
Abstract
PURPOSE An isolated focus on 1 disease at a time is insufficient to generate the scientific evidence needed to improve the health of persons living with more than 1 chronic condition. This article explores how to bring context into research efforts to improve the health of persons living with multiple chronic conditions (MCC).
METHODS Forty-five experts, including persons with MCC, family and friend caregivers, researchers, policy makers, funders, and clinicians met to critically consider 4 aspects of incorporating context into research on MCC: key contextual factors, needed research, essential research methods for understanding important contextual factors, and necessary partnerships for catalyzing collaborative action in conducting and applying research.
RESULTS Key contextual factors involve complementary perspectives across multiple levels: public policy, community, health care systems, family, and person, as well as the cellular and molecular levels where most research currently is focused. Needed research involves moving from a disease focus toward a person-driven, goal-directed research agenda. Relevant research methods are participatory, flexible, multilevel, quantitative and qualitative, conducive to longitudinal dynamic measurement from diverse data sources, sufficiently detailed to consider what works for whom in which situation, and generative of ongoing communities of learning, living and practice. Important partnerships for collaborative action include cooperation among members of the research enterprise, health care providers, community-based support, persons with MCC and their family and friend caregivers, policy makers, and payers, including government, public health, philanthropic organizations, and the business community.
CONCLUSION Consistent attention to contextual factors is needed to enhance health research for persons with MCC. Rigorous, integrated, participatory, multimethod approaches to generate new knowledge and diverse partnerships can be used to increase the relevance of research to make health care more sustainable, safe, equitable and effective, to reduce suffering, and to improve quality of life.
INTRODUCTION
More than 1 in 4 Americans lives with the burden of more than 1 ongoing health condition,1–3 and the number of persons living with multiple chronic health conditions is growing dramatically.2,4 Medical costs for persons with chronic illnesses account for 75% of US health care spending,4 and more than 90% of the Medicare spending on older adults is devoted to persons suffering from multiple chronic conditions (MCC).5 This heavy expenditure has not yielded the desired increase in quality of life for those affected.4 A strategic framework of the Department of Health and Human Services (DHHS)6 and multiple proposals and programs from the private sector highlight the growing concern about persons living with MCC.7
Current health care and research approaches are largely mismatched to the challenge of persons living with MCC. Both health care and research are primarily focused on single diseases.8,9 Most prevailing scientific approaches are designed to isolate objects of inquiry, controlling for potentially confounding contextual factors that are treated as noise to be muffed. Although reductionist research can yield useful information on the causes and consequences of single diseases, it is not well suited to addressing multifaceted problems, such as understanding the complex interaction of multimorbid chronic illnesses with social, environmental, and health care systems.10,11 Indeed, most randomized clinical trials12 and the evidence-based guidelines derived from them not only exclude persons with MCC,13 but attempt to hold contextual factors constant, thus contributing to evidence-based care that is fragmented and potentially harmful.14–16
Context involves the many factors that influence a person’s life, from the biology of interacting diseases or treatments, to the values and life goals of the individual and family, the health and functioning of family and friend caregivers, and relevant health care system factors, community resources, and policies. These multilevel,17–21 complexly interacting factors are important for understanding MCC, for ensuring optimal benefit of preventive and therapeutic interventions, and for improving the lives of persons living with MCC.
As a result of fragmented, decontextualized research and health care, persons living with chronic illnesses, as well as their family and friend caregivers, often feel isolated and unsupported. Their health care is often splintered,10,22,23 potentially dangerous,24–28 unguided by relevant scientific knowledge,13,29,30 and unsustainably expensive.31–37
The purpose of this article is to (1) identify domains of important contextual factors for research on MCC, (2) advance the research agenda, (3) recommend relevant research methods, and (4) suggest partnerships helpful for collaborative action. Its goal is better care and a higher quality of life for persons with MCC and their families and lower costs for society.
