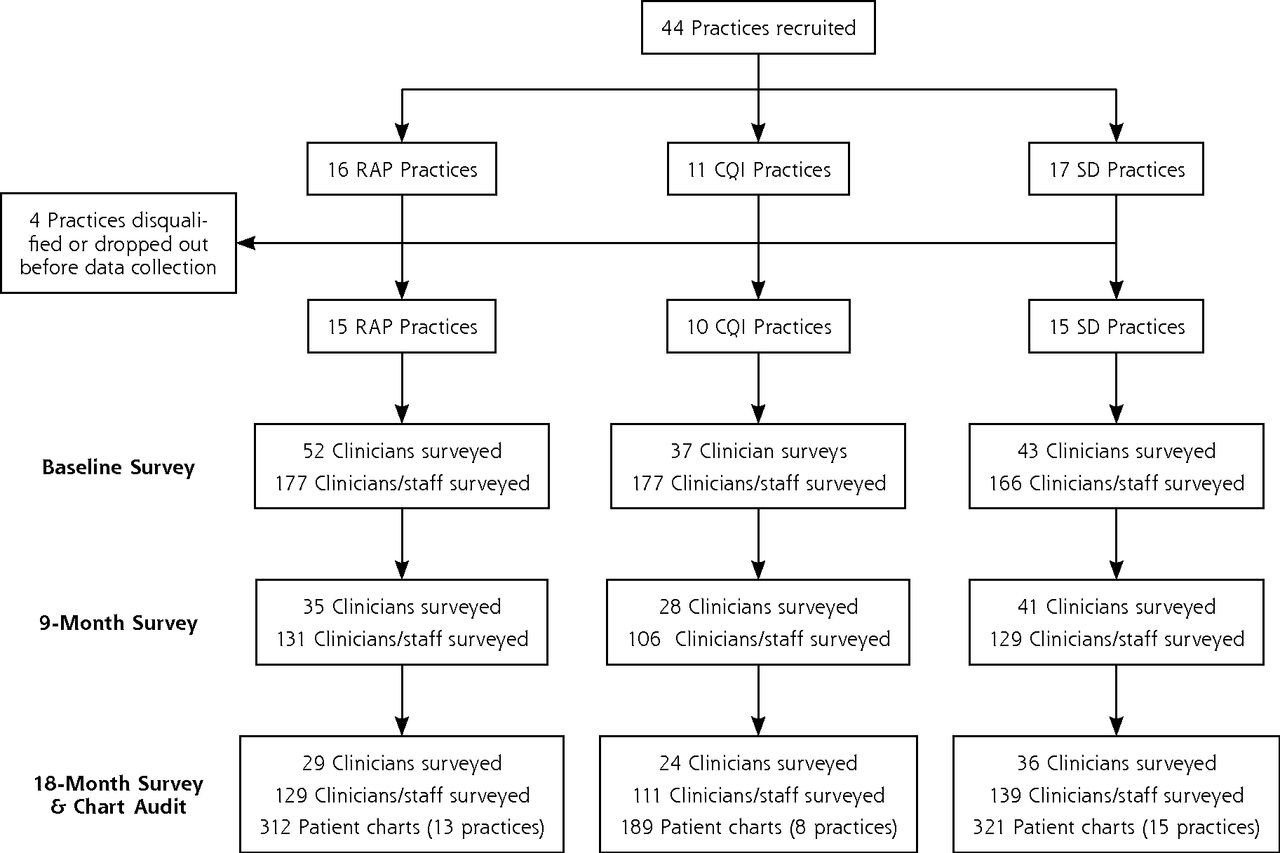
- Figure 1
CONSORT diagram.
CONSORT = Consolidated Standards of Reporting Trials; CQI = continuous quality improvement; RAP = reflective adaptive process; SD = self-directed.
Notes: 2 RAP practices and 2 CQI practices had limited or no active participation after baseline. Clinicians surveyed using the Assessment of Clinician Diabetes Management included all physicians, nurse practitioners, and physician assistants. Clinicians and staff surveyed using the Practice Culture Assessment included everyone in any role in the practice.
Tables
Characteristic RAP CQI SD Practices (n = 15) (n = 10) (n = 15) Rural, No. (%) 4 (27) 2 (20) 4 (27) Practice size (office visits per week), No. (%) Large (>400) 3 (20) 1 (10) 3 (33) Medium (91–400) 10 (67) 4 (40) 10 (47) Small (1–90) 2 (13) 5 (50) 2 (20) Patients on Medicaid, % <5% 8 (53) 4 (40) 6 (40) 5%–20% 3 (20) 4 (40) 4 (27) >20% 4 (27) 2 (20) 5 (33) Patientsa (n = 312) (n = 189) (n = 321) Sex, % male 44.2 52.9 50.5 Age, mean (SD), y 60.5(12.6) 61.9 (12.1) 60.0 (13.2) Medical comorbidities, mean (SD), No.b 2.1 (1.2) 2.0 (1.3) 2.0 (1.1) Have psychiatric comorbidity, %c 20.5 14.3 13.1 HbA1c level, mean (SD), %d 7.18 (1.59) 7.35 (1.76) 7.69 (2.00) Systolic blood pressure, mean (SD), mm Hgd 128.3 (16.4) 131.8 (17.7 132.9 (19.7) Diastolic blood pressure, mean (SD), mm Hg 76.9 (10.9) 78.5 (12.2) 78.0 (11.9) Total cholesterol level, mean (SD), mg/dLe 174.5 (42.6) 185.8 (49.3) 184.8 (50.4) -
CQI = continuous quality improvement; HbA1c = hemoglobin A1c; RAP = reflective adaptive process; SD = self-directed.
-
↵a HbA1c levels were determined for 636 patients, systolic and diastolic blood pressure for 799 patients, and total cholesterol levels for 703 patients.
-
↵b Arthritis, connective tissue disease, gastrointestinal problems, coronary disease, hyperlipidemia, hypertension, liver disease, pulmonary disease, neurologic disease, peripheral vascular disease, renal disease, stroke, dementia, cancer in past 3 years.
-
↵c Depression, substance abuse, other psychiatric diagnosis.
-
↵d P <.01.
-
↵e P <.05.
-
Quality Measure RAP CQI SD Differential Change Over Time P Value Total process of care scorea Baseline 4.54 3.58 3.63 Overall: F4,2386 = 10.70 <.0001 9 months 4.69 4.91 4.04 RAP × SD: F2,1838 = 3.65 .03 18 months 4.85 4.91 4.39 CQI × SD: F2,1475 = 9.99 <.0001 …b …c …c CQI × RAP: F2,1455 = 19.27 <.0001 HbA1c level checked, % Baseline 85.8 69.9 77.6 Overall: F4,1568 = 0.49 .09 9 months 91.7 92.3 88.2 RAP × SD: F2,1208 = 0.14 .87 18 months 93.7 91.0 89.3 CQI × SD: F2,968 = 2.98 .051 …c …c …c CQI × RAP: F2,957 = 3.35 .04 Feet checked, % Baseline 43.5 34.1 35.1 Overall: F4,1568 = 2.98 .02 9 months 57.9 60.8 41.5 RAP × SD: F2,1208 = 14.86 .34 18 months 60.2 68.7 52.2 CQI × SD: F2,968 = 4.80 .009 …c …c …c CQI × RAP: F2,957 = 3.57 .03 Blood pressure checked, % Baseline 92.1 84.2 86.5 Overall: F4,1567 = 0.34 .85 9 months 99.5 99.6 98.8 RAP × SD: F2,1207 = 0.03 .97 18 months 99.7 99.1 99.5 CQI × SD: F2,967 = 0.66 .51 …c …c …c CQI × RAP: F2,957 = 0.38 .68 Dilated eye examination, % Baseline 16.1 8.5 6.0 Overall: F4,1567 = 2.35 .052 9 months 16.0 18.1 5.3 RAP × SD: F2,1207 = 1.23 .29 18 months 22.4 18.1 12.6 CQI × SD: F2,967 = 3.39 .03 …d …c …c CQI × RAP: F2,957 = 2.66 .07 Cholesterol checked, % Baseline 81.7 61.8 71.4 Overall: F4,1567 = 6.11 <.0001 9 months 78.8 86.4 79.5 RAP × SD: F2,1207 = 3.64 .03 18 months 79.9 79.5 81.1 CQI × SD: F2,967 = 4.21 .02 … …c …c CQI × RAP: F2,957 = 11.78 <.0001 Nephropathy screening, % Baseline 38.1 18.7 24.4 Overall: F4,1567 = 2.04 .09 9 months 33.1 27.7 20.2 RAP × SD: F2,1207 = 0.30 .74 18 months 33.6 26.9 23.8 CQI × SD: F2,967 = 2.90 .056 … …d … CQI × RAP: F2,957 = 3.44 .03 Influenza vaccination, % Baseline 27.7 28.7 18.0 Overall: F4,1567 = 3.01 .02 9 months 29.6 45.3 21.8 RAP × SD: F2,1207 = 3.96 .02 18 months 25.9 44.3 30.0 CQI × SD: F2,967 = 1.52 .22 … …c …c CQI × RAP: F2,957 = 3.30 .04 Nutrition counseling, % Baseline 38.0 16.7 21.3 Overall: F5,1567 = 2.61 .03 9 months 32.4 26.1 24.1 RAP × SD: F2,1207 = 1.62 .19 18 months 38.1 29.6 20.8 CQI × SD: F2,967 = 2.76 .06 … …b … CQI × RAP: F2,957 = 3.86 .02 Self-management support, % Baseline 20.4 22.2 12.9 Overall: F4,1567 = 1.09 .36 9 months 18.8 24.4 14.2 RAP × SD: F2,1207 = 1.57 .21 18 months 21.4 24.2 21.0 CQI × SD: F2,967 = 1.35 .26 … … …b CQI × RAP: F2,957 = 0.23 .79 -
CQI = Continuous Quality Improvement; HbA1c = hemoglobin A1c; RAP = Reflective Adaptive Process; SD = self-directed.
-