METHODS
In 2012, planning began to bring together a diverse group of expert stakeholders to address the need to incorporate context into research to improve the health of those living with MCC. Members of the planning group included representatives of the National Institutes of Health, the DHHS Office of the Assistant Secretary of Health, the Agency for Healthcare Research and Quality, the Centers for Disease Control and Prevention, the National Council on Aging, and the Patient-Centered Outcomes Research Institute. The planning process was guided by a logic model depicted in Figure 1, which shows how input from diverse participants, focused on 4 goal-directed activities, was hypothesized to lead to short-, intermediate- and long-term outcomes for persons living with MCC.

Logic model guiding the multiple chronic conditions in context initiative.
AHRQ = Agency for Healthcare Research and Quality; DHHS = Department of Health and Human Services; NIH = National Institutes of Health.
Forty-five invited experts met in Washington, DC, February 27–28, 2013, at the Patient-Centered Outcomes Research Institute. Participants were invited by the planning committee to represent the experience of individuals with MCC, family and friend caregivers, researchers, funders, nongovernmental agencies, policy makers, clinicians, and health care system and public health specialists.
Participants were assigned to small working groups with diverse representation to examine critically the 4 topic areas: (1) key contextual factors, (2) needed research, (3) relevant research methods, and (4) partnerships for collaborative action. Each group summarized their work in writing and shared their findings with all participants in an iterative process designed to challenge and refine the emerging insights.
Subsequently, one meeting facilitator (K.C.S.) blended the group reports into a common document that was refined by group leaders, and the other meeting facilitator (W.J.N.) then iteratively honed by participants after the meeting.
FINDINGS
Key Contextual Factors
The complex interaction of contextual factors relevant for persons with MCC occurs at multiple levels, from policy to health care system, community, family, person, and the underlying biology. A multilevel classification of key contextual factor categories, selected subcategories, and examples are depicted in Table 1. The World Health Organization succinctly sums it up in the statement: “The context of people’s lives determines their health.”38
Multiple Levels and Examples of Key Contextual Factors
These multilevel contextual factors interact in complex ways to enhance or reduce health.39,40 Understanding and improving health and health care among persons with MCC therefore requires discerning which contextual factors are most relevant and ascertaining how these factors interact with each other to influence health or health care.41,42
Which contextual factors are most important varies with the person, time, and situation. This heterogeneity of contextual factors is a conceptual and research challenge that requires understanding the health and health care of persons with MCC as a complex system in which contextual factors coevolve with time.42–49 Although it may seem simpler to ignore multilevel contextual factors, a constricted, disease-specific focus risks making misattributions about cause, effect, and intervention points of leverage in the complex and adaptive system of persons living with MCC.48 Identifying and then considering the most relevant factors from the domains of context outlined in Table 1 at all stages of the research process, from conceptualization to actualization to implementation and dissemination, and, finally, acting on the resulting hypotheses and understanding are needed to make research both rigorous in truly understanding the complexity of MCC, and relevant in focusing on what is most important.
Advancing the Research Agenda
Goal 4 of the DHHS strategic framework for optimum health and quality of life for individuals with MCC is to “facilitate research to fill knowledge gaps about, and interventions and systems to benefit, individuals with MCC.”6 The strategic framework suggests 4 main objectives: “increase the external validity of trials; understand the epidemiology of MCC; increase clinical, community, and patient-centered health research; address disparities in MCC populations.”6 The objectives that focus on external validity, patient-centeredness, and equity are highly consistent with the research foci identified in this article. Other helpful previous research agendas for MCC50,51 have emphasized the medical context of the person.
Table 2 displays examples of important and context-based research questions that build on these agendas. These questions cluster around 2 important themes developed at the conference.
Advancing the Research Agenda
First is developing knowledge that moves beyond a disease-driven research agenda9 to support health- and person-driven,52 goal-directed53,54 therapeutic and prevention strategies55 for persons with MCC. This effort involves shifting perspective from generating knowledge relevant for “… making sure the evidence-based commodities of care are delivered for each disease…” to systematic knowledge useful for “…assuring that persons with multiple illnesses get health care that helps them get on with what is important in their life.” Relevant research questions include assessing specific contextual factors meaningful to different persons in different situations so that health care and health promotion can be focused on specific needs and goals.
The second theme relates to achieving the needed paradigm shift. The research questions here are about developing a culture, system, technology, and communities that facilitate person-driven, goal-directed care and self-management that improves health and well-being.
Methods for Generating the Needed New Knowledge
Because contextual factors change with time in ways that may affect outcomes,39,40 relevant contextual factors must be considered and assessed from conceptualization to completion and application of the research study. Methods need to be open to the possibility of emergence. They need to go beyond assumptions of linear effects and do more than assess central tendency. From a traditional clinical trials perspective, contextual factors would be considered as noise,56 as effect modifiers, or as confounding variables to be controlled or their effects made irrelevant through randomization.57–59 Decontextualized research methods, however, are a major reason why their findings are not translated into practice.60,61 They are not relevant to either patients or their clinicians.62–64
Considering context can cause diverse ontological and epistemological views of research, conceptual models, and analytic approaches to surface.65 Expanded research methods can be used to go beyond common reductionist conceptualizations to embrace new conceptual and computational models that include contextual factors.66 Methods that take context into account can help make sense of heterogeneity56 and of the frequent failure to replicate decontextualized studies in different settings.67–69 These methods can help to move beyond understanding what works on average to understanding what works for whom and in what situation.70,71
Table 3 lists current methodological challenges relevant to research on MCC and offers suggestions for contextualized research methods. This research requires methods that are participatory, multilevel, and flexible; are conducive to ongoing measurement from diverse (and sometimes innovative or novel) data sources, including existing data; assure study integrity; integrate quantitative and qualitative methods; and generate ongoing learning. In addition, consideration of relationship-centered principles,72,73 such as transparency and trustworthiness, responsiveness to concerns, early and consistent engagement, and openness to diverse perspectives, is necessary to ensure that research is informed by the perspectives of multiple stakeholders.74,75
Methods for Generating the Needed New Knowledge
These methods can contribute to a continuously learning health system76–78 that includes targeted populations, surrounding communities, and all stakeholders. The needed inclusive work is facilitated by developing a common lexicon across diverse stakeholders and by consistently requiring consideration of relevant contextual factors in funding proposals and journal reporting.79,80
Partnerships for Collaborative Action
The multilevel nature of contextual factors in MCC, along with the associated paradigm shift in research approach, requires partnership to generate, evaluate, and apply the needed new knowledge effectively in diverse settings and situations. Such collaborative action is consistent with recent calls by the NIH and others for team science81–83 and with the growing recognition of the need for multistakeholder partnerships to address complex multifactorial problems.49,84,85
Table 4 identifies suggested partners, domains in which their engagement is critical, and steps for their engagement. The changes required for research in MCC are both instrumental and part of a larger movement and political process; therefore, the requisite partnerships will also require a combination of incremental changes and movement toward a far-reaching, boundary-spanning86–88 new vision. Figure 2 depicts the necessary interactions across the spectrum of stakeholders generating the needed new knowledge, including payers and policy makers, community partners, patients and caregivers, the health care system, and research community.