Note: Data are from chart audits. All measures pertain to whether care was provided in past 12 months.
-
↵a Possible scores ranged from 0 to 9, with higher scores indicating better quality of diabetes care.
-
↵b P <.05 within-group change.
-
↵c P <.01 within-group change.
-
↵d P <.10 within-group change.
-
Item Change Culture Work Culture Chaos After making a change, we discuss what worked and what didn’t. 0.66398 … … This practice puts a great deal of effort into improving the quality of care. 0.67917 … … This practice encourages everybody’s input for making changes. 0.81108 … … We regularly take time to consider ways to improve how we do things. 0.79724 … … The practice leadership makes sure that we have the time and space necessary to discuss changes to improve care. 0.78396 … … This practice uses data and information to improve the work of the practice. 0.62714 … … Our practice encourages people to share their ideas about how to improve things. 0.79928 … … The leadership in this practice is available to discuss work related problems 0.72885 … … When we experience a problem in the practice we make a serious effort to figure out what’s really going on. 0.72684 … … The leadership of this practice is good at helping us to make sense of problems or difficult situations. 0.74846 … … My opinion is valued by others in this practice. … 0.69821 … People in this practice understand how their jobs fit into the rest of the practice. … 0.65733 … I can rely on the other people in this practice to do their jobs well. … 0.73350 … When there is conflict or tension in this practice, those involved are encouraged to talk about it. … 0.67104 … People in this practice are thoughtful about how they do their jobs … 0.77181 … People in this practice pay attention to how their actions affect others in the practice. … 0.74617 … Most of the people who work in our practice seem enjoy their work. … 0.76567 … The practice leadership promotes an environment that is an enjoyable place to work. … 0.76768 … This practice is almost always in chaos. … … 0.71993 This practice is very disorganized. … … 0.73899 Our practice has recently been very stable. … … −0.67600 Things have been changing so fast in our practice that it is hard to keep up with what is going on. … … 0.58880 Subscale RAP CQI SD Differential Change Over Time P Value Change Culture Baseline 66.2 69.5 67.1 Overall: F4,66 = 1.91 .12 9 months 68.5 68.5 66.6 RAP × SD: F2,52 = 3.33 .04 18 months 64.0 67.3 66.9 CQI × SD: F2,42 = 0.51 .60 …a … … CQI × RAP: F2,38 = 1.75 .19 Chaos Baseline 47.7 43.4 49.0 Overall: F4,66 = 3.47 .01 9 months 50.2 46.8 50.0 RAP × SD: F2,52 = 3.87 .03 18 months 50.8 48.2 47.3 CQI × SD: F2,42 = 5.63 .007 …b …b … CQI × RAP: F2,38 = 0.49 .62 Work Culture Baseline 69.8 68.7 66.5 Overall: F4,66 = 2.34 .06 9 months 68.8 69.2 68.1 RAP × SD: F2,52 = 4.59 .01 18 months 66.4 68.6 68.5 CQI × SD: F2,42 = 0.49 .62 …b … … CQI × RAP: F2,38 = 1. 59 .22
The Article in Brief
Practice Facilitation to Improve Diabetes Care in Primary Care: A Report From the EPIC Randomized Clinical Trial
W. Perry Dickinson , and colleagues
Background Many practice redesign efforts focus on implementing the Chronic Care Model, which summarizes basic elements for improving care in health systems at the community, organization, practice and patient levels. The current study compares the effectiveness of three different Chronic Care Model-based approaches to improve diabetes care in primary care. The three approaches are 1) Continuous Quality Improvement (CQI) in which practices follow a strategy of implementing registries to have diabetes quality measures motivate practice action, identify needed changes, and monitor progress; 2) Reflective Adaptive Process (RAP) in which practices follow a more practice-determined approach for improving practice culture; and 3) Self-Directed (SD) in which practices are given information and resources about the Chronic Care Model and quality improvement but without the assistance of a facilitator.