Partnership for Collaborative Action
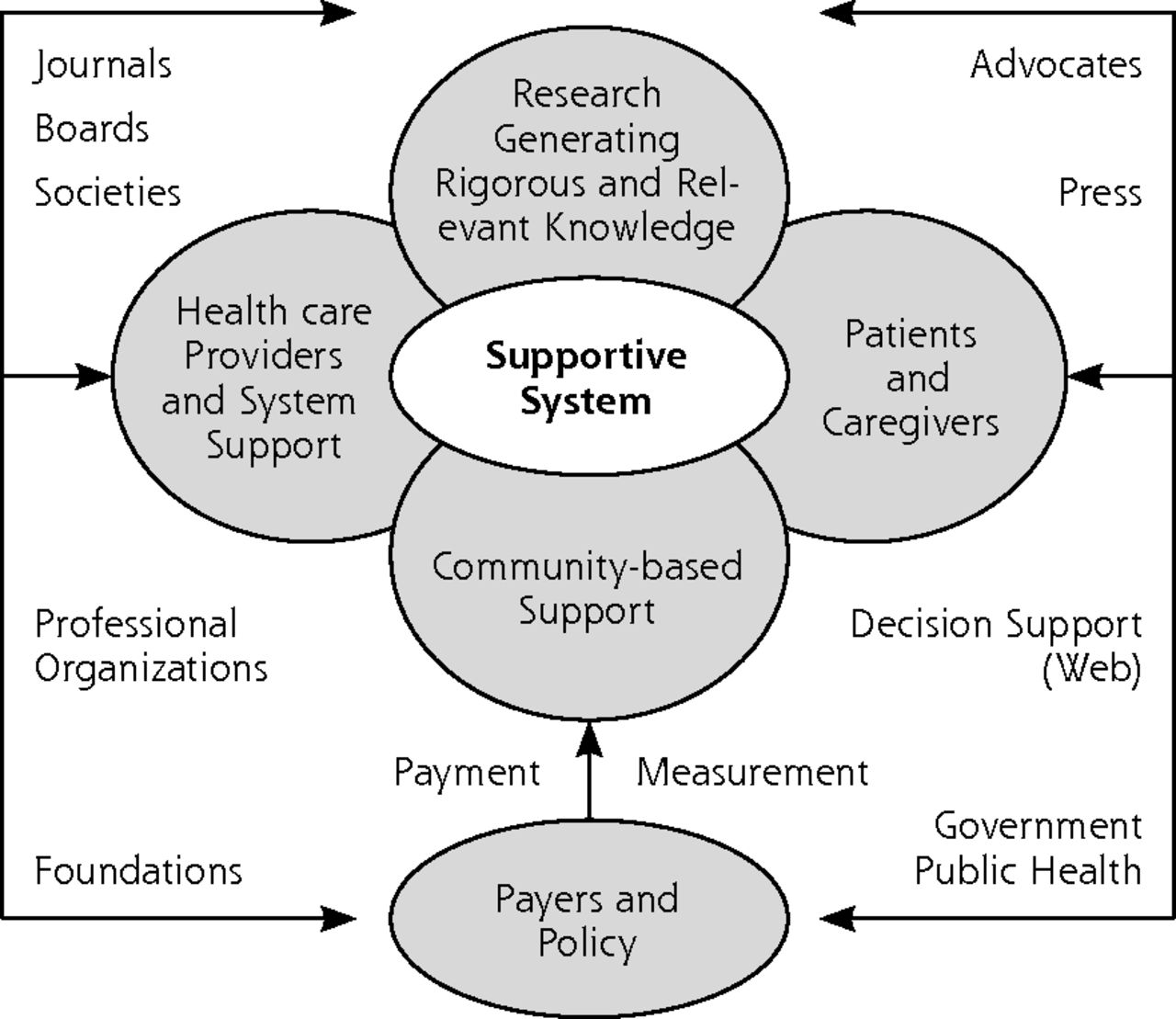
Partnerships for Collaborative Action
The DHHS strategic framework for managing MCC6 provides an important starting point for the needed collaborations, and it already has identified more than 250 programs, partners, and others working on aspects of the agenda.7 A more general framework for collaborative impact identifies 5 conditions of collective success: a common agenda, shared measurement systems, mutually reinforcing activities, continuous communication, and backbone supports.89 Using this framework, 5 short- to midterm recommendations emerge to support inclusion of key contextual factors in the initiatives:
-
Establish a measurement framework that includes a shared lexicon around priority contextual factors and indicators at the person, population, and system levels to monitor progress. The National Committee on Vital Health Statistics90 and the National Quality Forum91 would be logical homes for such efforts.
-
Build a national network of organizations interested in collecting and disseminating best practices in assessing and acting on context for persons with MCC. The national network would begin by identifying and building on current initiatives and identifying dissemination channels through which best practices can be shared.
-
Create a national public awareness campaign for consumers around key contextual factors. The campaign would build on emerging research and empower persons with MCC and their families to engage clinicians in contextual-based discussions that influence their care. (See the patient handout in the Supplemental Appendix.)
-
Activate and deploy a workforce that is skilled in incorporating context into research and practice. To do so will require the inclusion of contextualized understanding of MCC in the curriculum for health professionals and in training for early career scientists, as well as current researchers who need additional training in new methods and cross-cutting content.7
-
Develop a supportive policy environment. A broad-based coalition of private sector and government organizations is needed to think through policy options and help effect desirable policy changes as part of a long-term process of social change.
A longer term recommendation is to create an inventory and synthesis of interventions and best practices across all partner groups and convene a national-level entity (eg, an Institute of Medicine panel) to consider how contextual factors can be brought into research, implementation, and dissemination.
The fundamental premise among an emerging MCC-in-context collaborative is that government agencies, business, nonprofit organizations, and others can work together in a strategic, coordinated way to achieve ambitious societal goals focused on improving health and health care for those with multiple chronic illnesses while controlling health care costs.
DISCUSSION
Understanding contextual factors is vital to generating the new knowledge needed to improve the health of persons with MCC and to create a high-value health care system that is person-centered, goal-based, individualized, and sustainable. Such an effort will require a paradigm shift in how knowledge generation is understood and how research is conducted and implemented. The shift involves moving from a linear, reductionist view of the world to an understanding of the complexity of health and health care that is particularly apparent in persons with MCC.
The challenges to this work are substantial. Moving the research enterprise from a well-established and well-regarded reductionist approach that asks, “What is the matter?” to a research community that values context and asks, “What matters?” will require bold action by leaders within a research community supported and informed by persons with MCC, their family and friend caregivers, and clinicians. No group alone will be able to drive this movement forward. New coalitions and groups will need to form. Research and improvement efforts will need to be more congruent, so that contextualized knowledge generation and its application become part of the same learning community process.
New partnerships will involve researchers, clinicians, patients, caregivers, policy makers, and other stakeholders paying attention to contextual factors in generating questions, making observations, and doing interventions while continuing to learn during implementation, dissemination, and reinvention in new settings.92,93 New policy initiatives will involve the development of infrastructure and relationships for real-time shared learning in research and practice. Funders and journal editors40,79,94 can play a prominent role in calling for context to be included in the research that is needed to take the science to next step by more closely linking research, practice, and the lived experience of persons with MCCs.
A focus on incorporating the perspectives of key stakeholders in research, especially persons with MCC, resonates with the mission of the new Patient-Centered Outcomes Research Institute.95 It also aligns with the NIH focus on precision medicine96 that identifies key individual lever points to tailor interventions, as well as with growing initiatives around integrated care and care plans.32,54,97–99
The strengths of this report include findings generated by diverse stakeholder groups working together in an iterative process. Developing the working manuscript as a team provided an opportunity to bring together perspectives that are not usually apparent in the development of a research agenda, such as those of patients and family/friend caregivers, as well as community organizations and advocacy groups. The limitations of this article are that, despite its diversity, many stakeholders were not represented, and the results of our deliberations are only a first step in a large and diverse ongoing effort toward a more detailed blueprint for future action. Nevertheless, the meeting produced a set of principles for an ongoing inclusive process.
For those who have or who are at risk for MCC (which is almost everyone), developing an evidence base that includes context will ultimately lead to more integrated, effective, high value health care that is responsive to individual needs, preferences, and desires.