What This Study Found All methods resulted in significant improvement in diabetes care measures, but there were differences in the extent and duration of improvement and trade-offs in work culture change. Although measures of the quality of diabetes care improved in all three groups, improvement was greater in CQI practices compared with both SD and RAP practices, and greater in SD practices compared with RAP practices. In RAP practices, change culture scores showed a trend toward improvement at nine months, but decreased below baseline at 18 months, and work culture scores decreased from nine to 18 months. Both scores were stable over time in SD and CQI practices.
Implications
- Traditional CQI interventions are effective at improving measures of the quality of diabetes care, but may not improve practice culture.
- Short-term practice facilitation based on RAP principles appears to be less effective at improving quality measures and does not produce sustained improvements in practice culture.
- Recognizing that not all primary care practices need the same type, intensity, or duration of assistance, the authors call for practices to tailor the approach to their practice. They also call for the development and testing of new models that can produce the long-term improvements in both quality measures and practice cultures necessary for sustained care enhancement.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Successful Implementation of Integrated Behavioral Health
- Improving Care for Unhealthy Alcohol Use: Results from the Facilitating Alcohol Screening and Treatment (FAST) Colorado Study
- An Assessment of Weight Loss Management in Health System Primary Care Practices
- Improving Delivery of Cardiovascular Disease Preventive Services in Small-to-Medium Primary Care Practices
- Improving Delivery of Cardiovascular Disease Preventive Services in Small-to-Medium Primary Care Practices
- Determining feasibility of incorporating consumer engagement into implementation activities: study protocol of a hybrid effectiveness-implementation type II pilot
- Successful Trial of Practice Facilitation for Plan, Do, Study, Act Quality Improvement
- A Taxonomy for External Support for Practice Transformation
- Implementation of Community-Based Resource Referrals for Cardiovascular Disease Self-Management
- Adapting Diabetes Shared Medical Appointments to Fit Context for Practice-Based Research (PBR)
- Practice Transformation Support and Patient Engagement to Improve Cardiovascular Care: From EvidenceNOW Southwest (ENSW)
- Identifying Practice Facilitation Delays and Barriers in Primary Care Quality Improvement
- Sequential third-year medical student quality assurance (QA) clerkship projects appear to introduce a culture of continuous quality improvement across New Jersey family medicine practices
- Practice Characteristics Associated with Better Implementation of Patient Self-Management Support
- Practice Facilitator Strategies for Addressing Electronic Health Record Data Challenges for Quality Improvement: EvidenceNOW
- Experiences of practice facilitators working on the Improved Delivery of Cardiovascular Care project: Retrospective case study
- A Randomized Trial of High-Value Change Using Practice Facilitation
- Facilitation roles and characteristics associated with research use by healthcare professionals: a scoping review
- Strategies to Support the Integration of Behavioral Health and Primary Care: What Have We Learned Thus Far?
- Pragmatic Cluster Randomized Trials Using Covariate Constrained Randomization: A Method for Practice-based Research Networks (PBRNs)
- Do Experiences Consistent With a Medical-Home Model Improve Diabetes Care Measures Reported by Adult Medicaid Patients?
- In This Issue: Team-Based Care and Information to Improve Practice