Acknowledgments
The authors are grateful to the Patient-Centered Outcomes Research Institute, which hosted our meeting. Anand Parekh, MD, MPH, and Robert Kaplan, PhD, made helpful framing comments at the outset of our meeting.
Footnotes
-
Conflicts of interest: authors report none.
-
Contributors and groups: Project and conference facilitators: Wendy J. Nilsen, PhD, Office of Behavioral and Social Sciences Research, National Institutes of Health, Bethesda, MD, and Kurt C. Stange, MD, PhD, Case Western Reserve University, Cleveland, OH.
-
Key contextual factors: Group leaders Elizabeth A. Bayliss, MD, MSPH, Kaiser Permanente, Denver, CO, and David Meyers, MD, Agency for Healthcare Research and Quality, Rockville, MD; Suzanne Mintz, Family Caregiver Advocacy, Kensington, MD; Josephine P. Briggs, MD, National Center for Complementary and Alternative Medicine, Bethesda, MD; Emily Dessem, National Council on Aging, Washington, DC; Giovanna Giuliani, MBA, MPH, California HealthCare Foundation, Oakland, CA; Shari Ling, MD, Center for Medicare and Medicaid Services, Baltimore, MD; Diane Meier, MD, Mt. Sinai Hospital, New York, NY; Steven Mintz, Patient/Caregiver Advocate, Kensington, MD; Joan D. Penrod, PhD, Centers for Medicare and Medicaid Services, Baltimore, MD; Michelle Washko, PhD, Center for Disability and Aging Policy, Administration for Community Living, Washington, DC.
-
Research methods: Group leader Denise E. Bonds, MD, MPH, National Heart, Lung and Blood Institute, Bethesda, MD, and Sally Okun, RN, MMHS, PatientsLikeMe, Cambridge, MA; Melinda M. Davis, PhD, Oregon Health & Sciences University, Portland, OR; Barbara L. Kornblau, JD, OTR, Patient/Caregiver Advocate, Washington, DC, and Florida A&M University, Tallahassee, FL; Emmanuelle St. Jean, National Council on Aging, Washington, DC.
-
Research agenda: Group leaders Cynthia M. Boyd, MD, MPH, Johns Hopkins University School of Medicine and Bloomberg School of Public Health, Baltimore, MD, and Marcel E. Salive, MD, MPH, National Institute on Aging/NIH, Bethesda, MD; Michael H. Fox, ScD, Center for Disease Control and Prevention, Atlanta, GA; Russell Glasgow, PhD, National Cancer Institute, Bethesda, MD, and University of Colorado School of Medicine, Denver, CO; Suzanne Heurtin-Roberts, PhD, National Cancer Institute, Bethesda, MD; Sue Lachenmayr, MPH, CHES, National Council on Aging, Washington, DC; Catherine Alfano, PhD, National Cancer Institute, Bethesda, MD; Lisa A. Cooper MD, MPH, Johns Hopkins University School of Medicine and Bloomberg School of Public Health, Baltimore, MD; Marisa Elena Domino, PhD, UNC Chapel Hill, Chapel Hill, NC; Robert Hornyak, MS, Administration on Community Living, Washington, DC; Lisa LeRoy, MBA, PhD, Abt Associates, Cambridge, MA; Alicia Richmond Scott, MSW, Office of the Assistant Secretary for Health, Department of Health and Human Services, Rockville, MD; Mary Tinetti, MD, Yale University, New Haven, CT.
-
Collaborative action: Group leaders Richard Goodman, MD, MPH, Office of the Assistant Secretary for Health, Department of Health and Human Services, and Center for Disease Control and Prevention, Atlanta, GA, and Sarah Ruiz, PhD, National Council on Aging, Washington, DC; Bruce Fink, MD, Indian Health Services, Nashville, TN, and Baltimore, MD; Cristin Lind, Patient/Caregiver Advocate, Boston, MA (currently at the Karolinska Institutet, Stockholm, Sweden); Elizabeth A. Madigan, PhD, RN, FAAN, Case Western Reserve University, Cleveland, OH; Anne Beal, MD, MPH, Patient-Center Outcomes Research Institute, Washington, DC; Caroline Blaum, MD, MS, NYU Langone Medical Center, New York, NY; Gail Hunt, National Alliance for Caregiving-PCORI Board, Bethesda, MD; Keith Lind, JD, AARP, Washington, DC; Leon Purnell, Patient/Caregiver Advocate, Washington, DC; Joe Selby, MD, MPH, Patient-Center Outcomes Research Institute, Washington, DC; Michelle Spafford, National Council on Aging, Washington, DC.
-
Funding support: Dr Stange’s time is supported in part by a Clinical Research Professorship from the American Cancer Society and by the National Cancer Society through the Intergovernmental Personnel Act.
-
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily reflect the official position of the Centers for Disease Control and Prevention, National Institutes for Health, Agency for Healthcare Research and Quality, federal agencies, or other organizations of the authors or persons named in the above contributor groups.
-
Supplementary materials: Available at http://www.AnnFamMed.org/content/12/3/260/suppl/DC1/
- Received for publication August 6, 2013.
- Revision received December 24, 2013.
- Accepted for publication January 30, 2014.
- © 2014 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Protocol of the pilot study to test and evaluate the iCARE tool: a machine learning-based e-platform tool to make health prognoses and support decision-making for the care of older persons with complex chronic conditions
- Building on the past: how historical research can contribute to our understanding of the spaces of general practice
- Managing Multiple Chronic Conditions during COVID-19 Among Patients with Social Health Risks
- Impact of primary care usual provider type and provider interdependence on outcomes for patients with diabetes: a cohort study
- Magnitude, pattern and correlates of multimorbidity among patients attending chronic outpatient medical care in Bahir Dar, northwest Ethiopia: the application of latent class analysis model
- Changing Reasons for Visiting Primary Care Over a 35-Year Period
- Guideline deviation and its association with specific chronic diseases among patients with multimorbidity: a cross-sectional cohort study in a care management setting
- Cancer Survivorship Care Roles for Primary Care Physicians
- Multimorbidity of chronic non-communicable diseases and its models of care in low- and middle-income countries: a scoping review protocol
- Health-related preferences of older patients with multimorbidity: the protocol for an evidence map
- Experiences of community-dwelling older adults living with multiple chronic conditions: a qualitative study
- Multimorbidity in Older Adults With Cardiovascular Disease
- Managing Complexity in Older Patients with CKD
- Comparison of count-based multimorbidity measures in predicting emergency admission and functional decline in older community-dwelling adults: a prospective cohort study
- Capturing the experiences of patients across multiple complex interventions: a meta-qualitative approach
- A Participatory Model of the Paradox of Primary Care
- The relationship of individual comorbid chronic conditions to diabetes care quality
- Why do patients with multimorbidity in England report worse experiences in primary care? Evidence from the General Practice Patient Survey
- What to give the patient who has everything? A qualitative study of prescribing for multimorbidity in primary care
- AHA/ACC/HHS Strategies to Enhance Application of Clinical Practice Guidelines in Patients With Cardiovascular Disease and Comorbid Conditions: From the American Heart Association, American College of Cardiology, and US Department of Health and Human Services
- AHA/ACC/HHS Strategies to Enhance Application of Clinical Practice Guidelines in Patients With Cardiovascular Disease and Comorbid Conditions: From the American Heart Association, American College of Cardiology, and U.S. Department of Health and Human Services
- On-the-Ground Wisdom About Care Integration
- In This Issue: Many Arrows Rather than Magic Bullets
- IOM and DHHS Meeting on Making Clinical Practice Guidelines Appropriate for Patients with Multiple Chronic Conditions